● INTRODUCTION
It is generally acknowledged that anomalies of aortic arch branching are best understood when basic embryology of the aortic arch is reviewed. The hypothetical double aortic arch theory, suggested by Edwards (1), provides an explanation for various aortic arch abnormalities (2, 3). This theory is based on the presence of double aortic arch in the embryo, where the ascending aorta splits into a right and a left aortic arch, which merge to form the descending aorta, anatomically located in a central position, anterior to the spine (Fig. 29.1). The left and right aortic arches thus form a complete vascular ring, surrounding the trachea and esophagus. The left and right aortic arches give rise to two vessels each: the left and right common carotid and subclavian arteries, respectively (Fig. 29.1). In addition, the left and right pulmonary arteries are connected to the left and right aortic arches, respectively, by a left and right ductus arteriosus in the region of the subclavian arteries (Fig. 29.1). Normal and abnormal development of the aortic arch branching is thus related to which site of the left or right aortic arch regresses or persists during embryonic development (2, 3). Common aortic arch abnormalities encountered on prenatal ultrasound are discussed in this chapter.
● EMBRYOLOGIC FINDINGS
Embryologic events that result in various anatomic orientations of the aortic arch and its branches are hereby presented.
A: Normal (Left-Sided) Aortic Arch
The regression of the right aortic arch segment distal to the origin of the right subclavian artery results in a left aortic arch (normal anatomy) (Fig. 29.1A). The right subclavian and right common carotid arteries merge to form the right brachiocephalic (or innominate) artery. The left ductus arteriosus persists, whereas the right ductus arteriosus regresses.
B: Left-Sided Aortic Arch with Aberrant Right Subclavian Artery
This anomaly results from partial regression of the right aortic arch between the origin of the right common carotid artery and the right subclavian artery (Fig. 29.1B). This leads to the presence of a left-sided aortic arch with the following arising vessels: the right common carotid artery as the first branch, the left common carotid artery as the second branch, the left subclavian artery as the third branch, and an aberrant right subclavian artery (ARSA) as the last branch (Fig. 29.1B). The course of the right subclavian artery is posterior to the esophagus and trachea toward the right arm. The left ductus arteriosus persists, whereas the right ductus arteriosus regresses.
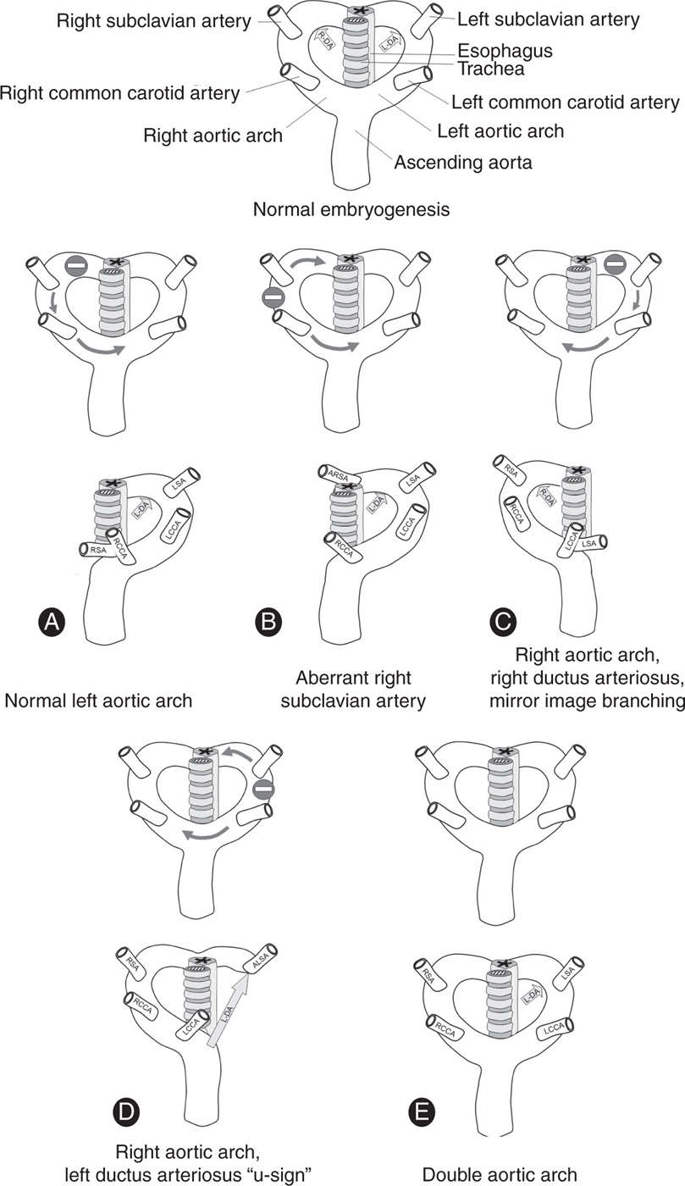
Figure 29.1: Schematic drawings of various forms of aortic arch abnormalities. During embryogenesis (top drawing), a double aortic arch exists, made by the left and right aortic arches, which forms a complete vascular ring surrounding the trachea and esophagus. The left and right aortic arches give rise to two vessels each: the left (LCCA) and right (RCCA) common carotid arteries and left (LSA) and right (RSA) subclavian arteries, respectively. In addition, a left (L-DA) and right (R-DA) ductus arteriosus exist in the region of the subclavian arteries. Normal and abnormal development of the aortic arch branching is thus related to which site of the left or right aortic arch regresses or persists during embryonic development. A: Normal development. B: Left aortic arch with aberrant right subclavian artery. C: Right aortic arch with mirror image branching. D: Right aortic arch with left ductus arteriosus. E: Double aortic arch. See text for details.
C: Right-Sided Aortic Arch with Right Ductus Arteriosus and with Mirror Image Branching of the Brachiocephalic Arteries
This is a mirror image version of the normal left-sided aortic arch. In this anomaly, the left aortic arch distal to the origin of the left subclavian artery regresses, resulting in a right aortic arch (Fig. 29.1C). The left subclavian and the common carotid arteries merge to form the left brachiocephalic (innominate) artery, which arises as the first branch of the right aortic arch followed by the right common carotid artery and the right subclavian artery (Fig. 29.1C). In almost all cases, the right ductus arteriosus persists, whereas the left ductus arteriosus regresses. This condition is often found in association with other congenital heart defects.
D: Right Aortic Arch with Left Ductus Arteriosus
In this anomaly, the left aortic arch regresses between the origin of the left common carotid artery and the left subclavian artery (Fig. 29.1D). The left ductus arteriosus persists in the region of the left subclavian artery, whereas the right ductus arteriosus regresses. This leads to the presence of a right-sided aortic arch and a vascular ring, surrounding the trachea from the left side as well (Fig. 29.1D). The following vessels arise from the aorta: first the left common carotid artery, second the right common carotid artery, third the right subclavian artery, and fourth an aberrant left subclavian artery. On rare occasions, the aberrant left subclavian artery arises directly from the descending aorta through an arterial conduit, called Kommerell diverticulum (4).
E: Double Aortic Arch
This anomaly results from persistence of right and left aortic arches (Fig. 29.1E). The left ductus arteriosus persists, whereas the right ductus arteriosus regresses. Each aortic arch gives rise to a subclavian and a common carotid artery. The double aortic arch forms a tight vascular ring around the trachea and esophagus, which needs surgical intervention postnatally.
● RIGHT AORTIC ARCH AND DOUBLE AORTIC ARCH
Definition, Spectrum of Disease, and Incidence
In normal conditions, the left aortic arch crosses the left bronchus in the upper chest. Right aortic arch is defined by the aortic arch that crosses the right bronchus instead of the left bronchus. In fetal echocardiography, a right aortic arch is diagnosed when the transverse aortic arch is located to the right of the trachea on transverse imaging of the chest (5) (Fig. 29.2B–D). A right aortic arch occurs in about 1 in 1,000 of the general population (5), but the prevalence of right aortic arch is probably higher when cases with other cardiac anomalies are considered. A right aortic arch is associated with three main subgroups of arch abnormalities: right aortic arch with a right ductus (see section C in “Embryologic Findings” [Figs. 29.1C and 29.2B]), right aortic arch with left-sided ductus (see section D in “Embryologic Findings” [Figs. 29.1D and 29.2C]), and double aortic arch (see section E in “Embryologic Findings” [Figs. 29.1E and 29.2D]). Right aortic arch can be part of a complex cardiac malformation, but can often also be an isolated finding (6).
Ultrasound Findings
Gray Scale and Color Doppler
In the four-chamber view, the descending aorta is more centrally located anterior to the spine in right aortic arch (Figs. 29.4A and 29.6A). The detection and classification is achieved in the three-vessel-trachea view, where the aorta has a course to the right side of the trachea (instead to the left) (Figs. 29.2B–D and 29.3 to 29.15). Three subgroups of a right arch can be generally differentiated by fetal echocardiography in combination with color Doppler (6, 7).
1. Right aortic arch with a right ductus arteriosus (right V-sign): In this group, the ductus arteriosus is right sided (see section C in “Embryologic Findings”). Both the aorta and pulmonary arteries merge together in a V-configuration on the right of the trachea with no vascular rings (Figs. 29.3 and 29.4). We refer to this anatomic finding as the right V-sign in contradistinction to the left V-configuration seen in normal anatomy. Because in most cases this condition is associated with a cardiac malformation, mainly a “conotruncal anomaly,” it is often difficult to demonstrate the exact course of the ductus arteriosus (Fig. 29.5). In some of the associated cardiac malformations only a right aortic arch is visualized and the pulmonary artery is, in general, hiding under the aortic arch (Fig. 29.5). The brachiocephalic vessels arise in mirror image branching to the normal left aortic arch. Color Doppler is helpful in the demonstration of the course of the vessels.
2. Right aortic arch with left ductus arteriosus (U-sign): The aortic arch is right sided and the pulmonary trunk and ductus arteriosus are to the left of the trachea (see section D in “Embryologic Findings”). In this condition, the trachea is seen as an echogenic structure between the transverse aortic arch (right) and the ductus arteriosus (left) (Figs. 29.6 to 29.9). These vessels surround the trachea in a U-configuration, called the “U-sign” (5, 8, 9). It is considered a loose “vascular ring” in comparison to the tight vascular ring seen with double aortic arch. This condition is commonly an isolated finding in the majority of cases with rare cardiac or extracardiac associated malformations (6). Associated anomalies include cardiac conotruncal anomalies (Fig. 29.8), chromosomal anomalies such as microdeletion 22q11 (Fig. 29.9), or unspecific extracardiac anomalies. Color Doppler can easily demonstrate the U-sign (Figs. 29.6 and 29.7) (8) and in almost all cases, there is an aberrant course of the left subclavian artery, arising from the region of the junction of the ductus arteriosus with the descending aorta, called Kommerell diverticulum (4).
3. Double aortic arch: The aortic arch has a course to the right side of the trachea but bifurcates directly at the level of the trachea to have one arch to the right and one to the left in the Greek letter “lambda” (λ) configuration (Figs. 29.10 and 29.11) (10). Behind the trachea both arches fuse into the descending aorta, which has a course directly central and anterior to the spine. The esophagus and trachea are entrapped between the right and left aortic arches. Sometimes the left arch is narrower than the right and in some conditions hypoplastic. Generally, the ductus arteriosus has a left-side course and connects with the left arch or descending aorta (Figs. 29.10 to 29.12). Two vessels arise from each aortic arch, a left and a right common carotid and subclavian artery. Color Doppler is helpful in the demonstration of the lambda bifurcation in front of the trachea and the course of the vessels (Figs. 29.10 and 29.11D). Compression of the trachea, at the anatomic level of the double aortic arch, can be demonstrated on a longitudinal view of the neck.
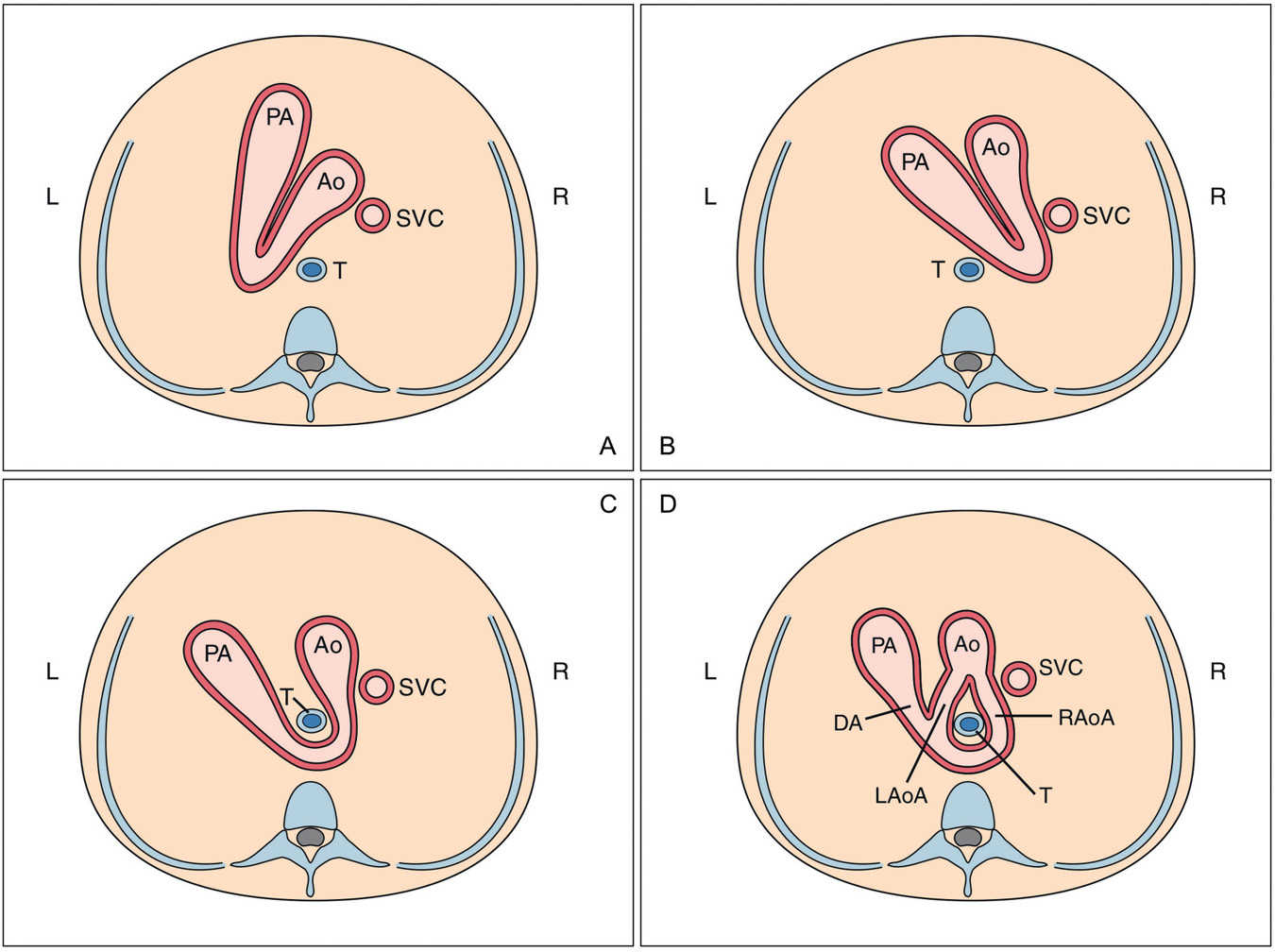
Figure 29.2: Schematic drawings of the three-vessel-trachea view in a normal fetus (A), where the transverse aortic arch (Ao) and isthmus merge with the pulmonary artery (PA) and ductus arteriosus (DA) into the descending aorta in a “V-shape” configuration to the left of the trachea (T). B represents a right-sided aortic arch with a right-sided DA in a “V-shape” configuration to the right side of the trachea. In B, the most common branching of the brachiocephalic vessels is a “mirror branching” to that in A (see text for details). C shows a right aortic arch with the transverse aortic arch to the right side of the trachea; the DA is left sided and the connection of aortic and ductal arches constitutes a vascular ring around the trachea in a “U-shape” configuration. D is a rare subform of right aortic arch with a left DA forming a double aortic arch with the transverse aortic arch bifurcating into a right (RAoA) and a left (LAoA) aortic arch surrounding the trachea and esophagus. L, left; R, right ; SVC, superior vena cava.
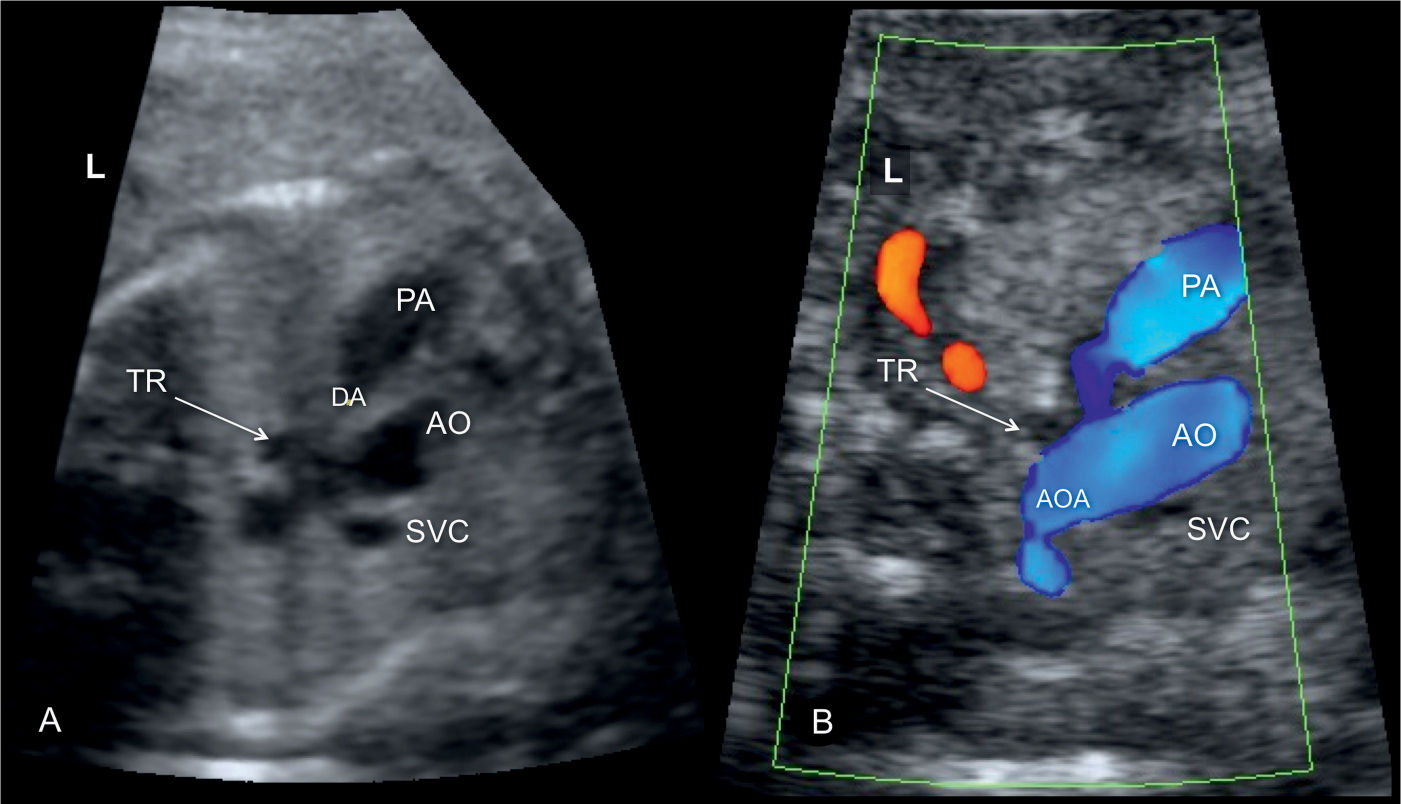
Figure 29.3: Gray scale (A) and color Doppler (B) at the three-vessel-trachea view in a fetus with right aortic arch (AOA) with right ductus arteriosus (DA). Note that both aortic and ductal arches are pointing to the right side of the trachea (TR). 22q11 microdeletion was confirmed postnatally. PA, pulmonary artery; AO, aorta; SVC, superior vena cava; L, left.
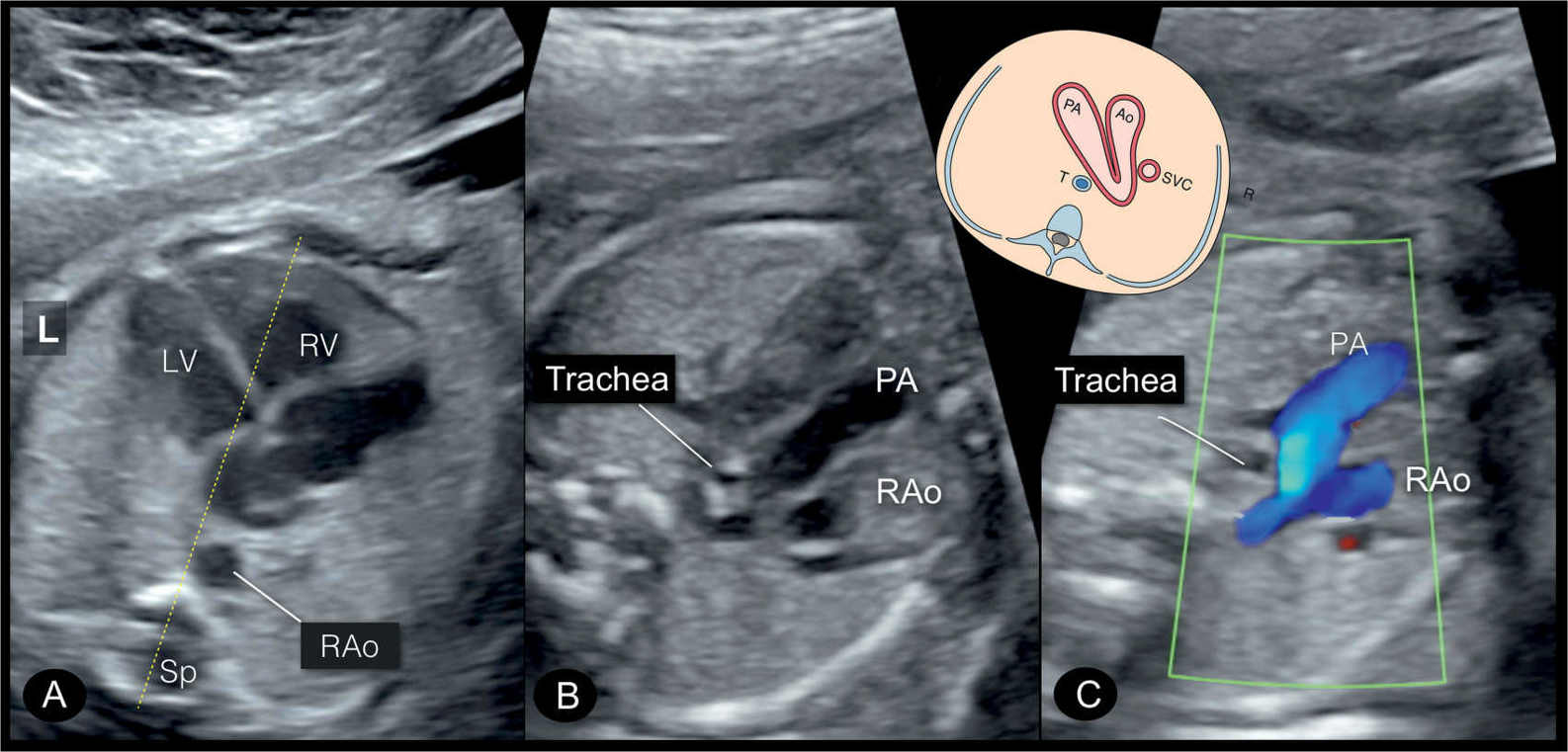
Figure 29.4: Four-chamber view (A) and three-vessel-trachea view in gray scale (B) and in color Doppler (C) of a fetus with right aortic arch (RAo). In this fetus, the ductus arteriosus (DA) is to the right as shown in Figure 29.2B. Note that both aortic and ductal arches are pointing to the right side of the trachea. PA, pulmonary artery; LV, left ventricle; RV, right ventricle; L, left; Sp, spine.
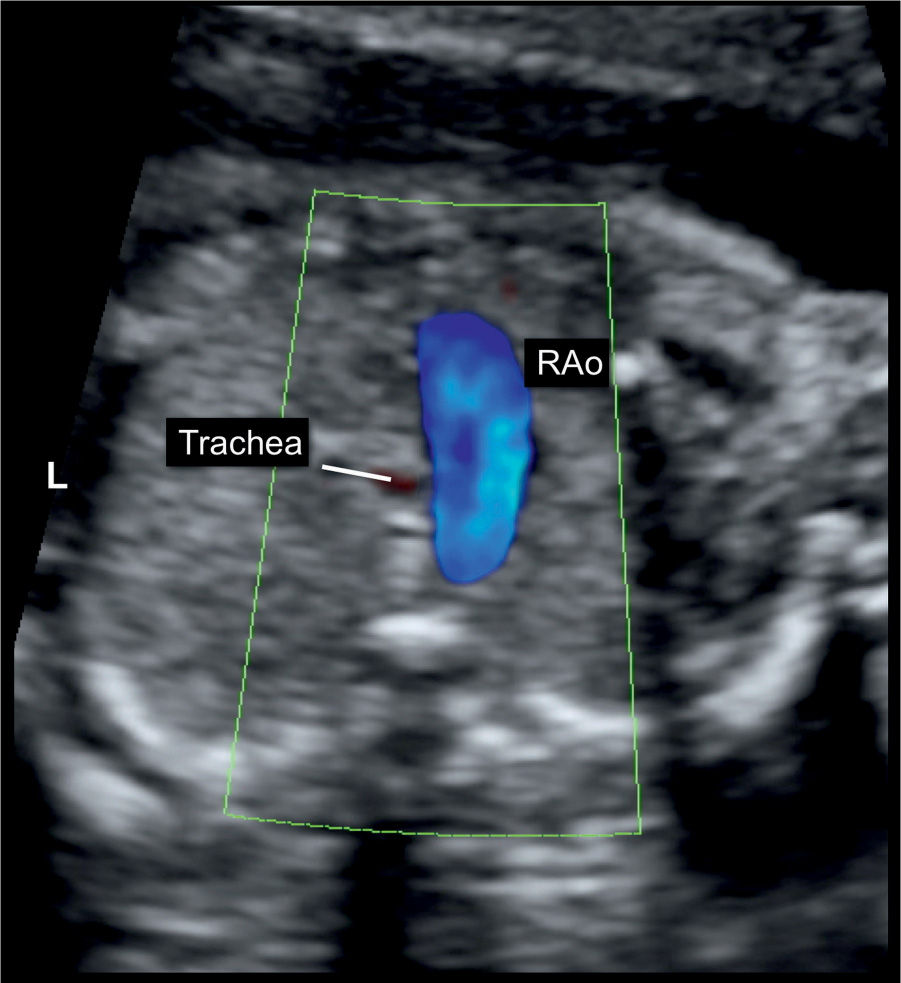
Figure 29.5: Three-vessel-trachea view in color Doppler in a fetus with pulmonary atresia with ventricular septal defect and a right aortic arch (RAo). Note the transverse aortic arch (RAo) is to the right of the trachea. The right ductus arteriosus is not seen, as it is posterior to the RAo. The presence of RAo and right ductus arteriosus is often associated with cardiac anomalies (compare with Fig. 29.8B). L, left.
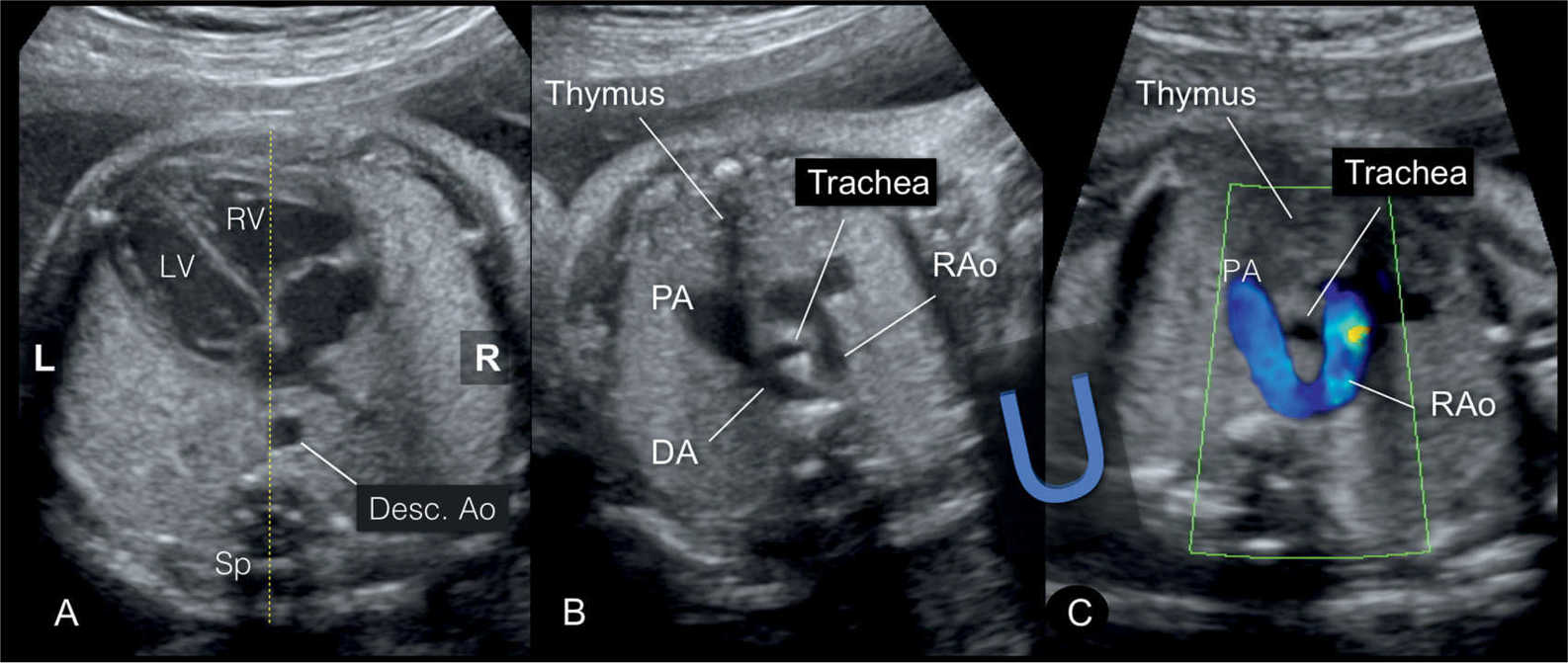
Figure 29.6: Four-chamber view (A) and three-vessel-trachea view in gray scale (B) and in color Doppler (C) of a fetus with a right aortic arch at 30 weeks’ gestation. Note in A the descending aorta (Desc. Ao) located in a central position over the spine. In B and C, the right aortic arch (RAo) has a course to the right side of the trachea, while the pulmonary artery (PA) and ductus arteriosus (DA) are to the left. This forms a “U-shape” configuration, which is more evident in color Doppler (C). Compare with the scheme in Figure 29.2C. This plane raises suspicion of a right aortic arch but does not allow clear differentiation between a right and a double aortic arch (Fig. 29.2C,D). The thymus is identified between the sternum and great vessels (compare with Fig. 29.9B). Sp, spine; RV, right ventricle; LV, left ventricle; L, left; R, right.
Early Gestation
The diagnosis of a right aortic arch is possible in early gestation at 11 to 13 weeks and is enabled by the use of color Doppler at the three-vessel-trachea view (11). It is commonly suspected on transabdominal scanning when the relationship of the transverse aortic and ductal arches is evaluated. Transvaginal scanning can help in confirming the diagnosis. In recent years, we were able to diagnose right-sided aortic arch with its three subgroups in early gestation. Differentiating between the U-sign right aortic arch and the double aortic arch (lambda sign) may be difficult in early gestation. Figures 29.13 to 29.15 show the three aortic arch abnormalities diagnosed in early gestation.
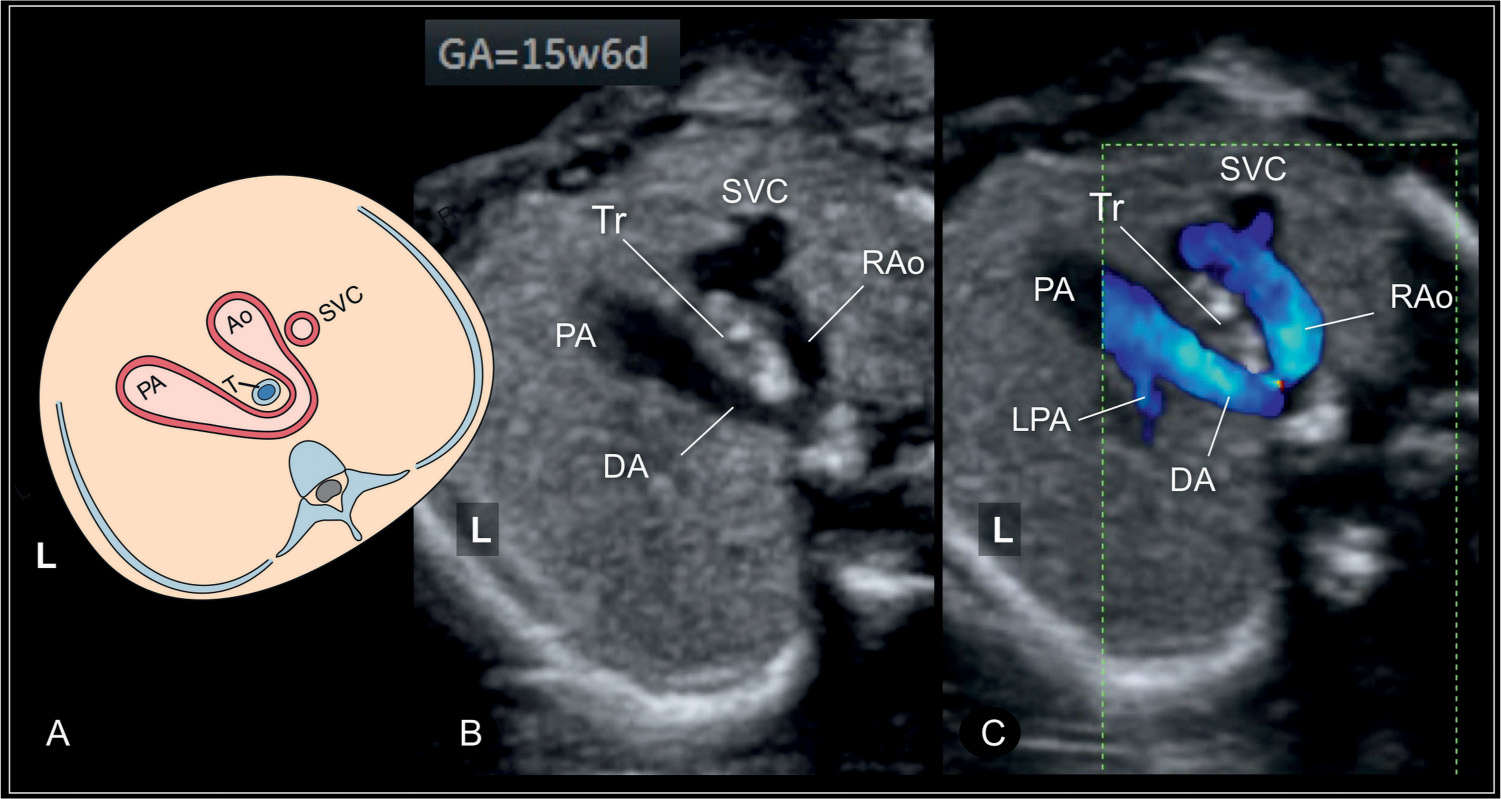
Figure 29.7: Schematic drawing of the three-vessel-trachea view (A) and corresponding ultrasound images in gray scale (B) and color Doppler (C) of a fetus at 15 weeks’ gestation with a right-sided aortic arch (RAo) and a left-sided ductus arteriosus (DA). Note that the RAo and DA form a U-configuration around the trachea (see also Fig. 29.6). The fetus was examined with a high-resolution linear transducer (see Fig. 29.6 for more details). SVC, superior vena cava; PA, pulmonary artery; LPA, left pulmonary artery; Ao, aorta; Tr or T, trachea; L, left.
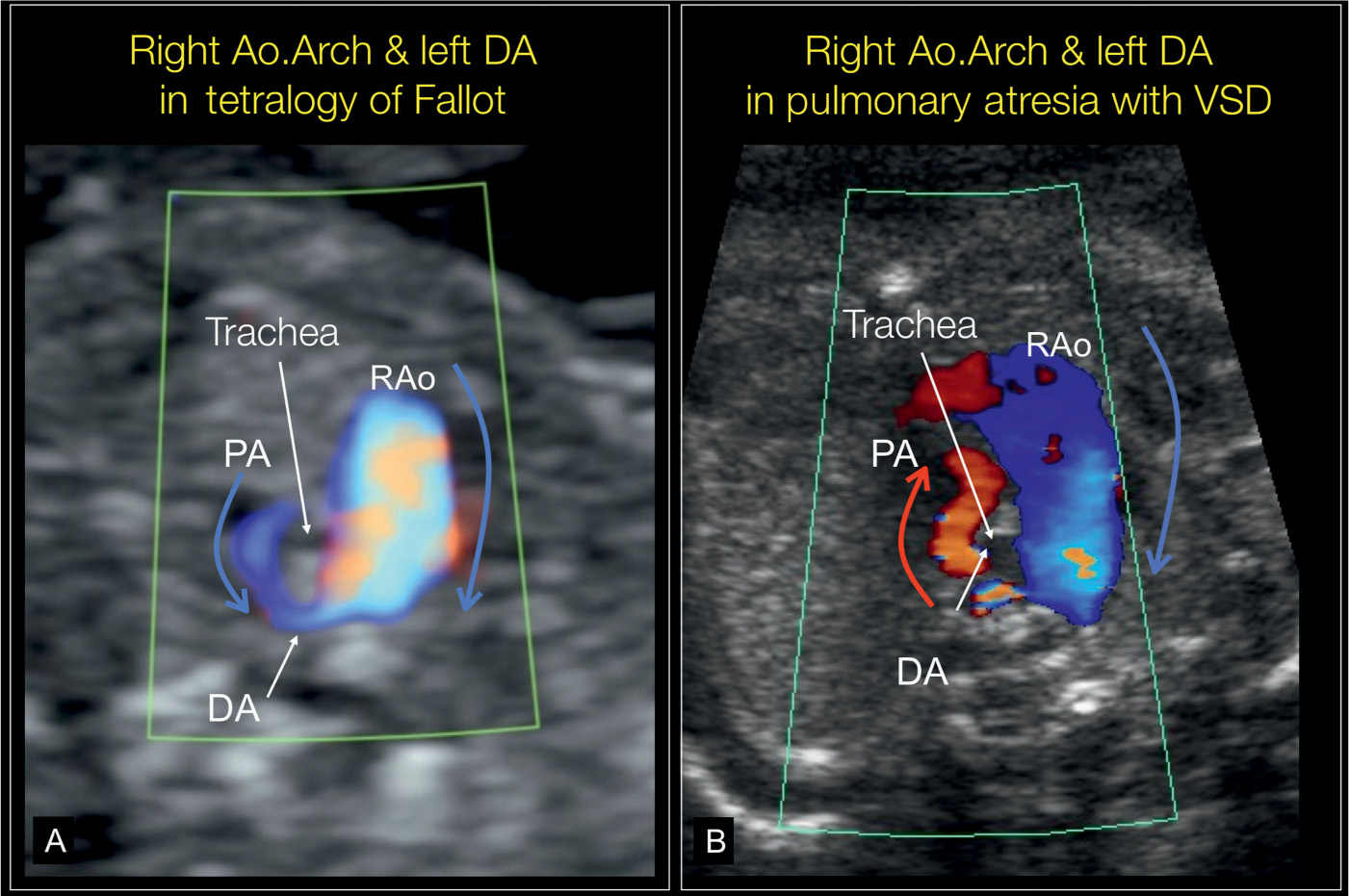
Figure 29.8: Color Doppler of the three-vessel-trachea view in two fetuses with a right aortic arch (RAo) and a left-sided ductus arteriosus (DA). The fetus in A also has a tetralogy of Fallot with antegrade flow in both aorta and in the small stenotic pulmonary artery (PA) (blue arrow). Fetus B also has pulmonary atresia with VSD. Note in B the presence of antegrade flow in the RAo (blue arrow) and retrograde flow in the small PA (red arrow). Compare with Figures 29.6C and 29.7B. VSD, ventricular septal defect.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


