● INTRODUCTION
In order to be able to accurately interpret fetal cardiac imaging by ultrasound, a full understanding of fetal cardiac anatomy is required (1, 2). The heart is a complex anatomic organ, and when imaged in the fetus, is of such a small size that makes interpretation of normal and abnormal anatomy challenging. Furthermore, the fetal ribs often shadow the fetal heart, especially later in gestation, and optimal imaging of the fetal heart is dependent on the fetal gestational age and the position of the fetus in the uterine cavity. In this chapter, we describe the fetal cardiac anatomy in detail and use anatomic specimen, drawings, and ultrasound images to illustrate various points. We owe a debt of gratitude to Drs. Anna Klassen (Orenburg, Russia) and Cornelia Tennstedt-Schenk (Mühlhausen, Germany), who kindly provided the anatomic specimens shown in this chapter. Figures were digitally altered to highlight various regions of interest.
● THE THORACIC CAVITY
The heart occupies the central portion of the thoracic cavity in the middle mediastinum. It is bordered anteriorly by the lower two-thirds of the sternum and the costal cartilage of the second through the sixth thoracic ribs (1). The heart is bordered by the lungs laterally and posteriorly and by the diaphragm inferiorly (1) (Fig. 5.1). One-third of the heart is located in the right chest and two-thirds in the left chest when the chest is bisected along the midsagittal plane (2).
The sternum binds the thoracic cavity anteriorly, the vertebral column posteriorly, and the ribs laterally (Fig. 5.2). The clavicles, the first ribs, and the body of the first vertebrae border the thoracic cavity superiorly and the diaphragm inferiorly. Although individual ribs incline inferiorly in the adult, in fetal life the ribs assume a more horizontal orientation within the thoracic cavity. In view of this rib orientation in the fetus, transverse views of the abdomen and chest can image large segments of individual ribs (Fig. 5.2).
The heart in the fetus lies horizontally in the thorax, and a four-chamber view plane of the fetal heart is obtained in almost the same plane as a transverse (axial) plane of the chest (Fig. 5.2). With growth, the cardiac apex swings downward and the postnatal heart is positioned more vertically in the thoracic cavity (2). The fetal rib corresponding to the four-chamber view plane of the heart is the fourth thoracic rib (3).
The right and left lungs fill the majority of the thoracic cavity, with the heart occupying the central portion. The right lung is composed of three lobes—superior, middle, and inferior—with a short eparterial main bronchus. The left lung is composed of two lobes—superior and inferior—with a long hyparterial main bronchus. Each lung lobe is further subdivided into lobules and is supplied by a secondary bronchus. Tertiary bronchi supply various segments within each lobe. Individual lung lobes are not seen on ultrasound unless in association with pleural effusion.
The thymus gland is located in the anterior upper mediastinum, bordered by the sternum anteriorly and the great vessels posteriorly (Fig. 5.1).
The posterior mediastinum is an anatomic area in the chest that is located central and posterior to the heart (Fig. 5.2). Structures in the posterior mediastinum include the descending thoracic aorta, the trachea, the main bronchi, the esophagus, the pulmonary veins, and the azygos vein. In the upper posterior mediastinum, the trachea bifurcates, at the level of the division of the main pulmonary artery, into two main bronchi that enter the hilus of each lung, respectively. The esophagus is anterior to the spine and posterior to the trachea in the upper posterior mediastinum. In the midchest region, past the level of the tracheal bifurcation, the esophagus takes a more ventral course to the left of the chest and is located between the thoracic aorta and the left atrium (Fig. 5.2). It then crosses the left diaphragm to connect with the stomach. The azygos vein is a small vessel located posteriorly along the spine slightly to the right side (Fig. 5.2). It forms an arch as it drains into the superior vena cava (SVC) at the level of the bifurcation of the trachea. Four pulmonary veins (two right and two left veins) enter the left atrium posteriorly. The left and right inferior pulmonary veins are seen at the four-chamber view plane (Fig. 5.2) and the left and right superior pulmonary veins are seen at the level of the left ventricular outflow tract plane. The four pulmonary veins anchor the heart to the chest.
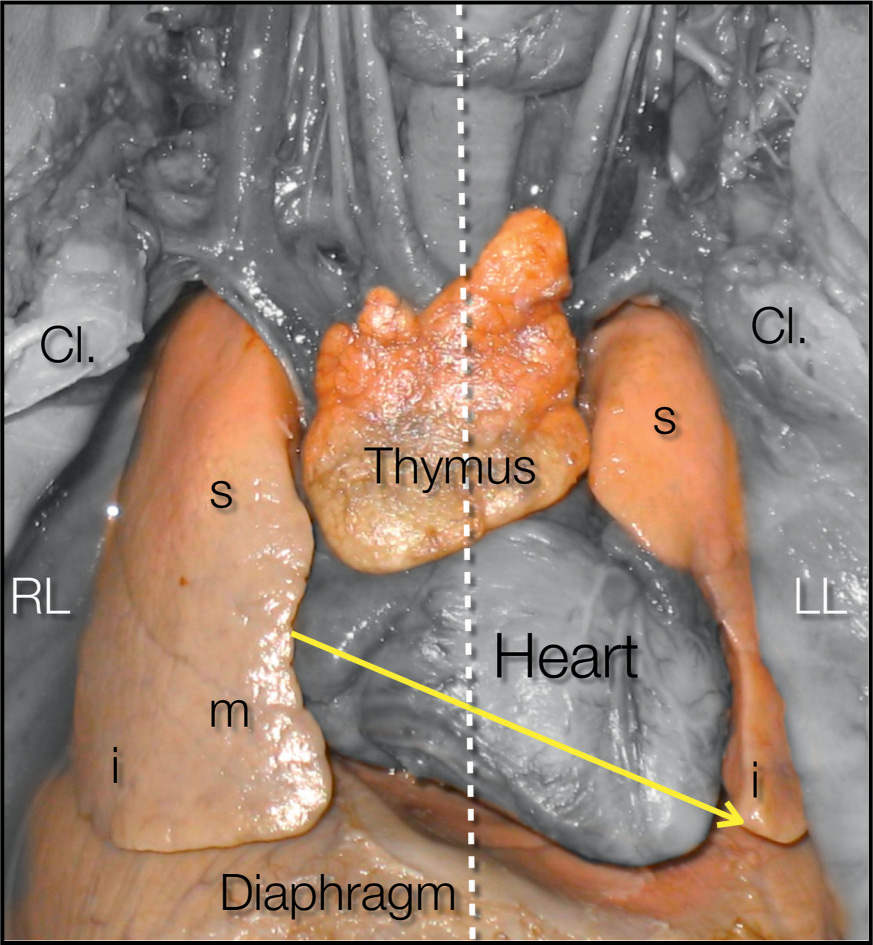
Figure 5.1: Anatomic specimen of the fetal thorax viewed from the front following removal of the sternum and ribs. A vertical line (dashed line) is drawn through the middle of the thorax dividing it into two equal halves. Note the location of the heart in the middle mediastinum with its largest portion located in the left hemithorax. The cardiac axis (yellow arrow) points to the left side. The right lung (RL), left lung (LL), and diaphragm surround the heart. The lung lobes, superior (s), middle (m), and inferior (i) on the right and superior (s) and inferior (i) on the left, are labeled. The thymus gland is seen anterior to the heart. Cl, clavicle.
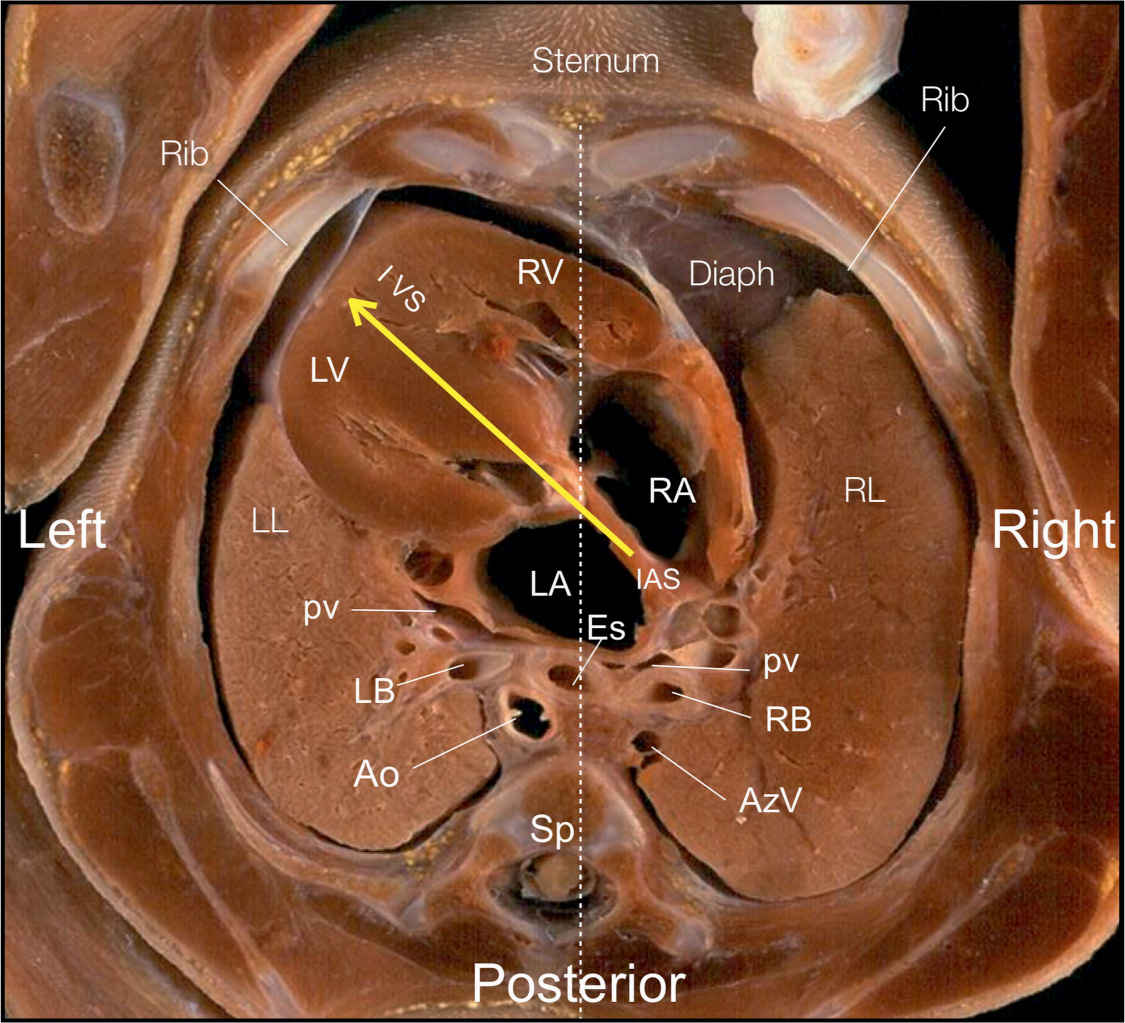
Figure 5.2: Anatomic specimen of a cross section of the fetal thorax at the level of the four-chamber view, showing the right atrium (RA), left atrium (LA), right ventricle (RV), left ventricle (LV), interventricular septum (IVS), and interatrial septum (IAS). A vertical line (dashed line) is drawn through the middle of the thorax dividing it into two equal left and right halves. About two-thirds of the heart is located in the left hemithorax, with the cardiac axis (yellow arrow) pointing to the left (compare with Fig. 5.1). Note in the region posterior to the heart the presence of two pulmonary veins (pv) draining into the left atrium, the thoracic aorta (Ao) left and anterior to the spine (Sp), the esophagus (Es) between the Ao and LA, and the right (RB) and left (LB) bronchi. The azygos vein (AzV) is seen to the right of the spine. RL, right lung; LL, left lung.
● EXTERNAL ASPECT OF THE HEART
The external aspect of the heart is seen from the anterior thorax and shows the cardiac chambers and the great arteries (Figs. 5.1 and 5.3). The external surface of the heart contains several grooves that separate the atria from the ventricles (Fig. 5.3). The atrioventricular (AV) or coronary groove (Fig. 5.3) separates the atria from the ventricles. Within this groove lie the coronary sinus and the main trunk of the coronary arteries. The anterior interventricular groove, which contains the anterior interventricular descending branch of the left coronary artery, separates the right ventricle from left ventricle anteriorly (Fig. 5.3). The posterior interventricular groove contains the posterior descending coronary artery and the middle cardiac vein.
The right atrium occupies a right anterior position within the heart (Fig. 5.3). The right atrial appendage is well recognized as it shows a broad triangular or pyramidal shape (Figs. 5.3 and 5.4).
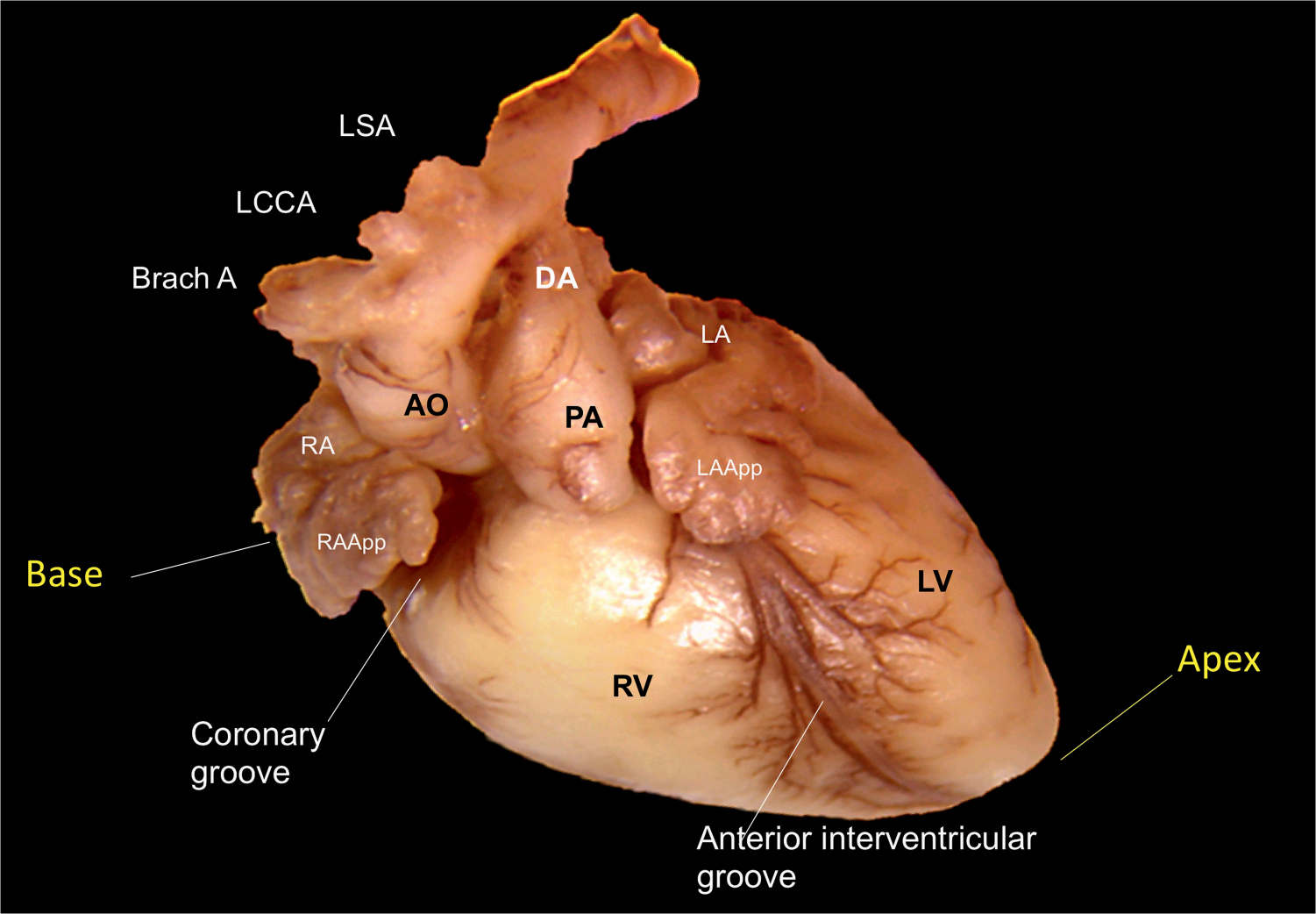
Figure 5.3: Anatomic specimen of the fetal heart shown from an anterior view. The right ventricle (RV) is seen as the most anterior cardiac chamber with the pulmonary artery (PA) arising from it. The anterior interventricular groove separates the RV from the left ventricle (LV). The ductus arteriosus (DA) in the fetus connects the PA with the isthmic region of the aortic arch. The ascending aorta (AO) is seen to the right and posterior to the PA. The three vessels—the brachiocephalic artery (Brach A), the left common carotid artery (LCCA), and the left subclavian artery (LSA)—are seen arising from the transverse aortic arch. Right (RA App) and left (LA App) atrial appendages are also seen. The coronary groove separates the right atrium (RA) from the RV.
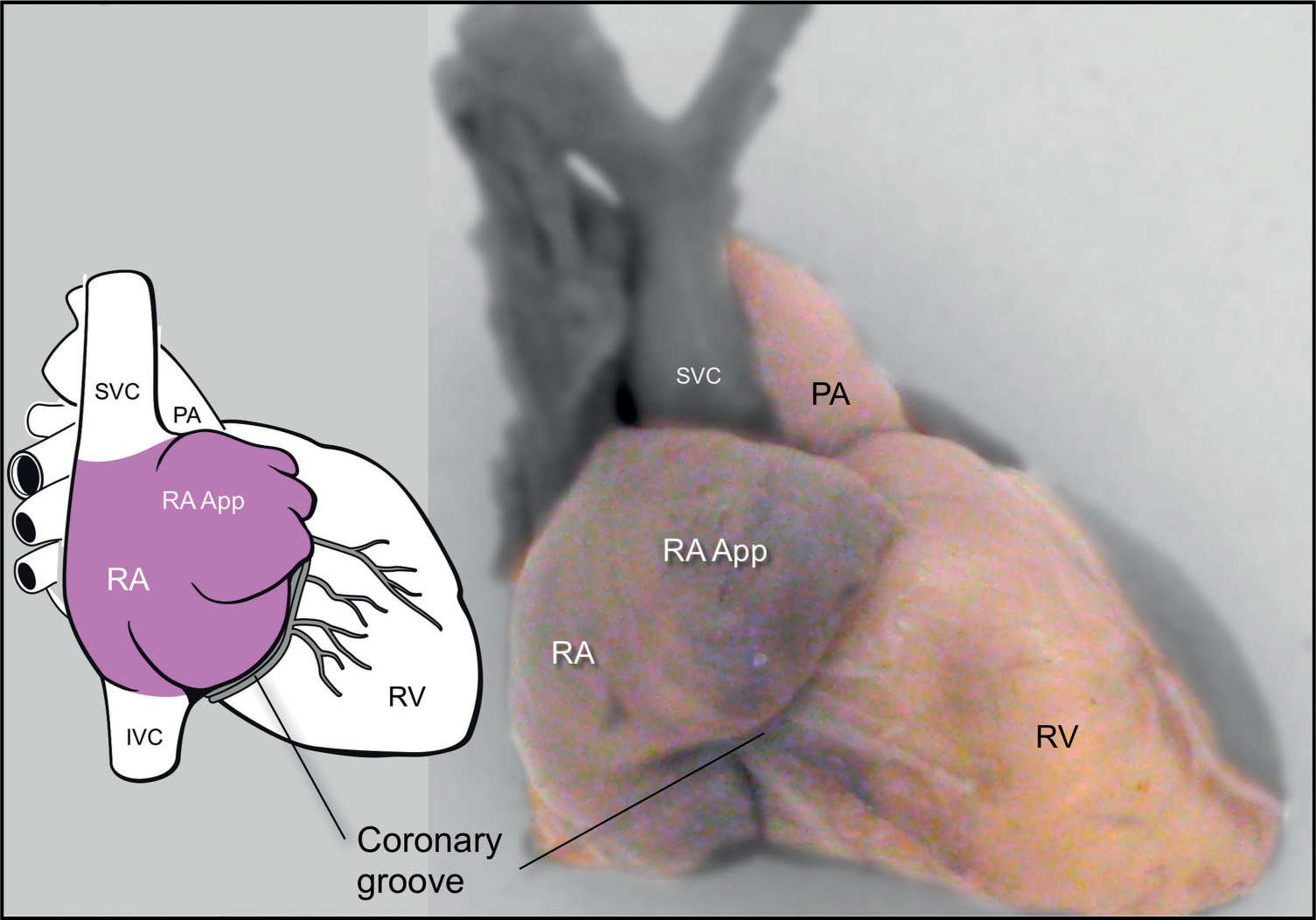
Figure 5.4: Anatomic specimen and a schematic drawing of the anterior right-sided view of the fetal heart. The right atrium (RA), the right atrial appendage (RA App), the right ventricle (RV), and the pulmonary artery (PA) are seen. The superior (SVC) and inferior (IVC) venae cavae enter the RA from its cranial and caudal aspect, respectively.
The right ventricle is positioned anteriorly and occupies the majority of the anterior surface of the heart. The right ventricle, with its anterior outflow tract (pulmonary artery), is the most anterior (ventral) cardiac chamber in proximity to the anterior chest wall (Figs. 5.2 to 5.4).
The left ventricle occupies the left posterior surface of the heart (Fig. 5.3). The left ventricular outflow tract (aorta) occupies the midsection of the heart (Fig. 5.3). The ventricular outflow tracts are well seen in this anterior view of the heart. The origin of the ascending aorta is not seen from the external view of the heart, as it is embedded between the right and left ventricles. The aortic arch, with its course to the right side of the pulmonary artery, is identified in the external view of the heart (Fig. 5.3).
The pulmonary artery emerges from the right ventricle, crosses over the aorta, and dips posteriorly into the chest. It divides into the right and left pulmonary arteries and the ductus arteriosus. The long axes of the two ventricular outflow tracts are perpendicular to each other (Fig. 5.3).
The aorta, with its long axis parallel to the long axis of the left ventricle, angles anteriorly and points toward the fetal right shoulder (Fig. 5.3) as it exits from the left ventricle and before it arches and descends along the left side of the spine. Three arteries originate from the aortic arch: the brachiocephalic (innominate), the left common carotid, and the left subclavian (Fig. 5.3). The pulmonary artery is anterior to the aorta and points toward the fetal left shoulder as it arises from the right ventricle.
The left atrium, which receives blood from the pulmonary veins, is the most posterior cardiac chamber in proximity to the fetal spine (Fig. 5.2). From an anterior view of the heart, the left atrium is not seen (Fig. 5.3). The left atrial appendage, narrow and fingerlike in shape, can be recognized to the left of the main pulmonary artery.
Similar to the adult heart, in the fetal heart, the left ventricle predominantly contributes to the apex of the heart, as it is longer than the right ventricle (Figs. 5.2 to 5.3). The term base of the heart has been used to describe various anatomic landmarks. It is actually the posterior aspect of the atria (Fig. 5.3), but it is often used to describe the base of the ventricular mass (2). A schematic drawing of the base of the heart (Fig. 5.5) describes the surgical view with both atrioventricular valves and the origin of the great vessels. A comparative image on three-dimensional (3D) ultrasound is shown in Figure 15.16.
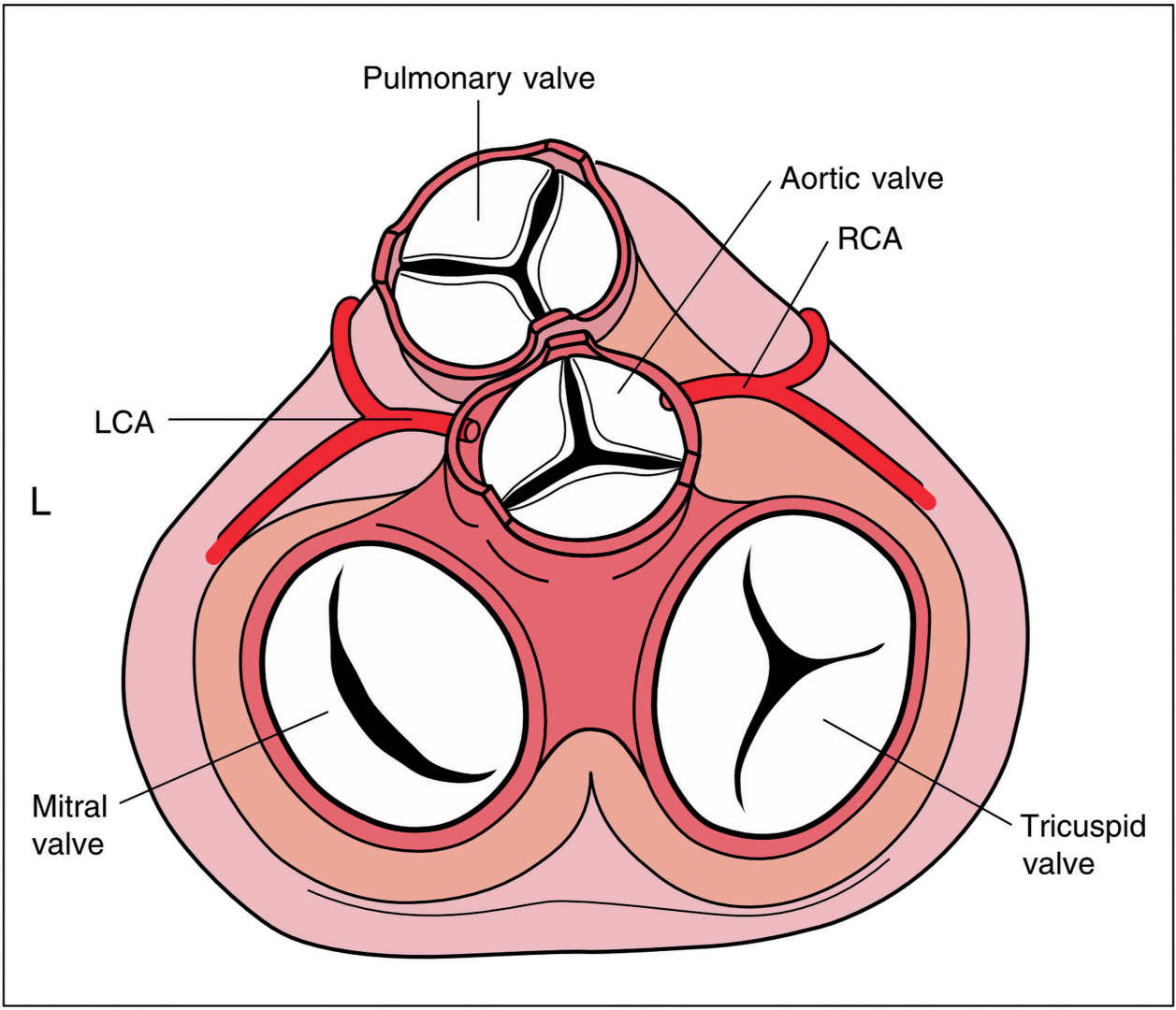
Figure 5.5: Schematic drawing showing the relationship of the semilunar valves to the atrioventricular valves. Note the location of the pulmonary valve, anterior and slightly to the left of the aortic valve. The aortic valve is located in the central portion of the heart, between the tricuspid and mitral valves and posterior to the pulmonary valve. Right (RCA) and left (LCA) coronary arteries are seen to arise from the ascending aorta behind the right and left coronary cusps, respectively. L, left.
● THE CARDIAC CHAMBERS
The Right Atrium
The right atrium is located anteriorly and to the right of the left atrium (Figs. 5.4). The posterior portion of the right atrium (sinus venarum) has a smooth wall and receives the SVC and inferior vena cava (IVC) and the coronary sinus. The anterior portion of the right atrium is lined with coarse muscle bundles, named pectinate muscle (Fig. 5.6). The crista terminalis is a ridge that separates the smooth and coarse regions of the right atrium (Fig. 5.6). This crista runs inferiorly and parallel to the openings of the IVC and SVC. The IVC enters the right atrium at its lowest part, near the interatrial septum (Fig. 5.6). The Eustachian valve, which represents a flap of endocardium, is located at the opening of the IVC (Fig. 5.6). This valve serves a critical function in the fetus as it directs highly oxygenated blood originating from the ductus venosus to the foramen ovale in a caudal-to-cranial flow pattern. On occasions, the Eustachian valve can be imaged on fetal echocardiography in a four-chamber view plane that is posterior to the optimal plane, where it can be mistaken for the flap of the foramen ovale. The opening of the coronary sinus is guarded by the Thebesian valve (Fig. 5.6). The SVC enters the right atrium anteriorly and has no flap at its opening. The sinoatrial (SA) node is located on the epicardium of the right atrial wall superiorly, just below the SVC (Fig. 5.6). The atrioventricular node is located on the floor of the right atrium in proximity to the opening of the coronary sinus.
The right atrial appendage is somewhat pyramidal in shape and has a broad base (Figs. 5.4 and 5.6). The Chiari network, another embryologic remnant, is composed of lacelike strands and is occasionally seen at the level of the tricuspid valve annulus within the right atrium. Table 5.1 lists the anatomic characteristics of the right atrium.
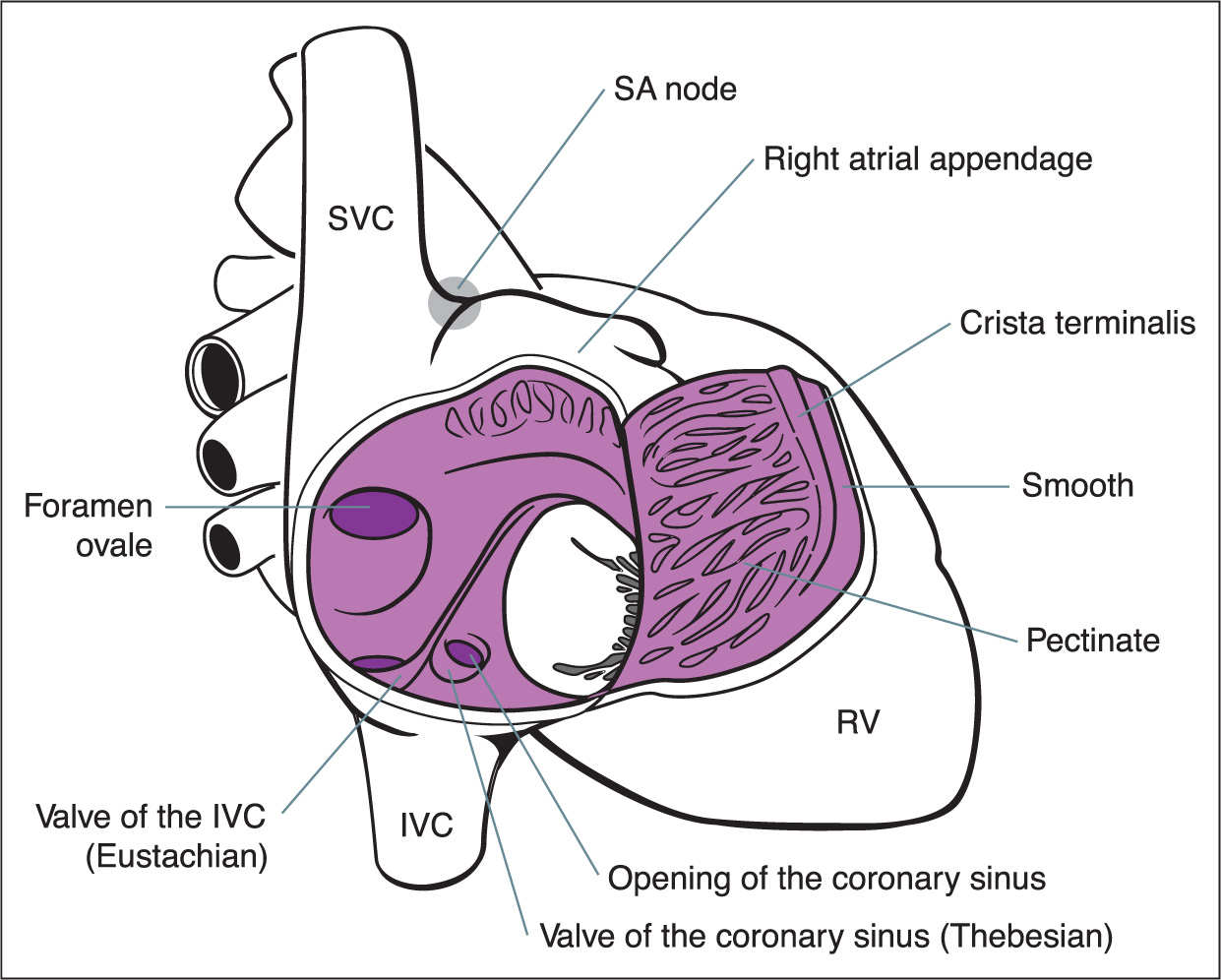
Figure 5.6: Schematic drawing of the internal anatomy of the right atrium (RA). The posterior wall is smooth; the anterior wall is coarse. Note the openings of the inferior vena cava (IVC), superior vena cava (SVC), and coronary sinus. See text for details. RV, right ventricle; SA, sinoatrial.
The Tricuspid Valve
The tricuspid valve prevents the blood from flowing back into the right atrium from the right ventricle during ventricular systole. This valve has three leaflets—anterior, septal, and posterior—named based on their anatomic orientation in the right ventricle (Fig. 5.7). The valves are anchored by chordae tendineae, which prevents the leaflets from prolapsing into the right atrium during systole. Chordae tendineae insert into three papillary muscles (Figs. 5.7 and 5.8). The anterior papillary muscle, the largest of the three and commonly seen on ultrasound, is located at the apex of the right ventricle and receives chordae tendineae insertions from the anterior and posterior leaflets (Fig. 5.7). The posterior papillary muscle is located in the posterior lateral wall and receives chordae tendineae insertions from the posterior and septal leaflets (Fig. 5.7). The septal papillary muscle has attachments to the septal and anterior leaflets. Chordae tendineae from the valve leaflets insert directly into the septal wall, a feature found only in the right ventricle (Fig. 5.7). The tricuspid valve inserts more apically than the mitral valve on the interventricular septum (Fig. 5.8). This anatomic finding is extremely useful in determining ventricular situs and in recognizing atrioventricular canal abnormalities. Unlike the left ventricle inflow and outflow, in the right ventricle, a subpulmonic conus separates the tricuspid valve from the pulmonary valve, resulting in no fibrous continuity between the two (Fig. 5.7).
Anteriorly located, to the right of the left atrium Posterior portion is smooth; anterior portion is trabeculated Receives the inferior vena cava, superior vena cava, and coronary sinus Contains the sinoatrial and atrioventricular nodes Right atrial appendage is pyramidal in shape with broad base |
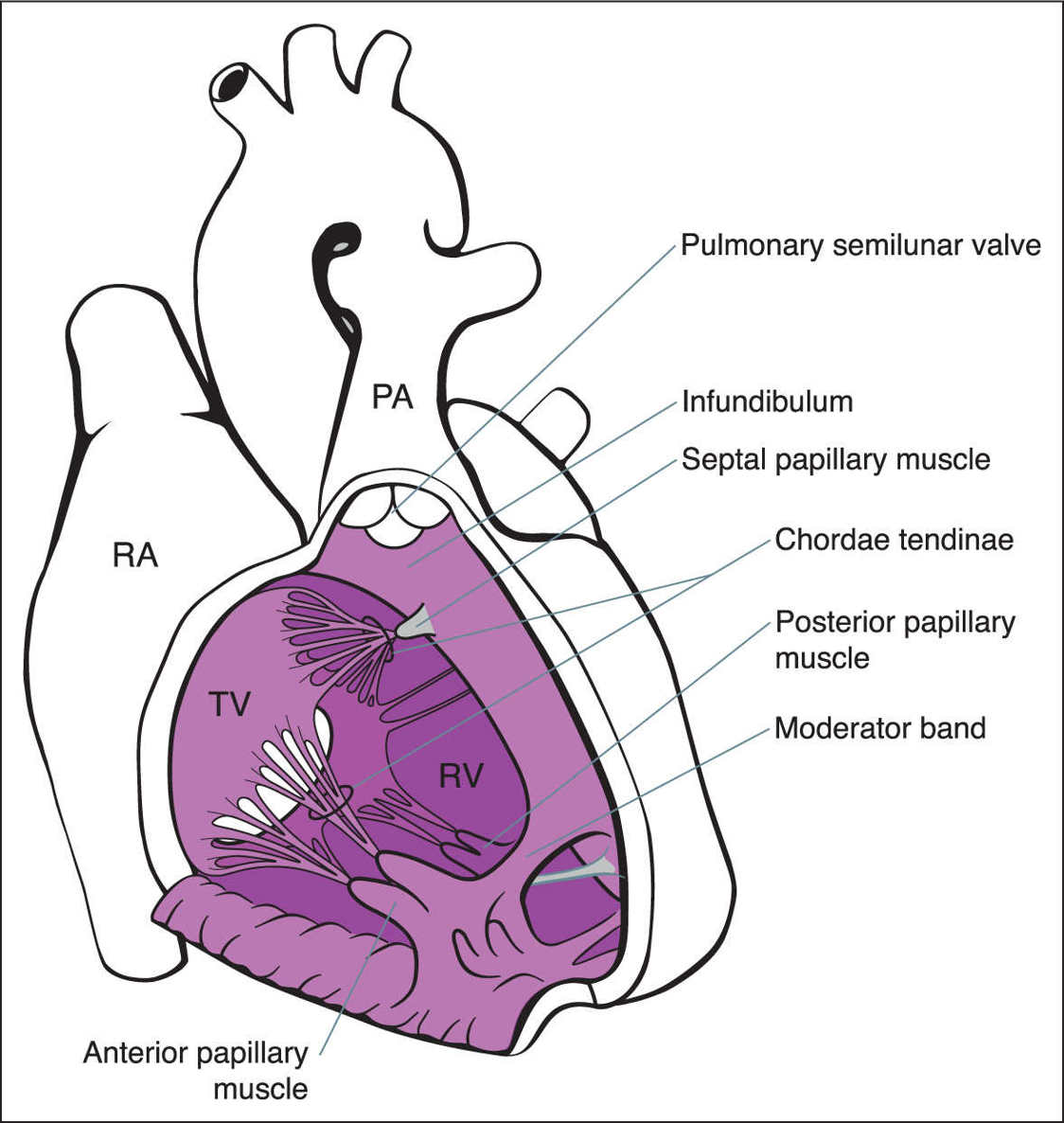
Figure 5.7: Schematic drawing of the internal anatomy of the right ventricle (RV). The RV is made up of an inlet, apical, and outlet portion. The tricuspid valve (TV) is made up of three leaflets and three papillary muscles. The moderator band occupies the apex of the RV. See text for details. RA, right atrium; PA, pulmonary artery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


