● INTRODUCTION
Despite the advent of sophisticated ultrasound devices and tools in the last several years, the basic examination of the fetal heart is still best performed with two-dimensional (2D) grayscale (B-mode) ultrasound. Visualization of fetal situs, the cardiac chambers, the origin and course of the great vessels, and surrounding organs can be accurately performed with 2D ultrasonography. The quality of the 2D ultrasound image is dependent on several factors, including the choice of the transducer and presets, the angle of insonation and access to the region of interest, and magnification of the target region. In this chapter, we explain the practical aspects of the 2D grayscale ultrasound image optimization as it relates to the fetal heart.
● CHOICE OF TRANSDUCER
Ultrasound companies offer a wide range of transducers, similar to the choice of lenses in professional photography. Many examiners consistently use one or two preferred transducers, which provide good images in the majority of patients. Most obstetric transducers are curved array with a frequency range of 2 to 8 MHz (1). In general, two groups of transducers are used in transabdominal obstetric scanning: low-frequency range (2–5 MHz) (Fig. 11.1A), which allows for good penetration of sound and acceptable resolution; and high-frequency range (5–8 MHz) (Fig. 11.1B), which allows for improved resolution but with limited sound penetration.
Recently, linear transducers that are commonly used for soft tissue imaging in radiology have been adapted to obstetric imaging (2, 3). These linear transducers are desirable because of their high resolution and thus are primarily used in the first trimester or when detailed anatomic information is needed (Fig. 11.2A). Unlike the curved array transducers, the linear transducers have ultrasound beams that are uniform throughout all tissue levels and do not diverge in deeper tissue (2, 3). When abdominal scanning of the fetal heart is suboptimal in the first and early second trimesters of pregnancy, a transvaginal transducer can be used (Fig. 11.2B). The main advantage of the transvaginal approach is the short distance to the region of interest (heart) with less maternal tissue between the transducer and the fetal heart, allowing for the use of higher frequency with better resolution.
● IMAGE PRESET
Harmonic Imaging
In the last decade, ultrasound manufacturers have introduced high-frequency transducers in order to improve image resolution. Limitations of high-frequency transducers include reduced tissue penetration and decreased resolution for deep pelvic structures. Harmonic imaging was also introduced to enhance visualization and reduce artifact (4, 5). In harmonic imaging, the transducer sends and receives signals at two different ultrasound frequencies (4, 5). This results in an improved image and contrast with reduced artifact because the reflected harmonic wave has a lower amplitude and higher frequency (twice the original) than the fundamental wave. Harmonic imaging is especially useful for structures with tissue–fluid interface, such as the heart (Fig. 11.3).
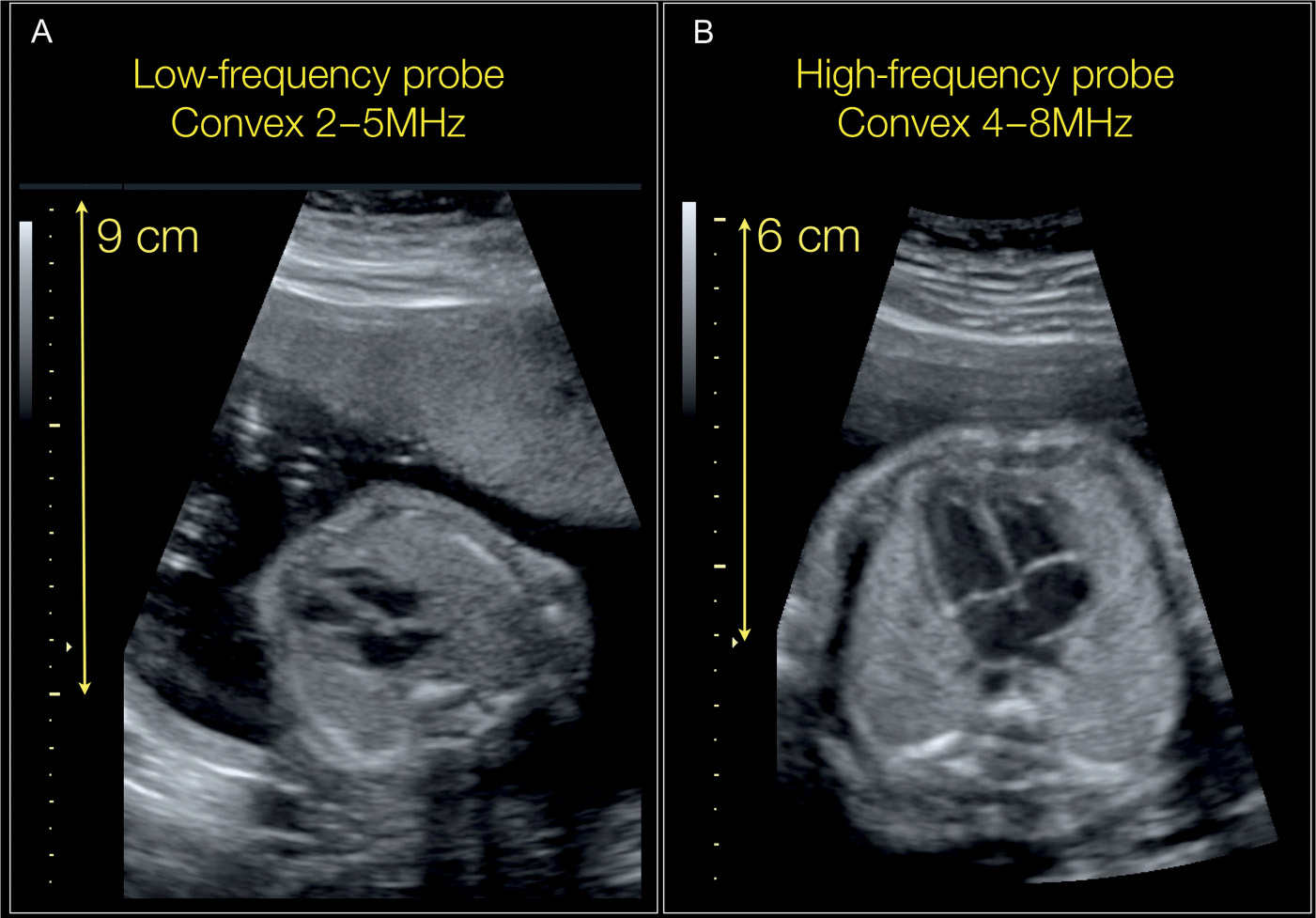
Figure 11.1: Four-chamber views of the fetal heart in two fetuses A and B imaged with two different ultrasound transducers. In fetus A, a 2- to 5-MHz transducer is used. The fetus in A lies deep in the pelvis due to increased maternal body habitus and an anterior placenta. The use of low-frequency transducer in A allows for deep penetration but with reduced resolution. In fetus B, a 4- to 8-MHz transducer is used as the fetal heart lies in a more superficial position in the pelvis than fetus A. The use of a high-frequency transducer in B allows for enhanced resolution.
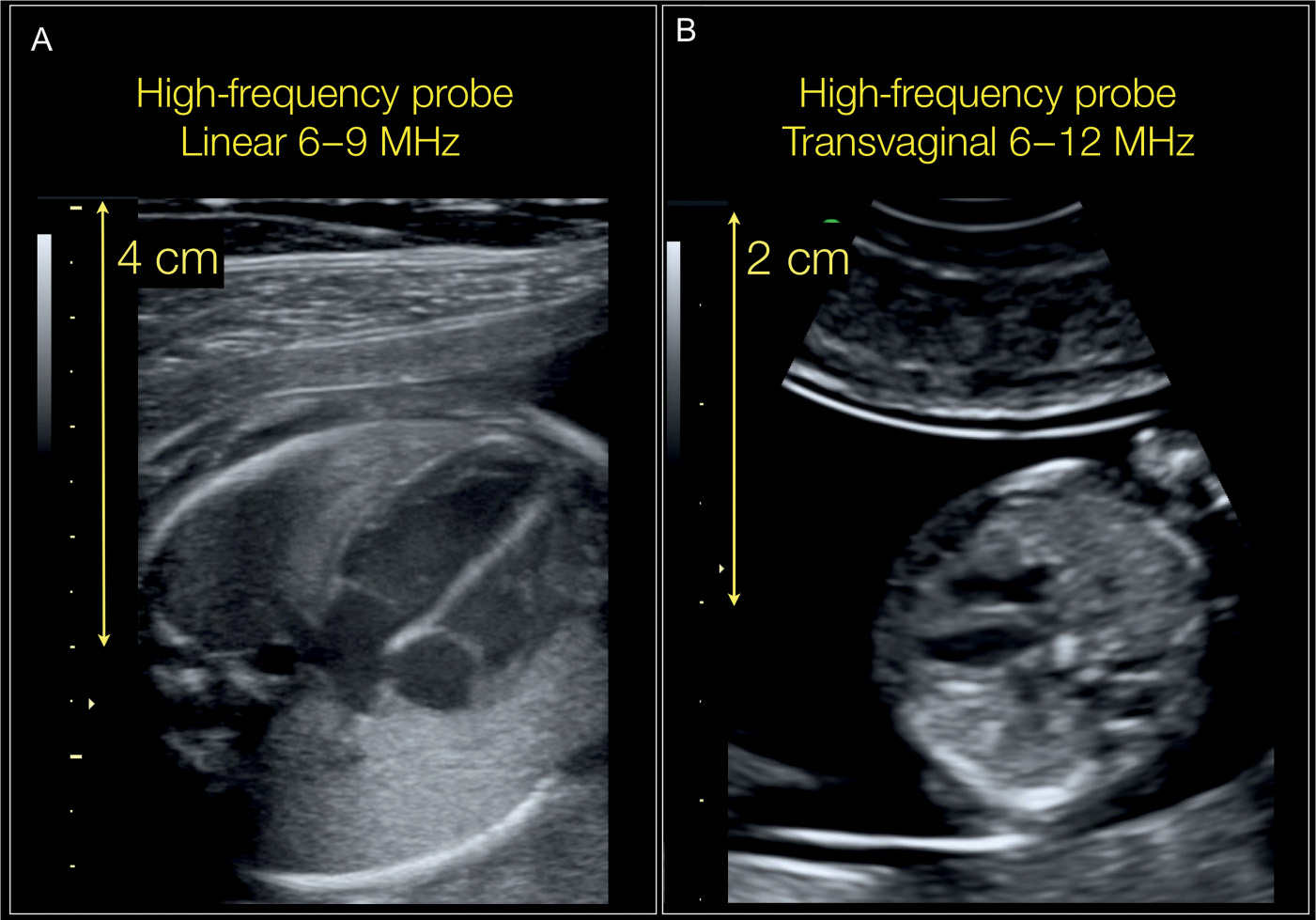
Figure 11.2: Four-chamber views of the fetal heart in two fetuses A and B examined with two different ultrasound transducers. In fetus A, a high-frequency linear probe (6–9 MHz) is used, which allowed for excellent resolution (improved over Fig. 11.1B). This high-frequency transducer provides optimal images for a relatively short depth range. In fetus B, a transvaginal transducer with a 6- to 12-MHz range is used, which provides excellent resolution for cardiac scanning in early gestation.
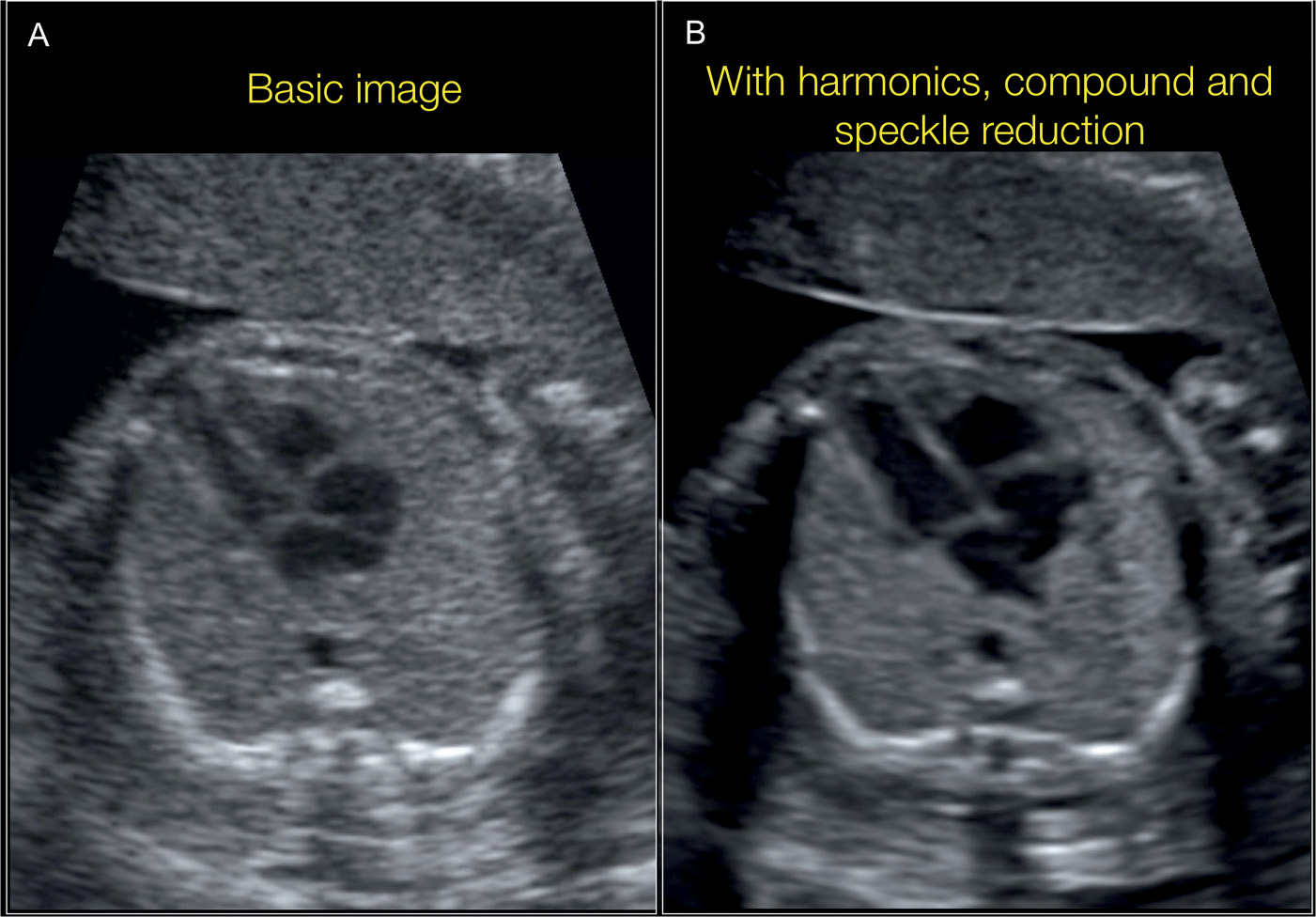
Figure 11.3: Four-chamber views of the fetal heart in the same fetus demonstrated in A with basic ultrasound presets and in B by the addition of harmonic and compound imaging and speckle reduction filter. Note the enhanced visualization of cardiac structures in B.
Compound Imaging
Compound imaging technology involves combining several (three or more) images from different steering angles of the transducer into a single image (6). Traditionally, transducers send ultrasound signals in a single line that is perpendicular to the transducer’s footprint. Compound imaging allows the transducer to send signals at multiple angles, allowing it to eliminate artifact and improve resolution (6) (Fig. 11.3).
Speckle Reduction Imaging
Speckle reduction imaging is a technique that uses an algorithm to stratify strong and weak ultrasound signals. By doing so, reflected weak signals, termed speckle, are eliminated whereas strong signals are enhanced and brightened (6). This allows the image to become smoother and reduces artifact. Figure 11.3 shows a heart with and without speckle reduction imaging in addition to compound imaging.
Focal Zone(s)
In ultrasound imaging, the focal zone represents the region in the display where the sound beam is most sharply focused, thus resulting in the most optimal image. Modern phased array transducers and many linear array transducers allow the operator to select the focal zone distance by applying specific timing delays between transducer elements that cause the beam to converge at a specified distance. When multiple focal zones are applied during scanning, the transducer array elements acquire data repeatedly with different phase timing (6). This repeated acquisition results in a slower frame rate due to time delay. The focal zones should always be placed at the depth of interest on the ultrasound image in order to ensure the best possible lateral resolution. When imaging the heart, it is recommended to choose one focal zone at the region of interest. Although choosing multiple focal zones can maximize lateral resolution over depth, this, however, will result in a slower frame rate, which makes imaging of the fetal heart suboptimal (6). Figures 11.4 and 11.5 show the optimal placement of the focal zone when the fetal heart is imaged.
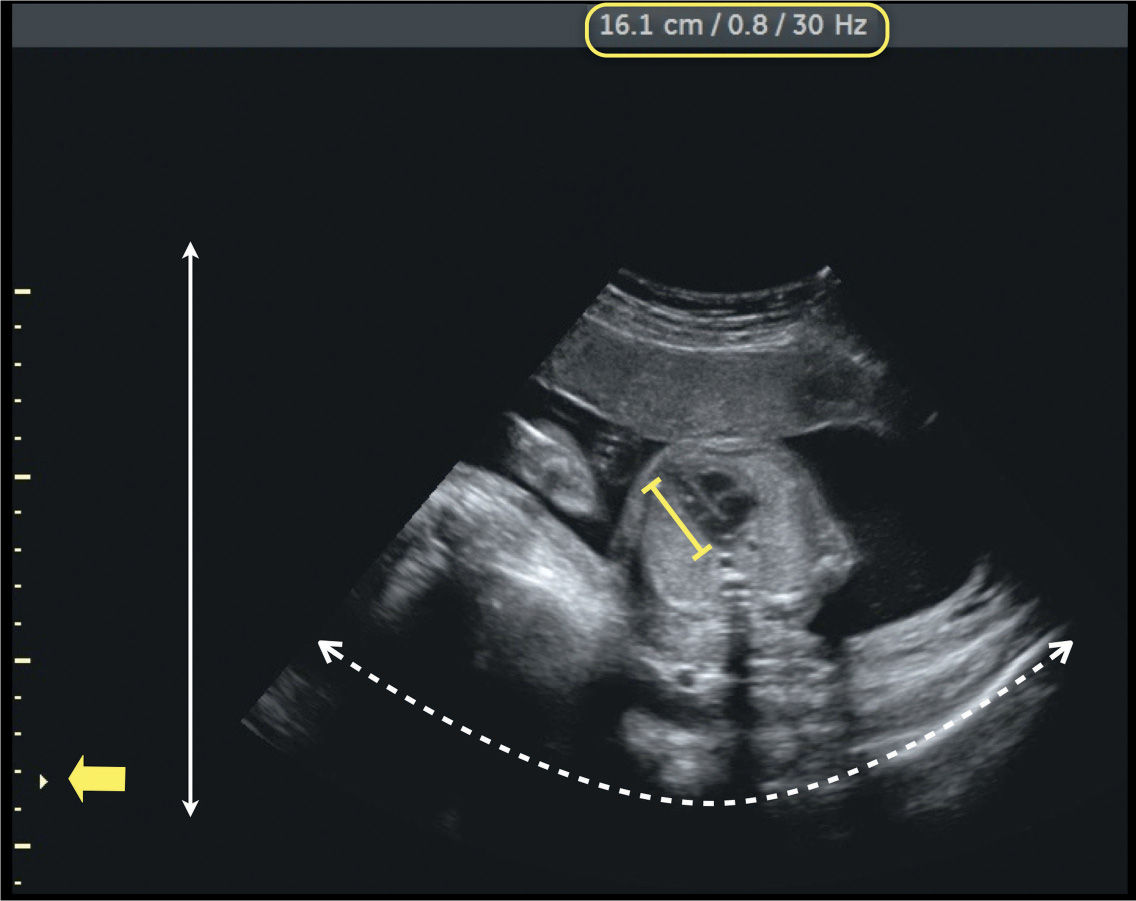
Figure 11.4: Four-chamber view of the fetal heart obtained without image optimization. Note that the depth is high (double straight arrow), the angle is wide (dashed arrow), and the focal zone (yellow arrow) is not placed at the level of the region of interest (four-chamber view). The size of the heart within the whole image (yellow line) is so small that it does not allow for any reliable detailed analysis. The information provided in the yellow box shows a depth of 16.1 cm, a magnification of 0.8, and a frame rate of 30 Hz. Compare with Figure 11.5 of the same fetus following image optimization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


