● INTRODUCTION
The first step in the ultrasonographic evaluation of the fetus is the assessment of fetal visceral situs as some organs are arranged symmetrically and others, such as the abdominal and thoracic organs, are arranged asymmetrically (1). A clear definition of left and right sidedness in the body is noted since early embryogenesis. A good understanding of fetal situs is important during ultrasound examinations, as some fetal anomalies are associated with abnormal laterality of abdominal and/or thoracic organs. Evaluating the orientation and position of the fetal heart in the thorax and the anatomic relationship of the abdominal organs is part of the targeted fetal cardiac examination. Knowledge of the anatomic landmarks in the chest and abdomen can facilitate the routine cardiac screening examination and provide clues to the presence of cardiac abnormality (1, 2). This chapter will focus on the fetal situs, including the anatomic orientation of the organs in the chest and upper abdomen.
● SEQUENTIAL SEGMENTAL ANALYSIS
In evaluating fetal cardiac anatomy, a sequential segmental approach helps in the description of cardiac abnormalities in a clear and simple approach. For many years, pathologists and pediatric cardiologists have been using this approach to describe normal and abnormal hearts (1, 3, 4). In the sequential segmental approach, the cardiovascular system is divided into segments, and for each segment, the anatomy, the position, and the connection with the next segment are described. This sequential segmental analysis involves three anatomic regions: the atria, the ventricles, and the arterial trunks. Each anatomic region is also partitioned into a right- and left-sided component. Atrioventricular valves separate the atria from the ventricles, and the semilunar valves separate the ventricles from the arterial trunks. A fourth anatomic segment, systemic and pulmonary venous connections, should also be evaluated. The cardiac chambers are therefore recognized by their morphologic structures rather than their anatomic locations. The direction of blood flow also helps assess the atrioventricular and ventriculoarterial connections. Assessment of visceral situs and cardiac position, which is described in detail in this chapter, should be part of this sequential segmental approach (1, 3, 4). Table 6.1 presents the steps for the sequential segmental analysis in fetal cardiac evaluation. Detailed anatomic evaluation of cardiac chambers, valvular structures, arterial trunks, and venous systems will be presented in the following chapters.
1. Identify visceral situs 2. Identify atrial arrangement (morphologic right and left atrium) 3. Identify atrioventricular (AV) connections (AV valves) 4. Identify ventricular arrangement (morphologic right and left ventricle) | 5. Identify ventriculoarterial connections (semilunar valves) 6. Identify arterial trunk arrangement (aorta and pulmonary artery) 7. Identify systemic and pulmonary venous connections |
● FETAL VISCERAL SITUS
Assessment of the fetal thoracic and visceral situs is the initial approach to the sequential segmental analysis of the fetal heart by ultrasound (5). Heterotaxy syndrome commonly involves cardiac and abdominal anomalies, and thus focusing on the fetal heart without an evaluation of the upper abdomen often results in an incomplete diagnosis. Although the current method for the determination of fetal situs relies on the position of the stomach and heart in the abdomen and chest, respectively, careful attention should also be paid to the position of the aorta and inferior vena cava below the diaphragm (4, 5) (Fig. 6.1), the orientation of the umbilical vein with the portal sinus, the presence and position of the gallbladder, and when feasible the presence and location of the spleen. It is generally agreed that the positions of the aorta and inferior vena cava below the diaphragm are more reliable criteria for the determination of right or left isomerism than the location of the stomach in the abdomen.
Technique
1. Locate the fetal head within the uterus and determine the presenting part (e.g., cephalic, breech) (Fig. 6.2).
2. Determine the fetal lie within the uterus by obtaining a sagittal view of the fetal spine. (Longitudinal lie: when the fetal spine is parallel to the maternal spine; transverse lie: when the fetal spine is perpendicular to the maternal spine; oblique lie: when the fetal spine is oblique to the maternal spine.)
3. After establishing the exact position of the fetus with steps 1 and 2, determine the location of the fetal left side with regard to the maternal abdomen (fetal left side is anterior [closer to the transducer], posterior [closer to the posterior uterine wall], right lateral [closer to the maternal right uterine wall], left lateral [closer to the maternal left uterine wall]) (Fig. 6.2).
4. Obtain a transverse view of the fetal abdomen by rotating the transducer 90 degrees from the sagittal view of the lower thoracic spine. The fetal stomach is imaged in the left side of the abdomen, the descending aorta is posterior to the left, and the inferior vena cava is anterior to the right (Figs. 6.1 and 6.3). In addition, the intrahepatic part of the umbilical vein is seen connecting with the left portal vein and portal sinus with an L-shape to the right (Figs. 6.1 and 6.3). By sliding the transducer toward the fetal chest, a four-chamber view of the heart is imaged. Note that the apex of the heart is pointing toward the left side of the fetal chest (Figs. 6.2 and 6.4). Determining that the stomach, descending aorta, and cardiac apex are located on the fetal left side and the inferior vena cava is located on the right side establishes normal visceral situs (Figs. 6.1 and 6.3).
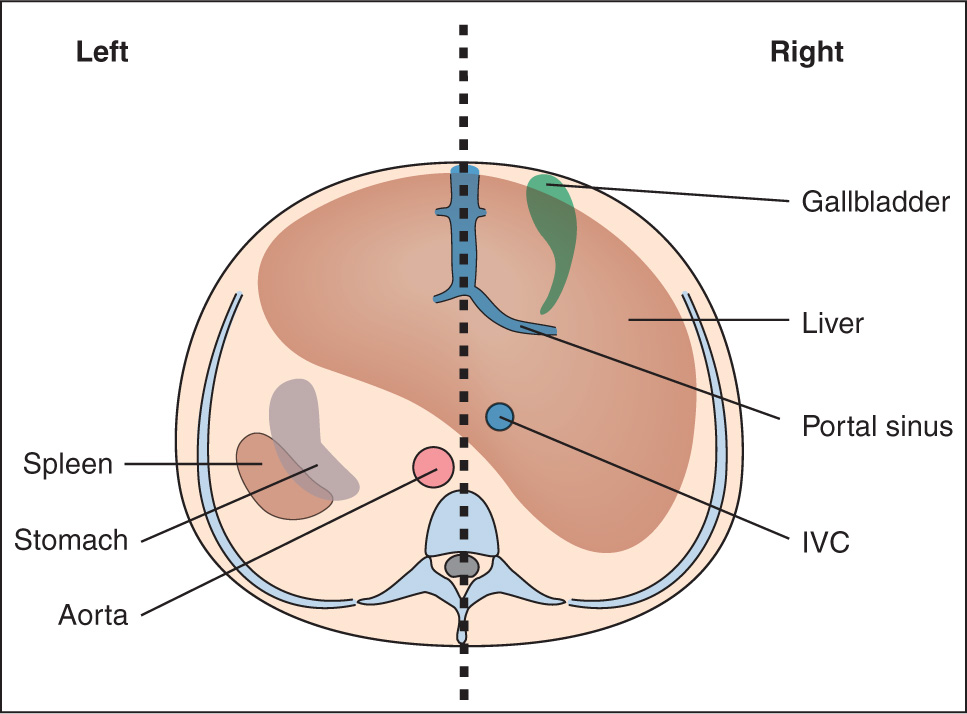
Figure 6.1: Schematic drawing of a cross section of the upper abdomen for the assessment of the abdominal situs. The vertical line divides this plane into right and left. The right-sided structures include the gallbladder, the portal sinus, a large part of the liver, and inferior vena cava (IVC). The left-sided structures include the descending aorta, the stomach, and the spleen. Figure 6.3 is the corresponding ultrasound plane.
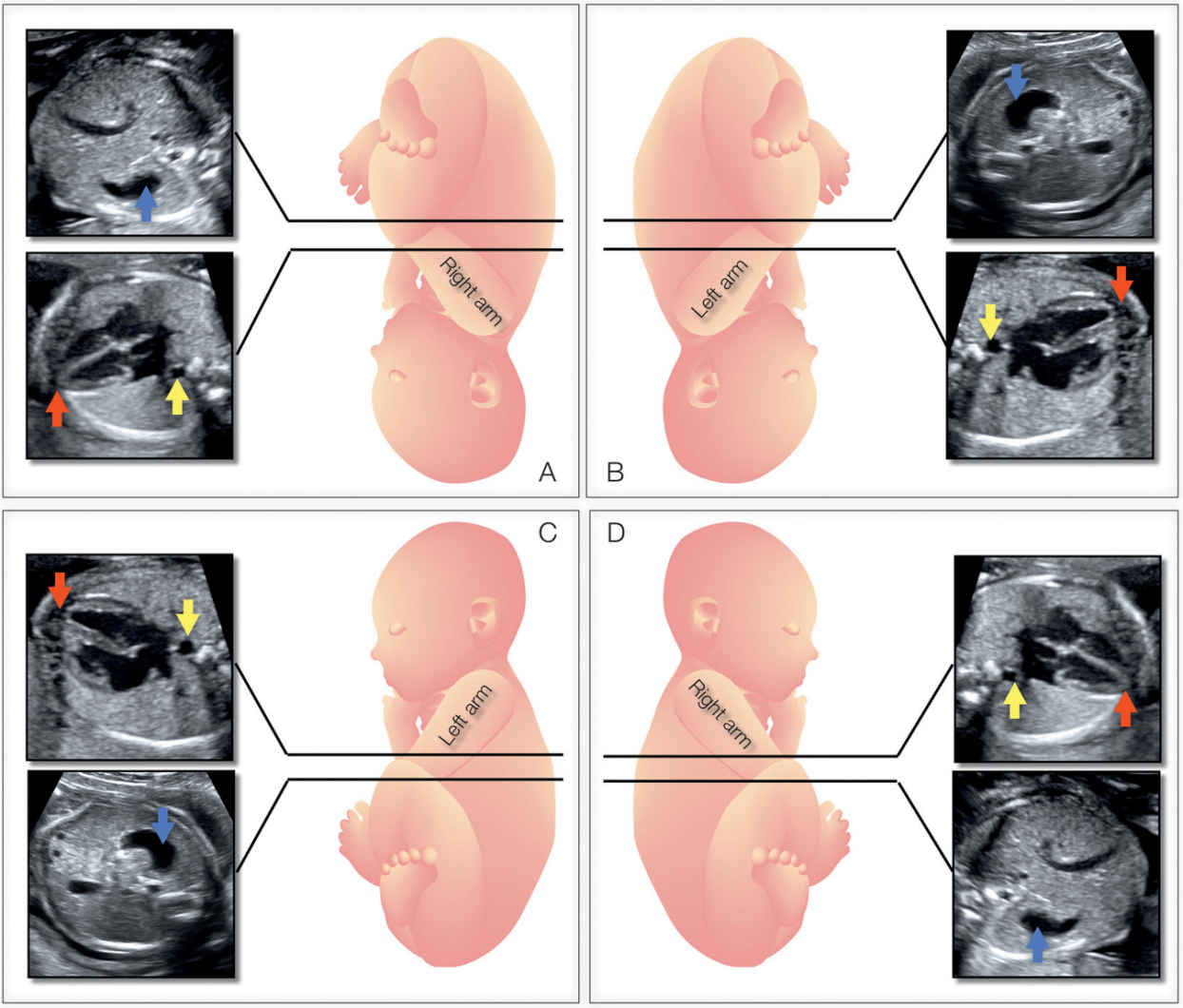
Figure 6.2: Determining fetal situs in longitudinal lie: In A, the fetus is in a cephalic presentation with the fetal spine close to the left uterine wall, resulting in the right side being anterior and left side posterior. In B, the fetus is in a cephalic presentation with the fetal spine close to the right uterine wall, resulting in the left side being anterior and right side posterior. In C, the fetus is in a breech presentation with the fetal spine close to the left uterine wall, resulting in the left side being anterior and right side posterior. In D, the fetus is in a breech presentation with the fetal spine close to the right uterine wall, resulting in the right side being anterior and left side posterior. Note the corresponding transverse ultrasound planes of the chest and abdomen. Blue arrows point to fetal stomach, red arrows to the apex of the heart, and yellow arrows to the descending aorta. See text for details.
Several methods for determining fetal situs during the ultrasound examination have been described. Cordes et al. (6) described a technique that involves orienting the transducer in a standardized way so that the fetal head is on the right side of the screen in a fetal sagittal plane as a starting point and then rotating the transducer 90 degrees in clockwise to obtain the caudocranial transverse views. Another method reported by Bronshtein et al. (7) is referred to as the right-hand rule for abdominal scanning and the left-hand rule for transvaginal scanning (Fig. 6.5). The palm of the hand corresponds to the face of the fetus, and the examiner holds the hand according to the side of the fetal face; the fetal heart and stomach are shown by the examiner’s thumb.
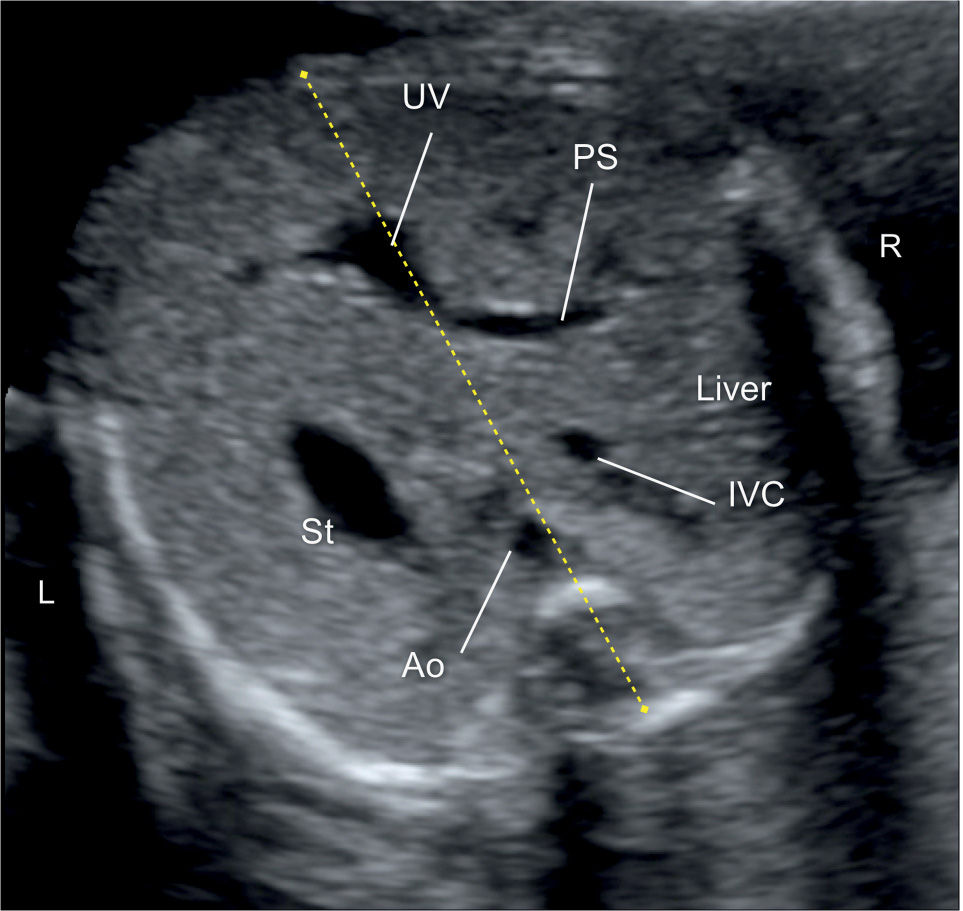
Figure 6.3: Axial view of the fetal abdomen in a fetus with situs solitus. Note the location of the liver, portal sinus (PS), and inferior vena cava (IVC) in right side (R); and the stomach (St) and descending aorta (Ao) in left side (L). The umbilical vein (UV) is located in the midline. Compare with Figure 6.1.
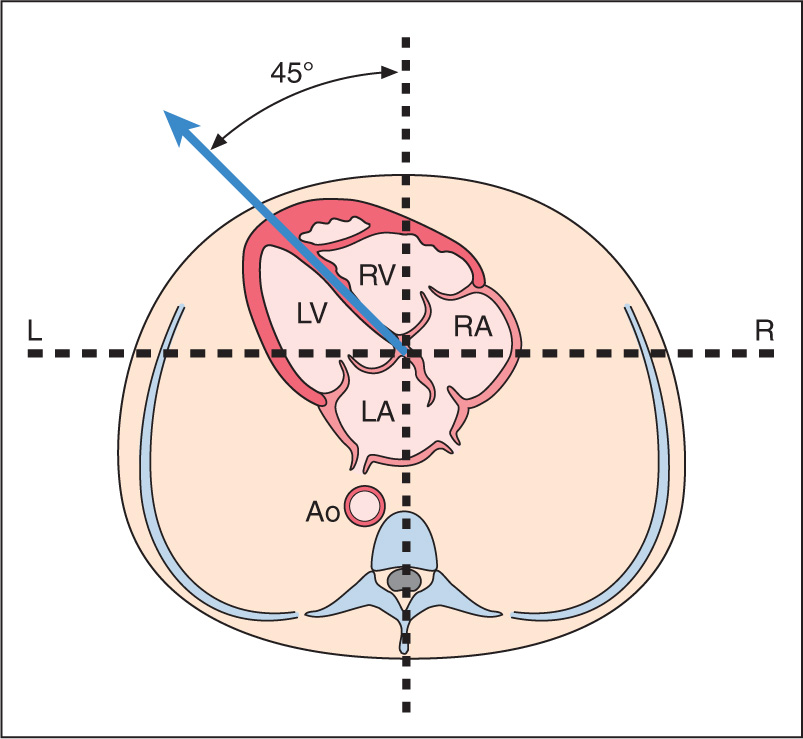
Figure 6.4: Schematic drawing of a cross section of the thorax at the level of the four-chamber view in a fetus with situs solitus. Note the position of the heart in the left chest with a normal cardiac axis of 45 degrees. See text for details. LA, left atrium; RA, right atrium; LV, left ventricle; RV, right ventricle; Ao, Aorta; L, left; R, right.
Situs Solitus, Situs Inversus, and Situs Ambiguous
Three types of visceral situs exist: situs solitus, situs inversus, and situs ambiguous (Table 6.2).
a.) Situs solitus refers to the normal arrangement of vessels and organs within the body (Fig. 6.1).
b.) Situs inversus, with an incidence of about 0.01% of the population, refers to a mirror-image arrangement of organs and vessels to situs solitus. Situs inversus is associated with a slight increase in the incidence of complex congenital heart disease (CHD), in the order of 0.3% to 5% (8), and with the presence of Kartagener syndrome in about 20% of the cases (9). Kartagener syndrome, with an autosomal recessive transmission, primarily involves ciliary dysfunction with recurrent respiratory infection and reduced fertility.
c.) Situs ambiguous (heterotaxy), which refers to visceral malpositions and malformations different from situs solitus or inversus, is commonly associated with complex CHD, abnormalities in venous drainage, bowel malrotations and obstruction, and splenic, biliary, and bronchial tree abnormalities. The incidence of situs ambiguous has been estimated around 1 per 10,000 infants (10). Two types of heterotaxy exist: right isomerism and left isomerism. In right isomerism, also referred to as asplenia, both sides of the body show the right morphology; in left isomerism, also referred to as polysplenia, both sides of the body show the left morphology. Chapter 30 presents a detailed overview of heterotaxy and isomerism in the fetus.
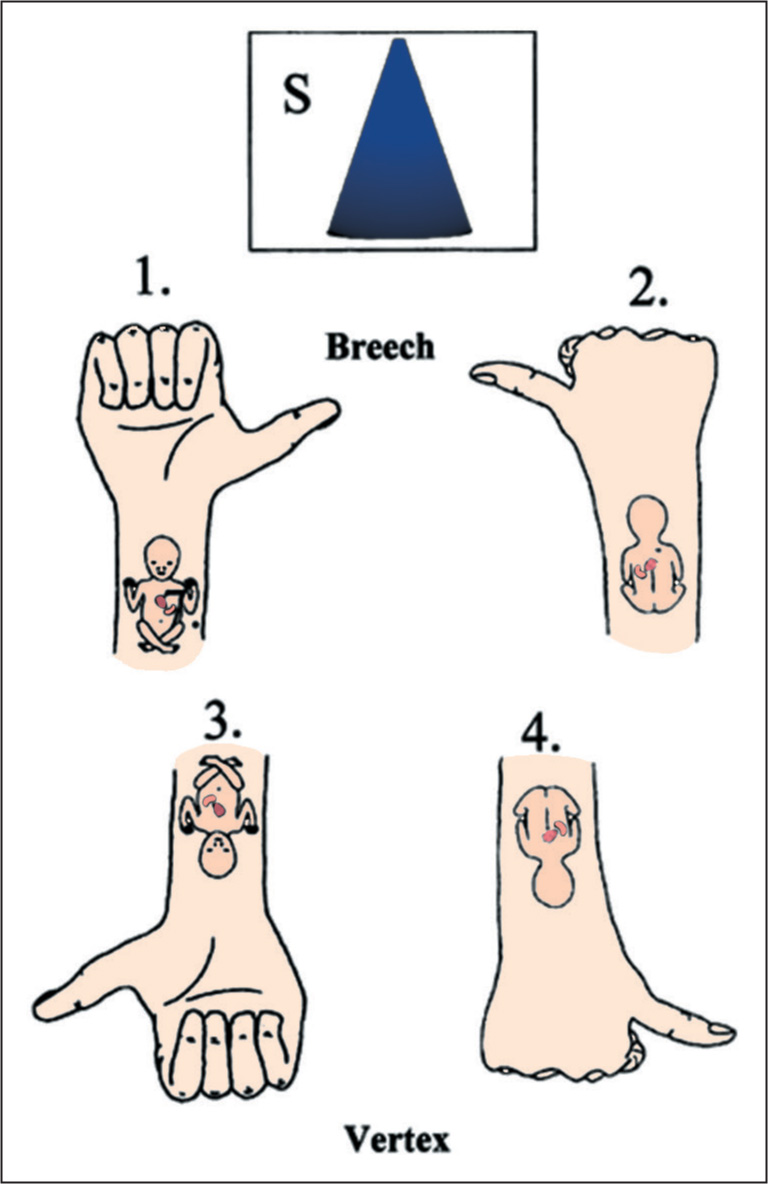
Figure 6.5: Determining fetal situs: A diagram of the fetus is presented in back posterior (1 and 3) and back anterior (2 and 4) positions. In transabdominal scanning, the ultrasound beam (S) is directed from top to bottom. The palm of the right hand represents the face of the fetus, and the fetal heart and stomach are on the same side of the examiner’s thumb. (Modified from Bronshtein M, Gover A, Zimmer EZ. Sonographic definition of the fetal situs. Obstet Gynecol. 2002;99(6):1129–1130, with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


