● INTRODUCTION
Color and pulsed Doppler ultrasound was introduced to clinical practice about two decades ago, and its clinical application in fetal echocardiography was quickly accepted (1–8). Color and pulsed Doppler ultrasound is currently available on almost all mid- and high-end ultrasound equipment involved in obstetric sonography. When imaging the fetal heart on ultrasound, some examiners recommend limiting the use of color Doppler to high-risk conditions such as the presence of a suspected anatomic or functional cardiac abnormality. Other examiners recommend the routine use of color Doppler as an integral component of fetal cardiac screening in every fetus, arguing that its routine use increases both the accuracy and speed of the examination (9, 10). There is general agreement, however, that when the fetal heart is examined in detail as part of a fetal echocardiogram, the routine application of color Doppler is warranted. In a consensus statement, the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) stated that color Doppler ultrasonography is an important component of the fetal echocardiogram and recommended its mandatory use in that setting and that the additional use of power Doppler is optional (11). ISUOG screening cardiac guidelines (12) also state that color Doppler ultrasonography should be used in routine cardiac screening if the examiner feels confident in using it.
We recommend the liberal use of color Doppler in the ultrasound examination of the fetal heart and that color Doppler should be part of fetal echocardiography. It is the author’s opinion that routine use of color Doppler makes the examiner more confident with this technique and improves its accurate and reliable use in difficult scanning conditions once an abnormal finding is suspected.
In this book, the use of color Doppler as it pertains to the diagnosis of cardiac malformations is described in the respective chapters on cardiac anomalies. Table 12.1 summarizes the clinical information that can be provided by color Doppler in normal and abnormal hearts. This chapter will focus on the optimization of color Doppler in fetal cardiac imaging and on the targeted anatomic cardiac planes evaluated by color Doppler ultrasonography.
● PRINCIPLE OF COLOR DOPPLER, POWER DOPPLER, AND HIGH-DEFINITION COLOR DOPPLER
Color Doppler ultrasound consists of the detection of flow velocity patterns in real-time and it is superimposed on the display of the two-dimensional grayscale image of the anatomic structures where the flow occurs (Fig. 12.1A and B). Color Doppler ultrasound utilizes the frequency shift generated by the velocity of flow of the red blood cells within a vessel to generate the image. The display of flow patterns is color-coded, which allows the demonstration of a variety of hemodynamic information of the velocities measured. Color Doppler is based on the assessment of the mean velocities during the time event and does not provide information on peak velocities. The visualization is thus qualitative or semiquantitative, and the true measurement of peak or mean velocities can only be achieved by spectral Doppler interrogation of the region of interest (see Chapter 13). The mean frequency shift estimated in color Doppler is dependent on the angle of insonation of the ultrasound beam with the direction of flow within the vessel, which creates a major limitation, especially when vascular structures are imaged at an increased angle to the direction of flow (13).
Information from color Doppler | Clinical impact |
Demonstration of presence of blood flow (yes/no) | Presence or absence of blood flow over a region of interest (e.g., perfusion across an “atretic” or dysplastic valve) Better demonstration of small structures (e.g., narrow pulmonary artery, shunt over a detected VSD) Identification of cardiac structures in early gestation |
Demonstration of direction of blood flow (antegrade/retrograde) | Demonstration of antegrade or retrograde flow in the aortic arch, in the pulmonary artery, across the ductus arteriosus, across the foramen ovale, in a left superior vena cava or a confluent vein, etc. |
Detection of unexpected blood flow events (laminar flow versus turbulent flow, etc.) | Detection of shunting across a small VSD, regurgitation across the tricuspid valve, turbulent flow across the aorta or the pulmonary artery with valve stenosis, detection of ventriculo-coronary fistula in pulmonary atresia |
Demonstration of small vessels | Pulmonary veins, peripheral pulmonary arteries, anomalous tortuous ductus arteriosus, abnormal vessels such as MAPCAs, LSVC, dilated azygos vein, etc. |
Optimizing placement of the sample volume for spectral Doppler evaluation | Stenosis or regurgitation of a valve, Doppler of small vessels, Doppler of fetal veins (ductus venosus, pulmonary veins, inferior vena cava, azygos vein, abnormal draining pulmonary veins) |
VSD, ventricular septal defect; MAPCAs, major aortopulmonary collateral arteries; LSVC, left superior vena cava.
In the other color-coded display called power Doppler, the intensity or amplitude of the Doppler signal is assessed instead of the velocities. The amplitude of the Doppler signal is generated by the signal intensity of the red blood cells within a vessel, which is almost independent of the angle of insonation (Fig. 12.1C). Power Doppler has therefore several advantages over conventional color Doppler. Enhanced sensitivity: Since the amplitude of Doppler signals is analyzed instead of their frequency shift, power Doppler is shown to be three to five times more sensitive than conventional color Doppler in visualizing small vessels and low flow patterns. Improved noise differentiation: In power Doppler, noise signals are encoded in a uniform color (Fig. 12.1C). Hence, it is possible to turn the gain all the way up, which fills the entire image with noise, and the vascular signal will still be distinguishable. Enhanced edge definition: Power Doppler has better edge definition when displaying flow. This is because color signals, which extend partially beyond the edges, have lower signal amplitude due to the lack of moving erythrocytes and are thus not displayed. Flow detection irrespective of angle of insonation (Fig. 12.1C, white arrow): Power Doppler is able to detect flow at right angles to the beam. The amplitudes of the positive and negative components of the flow tend to add up, resulting in a powerful signal. Disadvantages of power Doppler when compared to conventional color Doppler include the lack of information on the direction of blood flow and the inability to demonstrate the presence or absence of turbulence.
By combining the Doppler frequency shifts with signal amplitude, digital broadband assessment of Doppler signals is applied, providing a very sensitive tool known as advanced dynamic flow (14) or high-definition (HD) color or flow (Fig. 12.1D). This technique has been shown to be superior to conventional color Doppler as it demonstrates higher resolution, good lateral discrimination, and higher sensitivity (14). The combination of color Doppler and HD or power Doppler has been shown to be effective in the appropriate evaluation of hemodynamic changes under normal and abnormal conditions. Figure 12.1 shows the aortic arch on gray scale, color Doppler, power Doppler, and HD flow. HD flow color maps can be chosen by the examiner either as a bidirectional color flow map or as a uniform color.
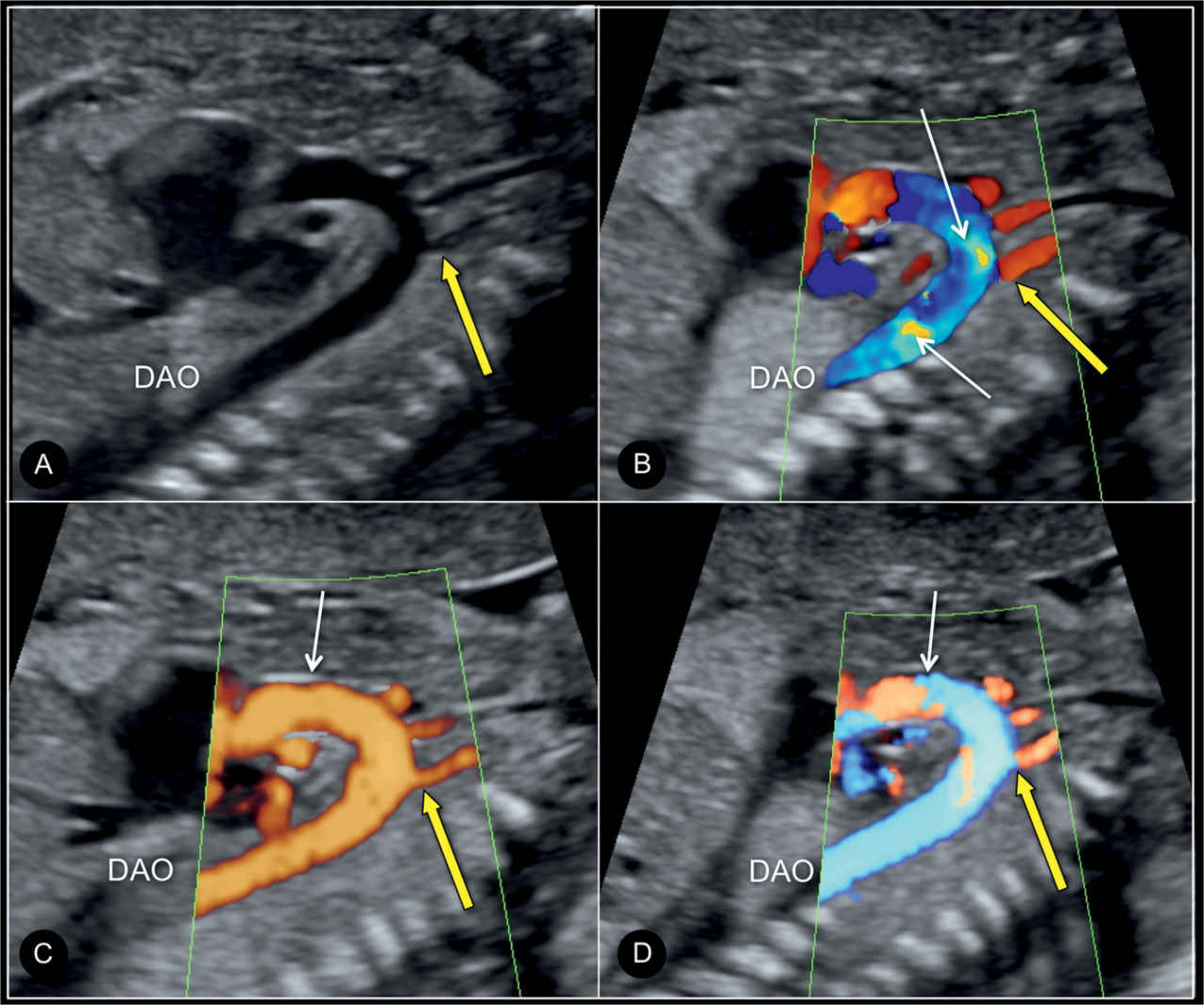
Figure 12.1: Parasagittal view of the aortic arch with the brachiocephalic arteries (yellow arrow) on grayscale (A), (conventional) color Doppler (B), power Doppler (C), and bidirectional high-definition flow (D). In B, displaying the brachiocephalic arteries can be achieved only by reducing the pulse repetition frequency, which leads to aliasing artifact within the aortic arch (white arrows). In C, power Doppler shows uniform, laminar and well-defined filling of the aortic arch (arrow) and brachiocephalic arteries. In D, high-definition flow demonstrates the most optimal display of the aortic arch (arrow) and great vessels with clear borders and uniform filling. DAO, descending aorta.
Additional advantages of various color Doppler displays are their application in the reconstruction of three-dimensional (3D) volumes (13, 15) in combination with static 3D, STIC (spatio-temporal image correlation), or live 3D, especially with matrix transducers (see Chapter 15 for more information on 3D).
● OPTIMIZING COLOR DOPPLER FOR THE FETAL CARDIAC EXAMINATION
Color Doppler examination of the fetal heart is enhanced when the proper settings of the ultrasound equipment are applied. The examiner should familiarize himself or herself with the standard features of the ultrasound equipment prior to the application of color Doppler. Improper use of color Doppler in the cardiac ultrasound examination may lead to false-negative or false-positive diagnoses. Steps in the optimization of the color Doppler ultrasound image in the fetal cardiac examination are hereby discussed.
Size of the Color Box
The optimum color Doppler image is a compromise between its quality and its frame rate. The color box, when activated, slows the frame rate of the ultrasound examination to a significant degree. When examining the fetal heart with color Doppler, a rapid frame rate with an acceptable image quality is essential given the small and complex anatomy of the fetal heart and its rapid rate in utero. We recommend choosing the smallest color box possible to maintain the frame rate as high as possible (Figs. 12.2 and 12.3). Frame rates greater than 20 to 25 frames/s are perceived by the human eye as “real time.” The image quality can be improved further by optimizing the use of the velocity scale, the wall filter, the persistence, the gain, and color line density.
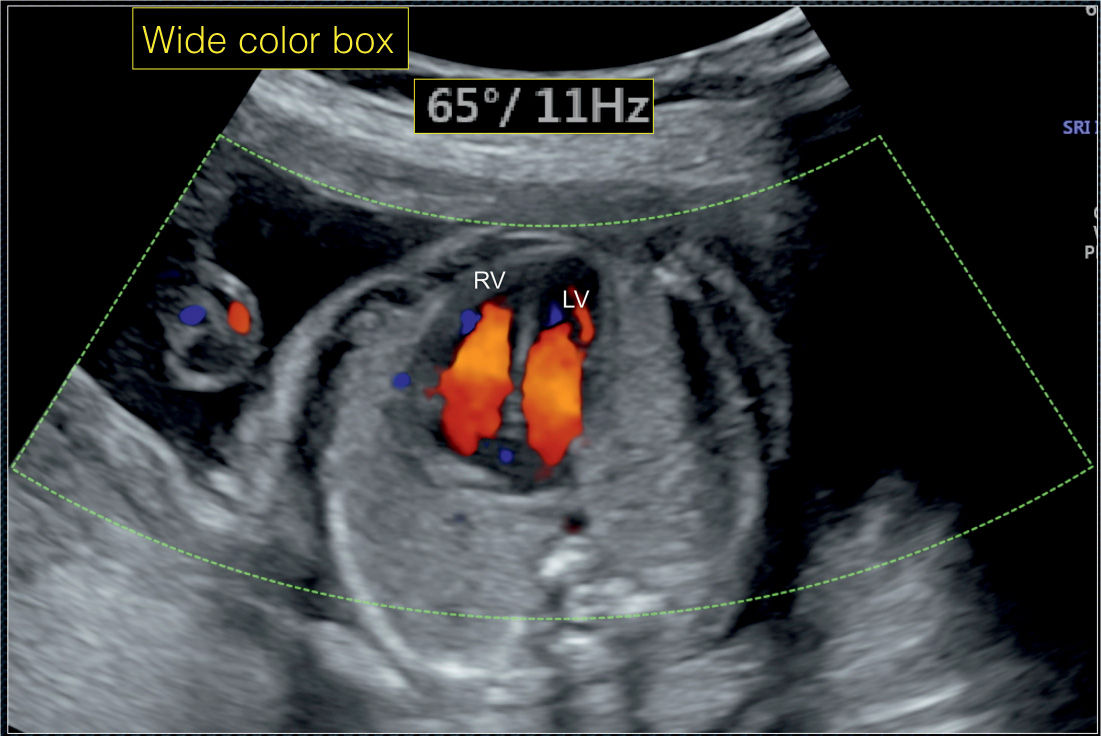
Figure 12.2: Apical four-chamber view of the fetal heart with color Doppler. A large color box is chosen (65 degrees), which results in a slow frame rate of 11 Hz (11 frames/s). A slow frame rate impedes visualization of the fetal heart on color Doppler. Compare with Figure 12.3. LV, left ventricle; RV, right ventricle.
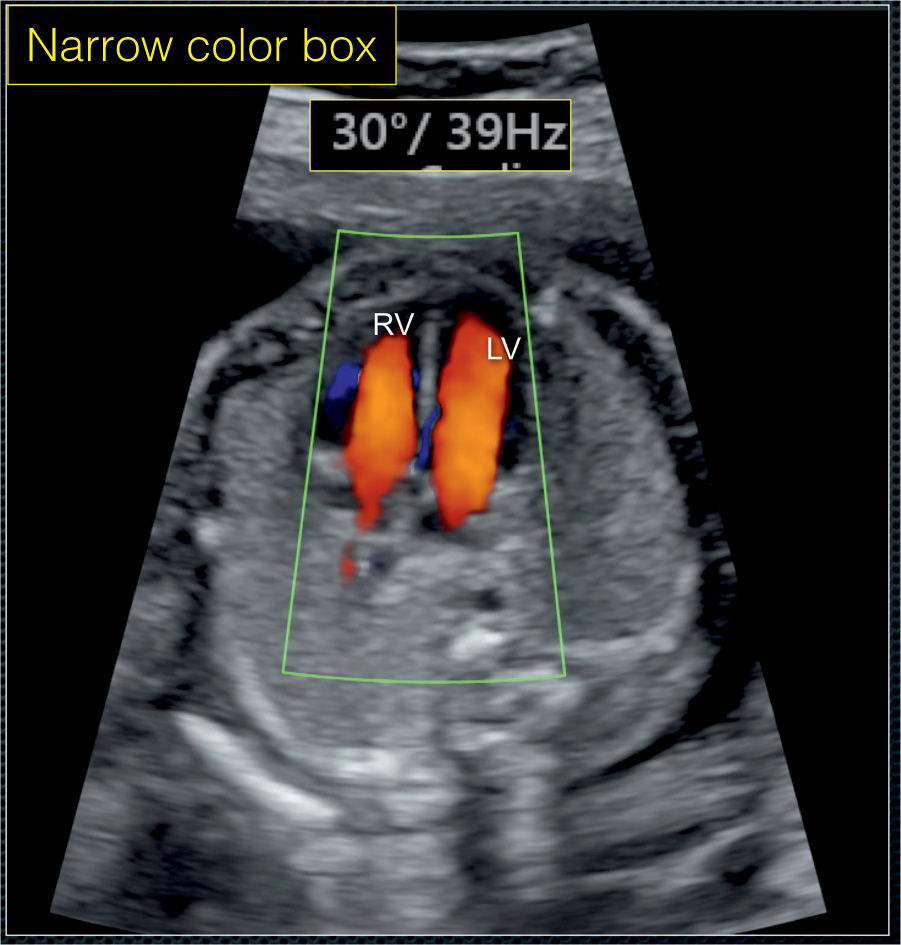
Figure 12.3: Apical four-chamber view of the fetal heart with color Doppler in the same fetus as in Figure 12.2. An appropriate size color box is chosen (30 degrees), wide enough to cover the fetal heart. This results in an improved frame rate of 39 Hz (39 frames/s). Compare with Figure 12.2. LV, left ventricle; RV, right ventricle.
Velocity Scale
Velocity scale or pulse repetition frequency is used to determine the range of mean velocities in the region of interest or within the color box. For color Doppler interrogation of the atrioventricular valves, the semilunar valves, and the great vessels, high-velocity range (>±30 cm/s) is selected. Figure 12.4A shows an improper use of low-velocity scale color setting resulting in aliased colors, which gives the impression of “turbulence” within the cardiac chambers. Increasing the color velocity scale to the appropriate level, as shown in Figure 12.4B, enhances the image quality. Low- to mid-velocity scales, in the order of 10 to 20 cm/s, are suitable for the pulmonary and caval veins given their low-velocity flow.
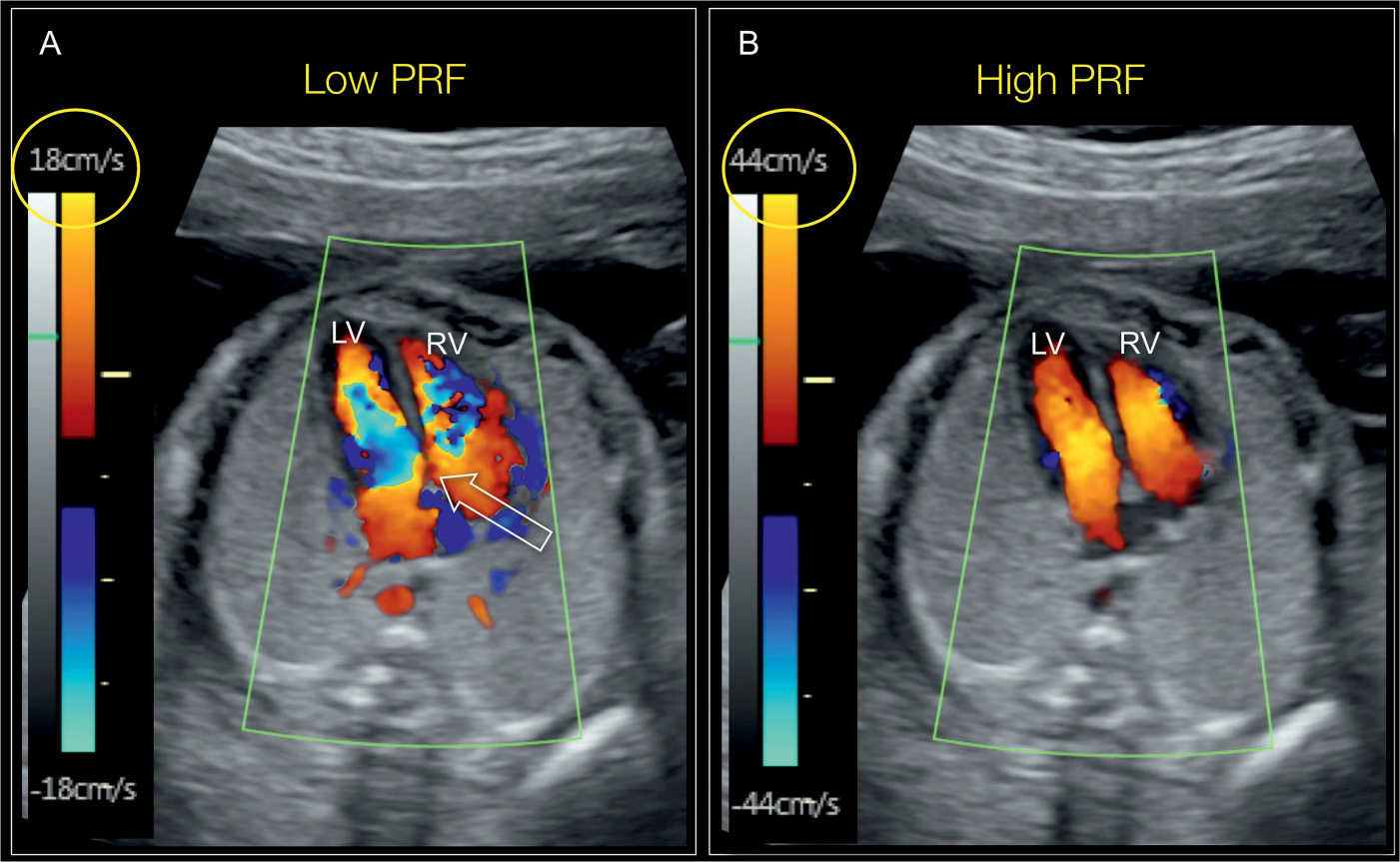
Figure 12.4: Apical four-chamber view of the fetal heart with color Doppler showing the effect of velocity scale (pulse repetition frequency [PRF]) on the display of color Doppler. In A, a low color Doppler velocity scale is chosen (18 cm/s), resulting in color aliasing of blood flow across the atrioventricular valves, thus mimicking flow turbulence (open arrow). In B, the color velocity scale is appropriately chosen (44 cm/s), resulting in optimal display of blood flow across the atrioventricular valves in diastole. LV, left ventricle; RV, right ventricle.
Color Filter
Color filter allows for the elimination of signals from wall motion and other low velocities. A high filter should therefore be selected for the color evaluation of the atrioventricular valves and flow across the great vessels, and a low color filter should be used for the evaluation of the pulmonary and systemic veins given their lower flow settings.
Color Persistence
Color persistence allows information from prior images to be overlapped on the current image, superimposing color signals from different phases of the cardiac cycle and thus reducing the impression of pulsation. Low color persistence settings should be generally selected for fetal cardiac assessment.
Color Gain
Color gain demonstrates the amount of color exhibited on the screen, similar to the grayscale gain function. Artifacts occur when the color gain setting is too high in fetal cardiac imaging (Fig. 12.5A and B). Gain settings in the midrange may also lead to superimposition of color over the border of a structure of interest, particularly when the atrioventricular valves are examined, giving the false impression of a septal defect. The color gain in cardiac imaging should therefore be initially set on low and gradually increased until the color information is optimized.
Color Doppler Image Resolution and Color Line Density
Color Doppler image resolution is related to the axial and lateral resolution as it relates to the number of color Doppler lines and sample volumes within the chosen color box. An increase in color resolution results in a slow frame rate. A compromise should therefore be sought between the color image quality and frame rate. We opt for a high color resolution when peripheral pulmonary vessels are imaged or in fetal echocardiography in early gestation in which the region of interest (color box) is usually small. The smallest color box is chosen in both these conditions in order to get the highest frame rate possible.
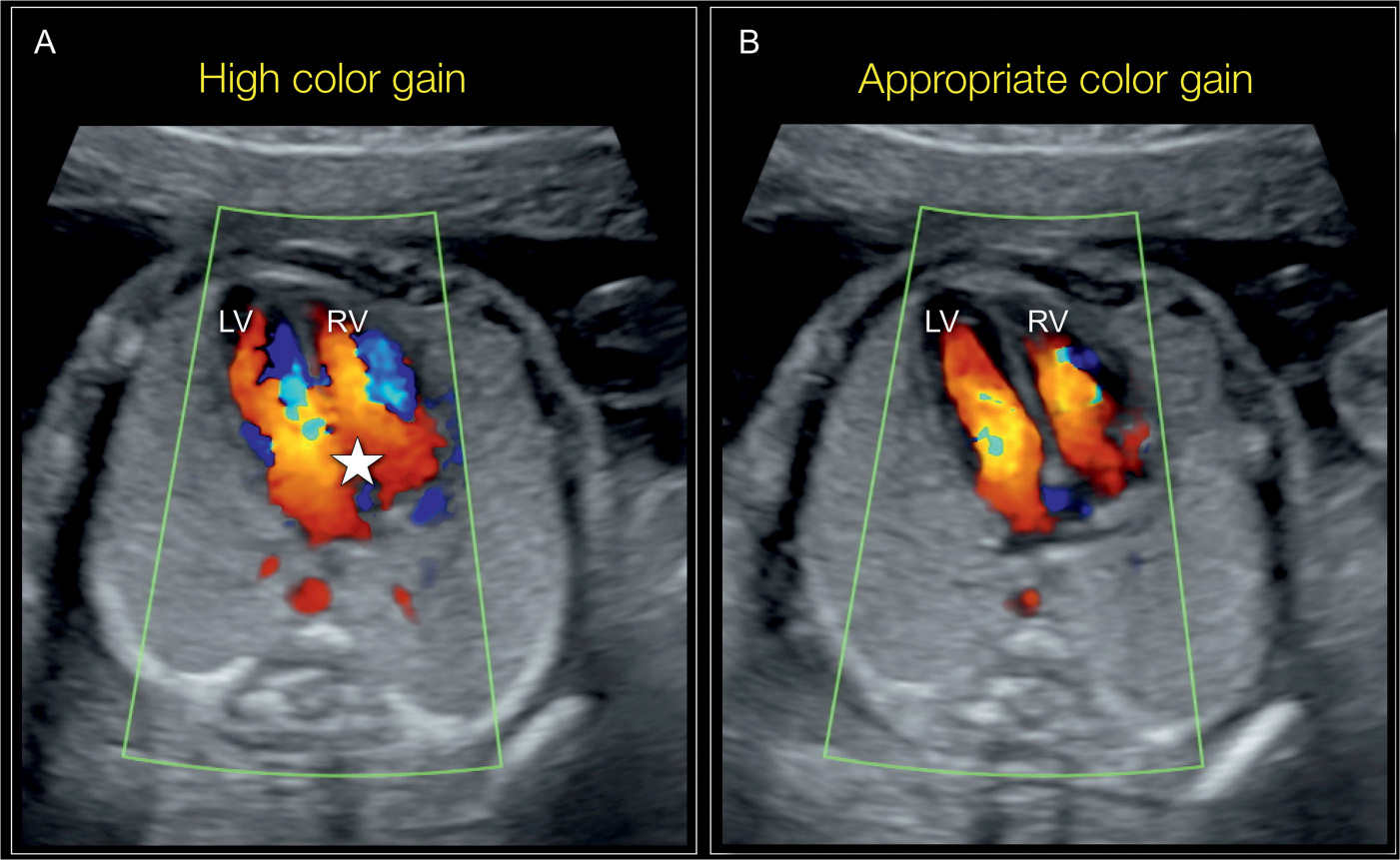
Figure 12.5: Apical four-chamber view of the fetal heart with color Doppler showing the effect of color gain on the display of color Doppler. In A, a high-gain setting is chosen, resulting in color overlap over the septum, mimicking the presence of an atrioventricular septal defect (star). In B, an appropriate color gain setting is chosen, resulting in optimal display of color flow across the atrioventricular valves during diastole. LV, left ventricle; RV, right ventricle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


