Surgical Disorders of the Skin
David Rowe
Arun K. Gosain
Department of Plastic Surgery, Medical College of Wisconsin, Milwaukee, Wisconsin 53226.
Department of Plastic Surgery, Medical College of Wisconsin, Milwaukee, Wisconsin 53226.
ANATOMY
The function of skin was described by Virchow as a covering that conferred protection to the underlying, more complex organs (1). He postulated that skin was a mere passive barrier to the loss of fluid and provided protection against injury. Since the time of Virchow’s observations, we have learned that the skin is, in fact, a highly complex organ characterized by precise interactions of many cellular and molecular processes. In toto, it is the heaviest organ in the body, accounting for up to 16% of total body weight. Skin provides not only a protective barrier against the elements, but also crucial regulatory mechanisms for temperature, sensory input, immunomodulation, and energy.
Skin is composed of many components (Fig. 107-1) and is comprised by the epidermis, arising from an ectodermal epithelial layer, and the dermis, a mesodermally derived connective tissue layer. The epidermis is a layered progression of stratified squamous epithelial cells that ultimately produce keratin and form the stratum corneum, the outermost protective layer of the skin. Interdigitated within the basal layer of the epidermis are melanocytes, which are neural crest-derived cells that provide pigmentation and protection from ultraviolet light. The dermis is the penultimate layer consisting largely of connective tissue. The dermis provides support for the epidermis, effectively attaching the outermost layer to the deeper subcutaneous tissues. Contained in the dermal layer are hair follicles and sebaceous glands, both of which protect the skin surface. The subcutaneous tissue, located under the dermis, consists of loose connective tissue and adipocytes. This layer provides a source of energy storage and provides a flexible and protective structure over deeper organs.
RASHES, PAPULES, AND VESICLES
The etiology of skin eruptions is expansive and not the primary focus of this discussion. Rashes, papules, and vesicles may be diagnosed by an accurate account of character duration, nature of onset, past medical history, family history, and medication use. Table 107-1 describes many common skin disorders, their diagnosis, and treatment modalities (Figs. 107-2 and 107-3).
BENIGN TUMORS
There are a multitude of skin tumors that may be found in children. Although the majority of lumps and bumps are benign, malignant and metastatic lesions may be found in this age group (2) (Table 107-2).
Epithelial Cysts
Epidermoid Cysts
Epidermoid cysts (infundibular cysts) comprise the most common type of surgically excised superficial tumors in children (3). They are lined with squamous epithelium and contain hair, sebaceous material, and keratin. The lesions most commonly occur on the face, neck, or trunk, but may be located in any area. These lesions range in size from 0.2 to 5 cm and enlarge slowly. On examination, they are elevated, tense, smooth intracutaneous or intradermal lesions.
Epidermoid cysts are treated with surgical excision. Complete excision of the cyst is necessary to prevent recurrence because any retained portion of the cyst will likely
cause recurrence. Rupture of the cyst may result in an intense granulomatous reaction. Once this foreign body reaction has occurred, the cyst may become adherent to the surrounding structures, making definitive enucleation problematic. Epidermoid cysts may also become infected. Treatment of infected cysts consists of primary drainage prior to surgical removal. Prior antibiotic treatment of infected or ruptured cysts has not been shown to reduce the bacterial load.
cause recurrence. Rupture of the cyst may result in an intense granulomatous reaction. Once this foreign body reaction has occurred, the cyst may become adherent to the surrounding structures, making definitive enucleation problematic. Epidermoid cysts may also become infected. Treatment of infected cysts consists of primary drainage prior to surgical removal. Prior antibiotic treatment of infected or ruptured cysts has not been shown to reduce the bacterial load.
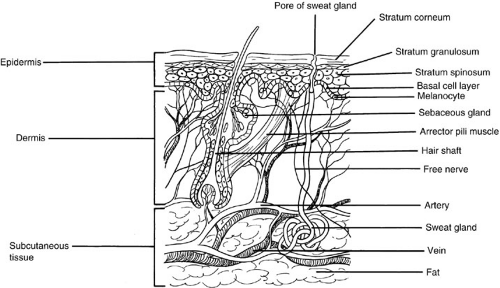 FIGURE 107-1. Schematic representation of the skin. (From Holbrook KA, Sybert V. Structure and biochemical properties of the skin of adults, children, and newborn infants. In: Schachner LA, Hansen RC, eds. Pediatric dermatology. New York: Churchill Livingstone, 1988: 30, with permission.) |
Dermoid Cysts
Dermoid cysts are subcutaneous congenital hamartomas lined by epithelium. These malformations are most commonly found in the lateral ends of the eyebrows and along the lines of cleavage. Size is variable, but may be as large as 10 cm and have similar characteristics as epidermoid cysts. Dermoid cysts have a small but important potential for intracranial extension.
Treatment of dermoid cysts is by surgical excision. Lesions found at the nasofrontal area must be carefully evaluated to rule out intracranial extension of the lesion. Lesions found off midline, such as those at the lateral aspect of the brow, do not routinely require computed tomography (CT) scan for preoperative evaluation (4). CT and magnetic resonance imaging are the two diagnostic modalities used to investigate the penetration of the calvaria for midline lesions.
Milia
Milia are epidermal inclusion cysts that are 1 to 4 mm in diameter. Primary milia are found on the face in as many as 50% of newborns. They are also commonly found in middle-age women, in areas following traumatic injury, and occasionally after prolonged use of nonsteroidal antiinflammatory drugs. Extrusion of cyst contents and abrasive cleaning are the treatment of choice.
VIRAL INFECTIONS
Verrucae (Warts)
Warts are benign tumors caused by the human papilloma virus (HPV). Lesions may be found on the skin or mucus membranes. Although more than 60 variants of HPV have been identified, HPV 2 and 4, the strains associated with verrucae vulgaris, are most common in children. Other lesions such as plantar warts (HPV 1) and condyloma accuminata (primarily HPV 6 and 11) are also found in this age group.
The appearance of condyloma accuminata in the anogenital region may raise suspicion of child abuse and/or early sexual exposure (Fig. 107-4). However, several studies that have investigated the appearance of anogenital warts in children concluded that the majority of these lesions are acquired via nonsexual contact, such as perinatal
contact with the mother or indirect transmission during routine contact situations (bathing, diaper changes) (5,6).
contact with the mother or indirect transmission during routine contact situations (bathing, diaper changes) (5,6).
TABLE 107-1 Rashes, Papules, and Vesicles. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Many methods are available for treatment of verrucae, including chemical and ablative techniques. Surgical excision incurs a high rate of recurrence and thus is usually not indicated. Topical agents such as salicylic acid, trichloroacetic acid, formaldehyde, and glutaraldehyde have been used. Liquid nitrogen is also a popular method of removal. However, this technique does produce pain and blistering. Intralesional bleomycin and topical 5-fluorouracil have also been reported to be effective. Electrodessication may be performed on recalcitrant lesions.
 FIGURE 107-2. Total-body sunburnlike erythema following low-grade fever and upper respiratory symptoms. Epidermal stripping (Nikolsky sign) is indicative of staphylococcal scalded skin syndrome. (From Cohen BA. Skin. In: Oldham KT, Colombani PM, Foglia RP, eds. Surgery of infants and children: scientific principles and practice. Philadelphia: Lippincott-Raven, 1997:1627, with permission.) |
 FIGURE 107-3. Stevens-Johnson syndrome. Severe blistering of skin and mucous membranes, as seen in picture, and widespread rash developed in this 6-year-old girl during a course of trimethoprim-sulfamethoxazole for an ear infection. (From Cohen BA. Skin. In: Oldham KT, Colombani PM, Foglia RP, eds. Surgery of infants and children: scientific principles and practice. Philadelphia: Lippincott-Raven, 1997:1627, with permission.) |
TABLE 107-2 Histologic Diagnosis of 775 Superficial Lumps Excised in Children. | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Molluscum Contagiosum
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


