results do not support maintaining oxygen saturation levels in very preterm infants in the first weeks of life between 85% and 89%. This is still a very controversial area. Although lower saturations are not routinely recommended, high saturations may also have increased risks, so limiting high saturation alarm to 95% is a common recommendation for these preterm infants (1). Additional analyses are being conducted that will combine individual patient data from these studies in an effort to arrive at a more precise and timely recommendation for specific groups of patients based on gestational age, postnatal age, and perhaps other confounding factors.
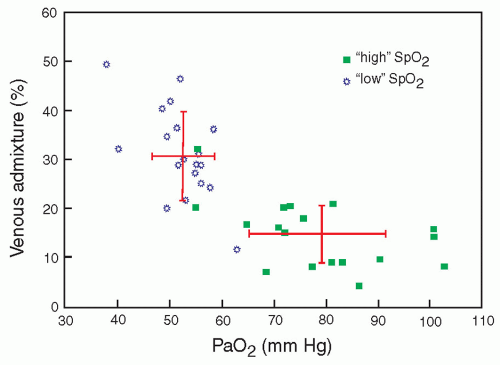 FIGURE 28.1 Relationship between venous admixture and PaO2. From Schulze A, Whyte RK, Way RC, et al. Effect of the arterial oxygenation level on cardiac output, oxygen extraction, and oxygen consumption in low birth weight infants receiving mechanical ventilation. J Pediatr 1995;126(5):777, with permission. |
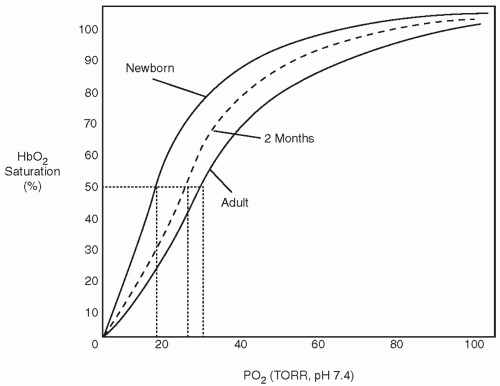 FIGURE 28.2 Oxygen equilibrium curves of hemoglobin at birth, 2 months of age, and adulthood. Note the increase in P50 with age. |
able to increase the work of breathing to accomplish adequate gas exchange without treatment, including oxygen administration. The extremely premature infant will have a much weaker respiratory drive and inadequate muscular development and, thus, is less able to compensate for lung abnormalities. The classic clinical signs of respiratory distress are helpful in the assessment of the mature newborn infant. Nasal flaring, grunting respirations, and tachypnea are almost always present. With progression of lung disease and decreased lung compliance, chest wall retractions become more marked. With increased work of breathing, retractions progress from sternal to subcostal, to intercostal, and then to a seesaw pattern of chest and abdominal wall movement. The full-term infant may increase respiratory rate above 100 per minute, with shallow respirations. This pattern is the most efficient way to increase gas exchange, with the least costly work of breathing. Expiratory grunting represents an effort to retard expiratory flow to increase end-expiratory pressure and maintain alveolar patency. It is unsafe to rely on color changes as an indication of oxygenation, as abnormalities in peripheral perfusion as a result of poor cardiac output, hypotension, or hypovolemia may be misleading. Similarly, infants with recurrent apnea will have intermittent deficiency in gas exchange. Auscultation assists in determining the quality of air entry in various parts of the lung and the presence of airway secretions or obstructions.
spontaneous breathing or as positive end-expiratory pressure (PEEP) during mechanical ventilation. This usually requires pressures from at least 5 cm H2O to 8 cm H2O if the lung disease is severe.
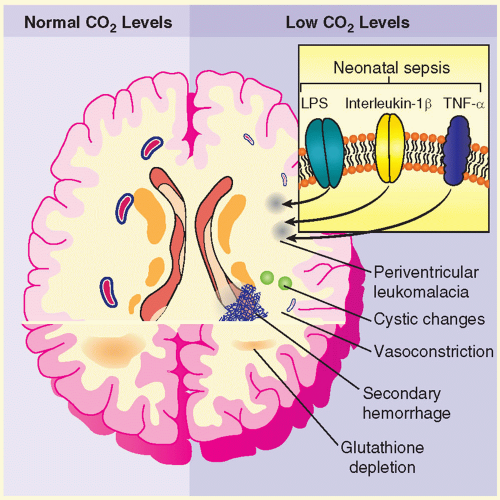 FIGURE 28.3 Effects of hypocapnia on the brain in premature infants. Hypocapnia has been implicated in the pathogenesis of neonatal white matter injuries, including periventricular leukomalacia, resulting in IVH. At normal CO2 levels (left-hand side of figure), cerebral blood flow is determined by local metabolic demand. Prolonged or severe hypocapnia includes severe cerebral vasoconstriction, resulting in brain ischemia, particularly in poorly perfused areas of the brain such as watershed areas (right-hand side of figure). This ischemia may initiate white matter destruction in the brain of premature infants. Additionally, antioxidant depletion (caused by excitatory amino acids), lipopolysaccharide (LPS), and cytokines produced in response to sepsis, such as interleukin-1β and tumor necrosis factor-α (TNF-α), potentiate the process. Finally, restoration of the normal partial pressure of arterial CO2 can result in cerebral vasodilation, which may precipitate or contribute to intraventricular hemorrhage. From Laffey JG, Kavanagh BP. Hypocapnia. N Engl J Med 2002;347(1):43, with permission. |
TABLE 28.1 Risks of Hypocarbia and Hypercarbia | ||||
|---|---|---|---|---|
|
 FIGURE 28.4 Gestational age and rates of respiratory treatments and admission in a neonatal intensive care unit (NICU) in a population of 173,058 live-born infants (Years 2000-2009). CPAP, continuous positive airway pressure. From Guoyon JB, Iacobelli S, Ferdunus C, et al. Neonatal problems of late and moderate preterm infants. Semin Fetal Neonatal Med 2012;17:147, with permission. |
 ) matching may injure epithelial and endothelial tissues. In the incompletely developed lungs, structures are less elastic and more vulnerable to barotrauma and volutrauma. Injury to the mesenchymal and epithelial tissues that later give rise to alveolar septation and vascular formation may be irreversible. Studies in adult animals have demonstrated that otherwise-healthy lungs can suffer injury, which is reflected by increased airway fluid and deterioration of gas exchange, if inappropriate distending lung pressures are applied (33). The particular problems of providing assisted ventilation are illustrated in Figure 28.5 (34). Relative immaturity of distal bronchioles and respiratory ducts, coupled with fluid-filled and collapsed alveoli, create a set of conditions leading to overdistention of some areas and underventilation of other areas, with resultant ineffective gas exchange. This uneven ventilation, coupled with injury produced by ROS, contributes to the common problem of CLD of prematurity. The risk of its development is inversely correlated with birth weight.
) matching may injure epithelial and endothelial tissues. In the incompletely developed lungs, structures are less elastic and more vulnerable to barotrauma and volutrauma. Injury to the mesenchymal and epithelial tissues that later give rise to alveolar septation and vascular formation may be irreversible. Studies in adult animals have demonstrated that otherwise-healthy lungs can suffer injury, which is reflected by increased airway fluid and deterioration of gas exchange, if inappropriate distending lung pressures are applied (33). The particular problems of providing assisted ventilation are illustrated in Figure 28.5 (34). Relative immaturity of distal bronchioles and respiratory ducts, coupled with fluid-filled and collapsed alveoli, create a set of conditions leading to overdistention of some areas and underventilation of other areas, with resultant ineffective gas exchange. This uneven ventilation, coupled with injury produced by ROS, contributes to the common problem of CLD of prematurity. The risk of its development is inversely correlated with birth weight.tract results in a total airway resistance approximately 15 times greater than that of an adult (39). Edema and inflammation can produce extremely high resistance to air flow in these narrow airways. During expiration, the airways become narrower, and resistance increases.
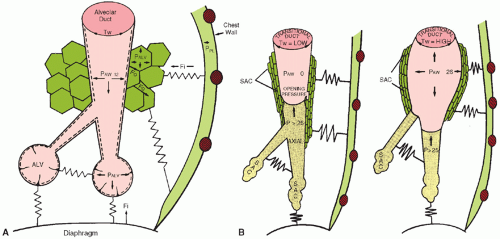 FIGURE 28.5 A: A mature alveolar duct and alveoli. Dotted line, surfactant; PALV, alveolar pressure; PAW, airway pressure; PPL, pleural pressure; Fi, tissue force (stretched springs) acting inward; Fo, tissue force directed outward; Tw, wall tension or recoil pressure. B: The end-expiratory airway pressure (PAW) equals zero in an immature distal airway (left). The saccules (SAC) and airways contain fluid (shaded area). The axial airway is concave at the air-liquid interface as a result of the surface tension forces. The peripheral SACs are collapsed or fluid filled. The lax tissues are represented by relaxed springs. The inspiratory airway pressure (PAW) is equal to 26 cm H2O (right). The distended distal airway has a high wall tension (TW). The liquid front has been pushed peripherally, but the SACs are still not inflated. From Thibeault DW, Lang MJ. Mechanisms and pathobiologic effects of barotrauma. In: Merritt TA, Northway WH Jr, Boynton BR, eds. Bronchopulmonary dysplasia. Contemporary issues in fetal neonatal medicine. Boston, MA: Blackwell Scientific Publishers, 1988:82, with permission. |
 FIGURE 28.6 Laryngoscopy for endotracheal intubation. |
of tube placement are intubation of the esophagus and intubation of the right mainstem bronchus. Auscultation, although helpful, is not reliable because breath sounds are well transmitted in a small chest. A chest radiograph should be obtained to confirm tube placement.
TABLE 28.2 Depth of Insertion of an Orotracheal Tube from the Lips of a Premature Infant | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
 ) matching. Distribution of tidal volume may vary with the associated PIP; low PIP can
) matching. Distribution of tidal volume may vary with the associated PIP; low PIP can result in tidal volume distribution only to already overinflated lung regions, resulting in worsened (
 ) matching, development or exacerbation of high (
) matching, development or exacerbation of high ( ) areas, and worsening of CO2 retention, despite normal or elevated (
) areas, and worsening of CO2 retention, despite normal or elevated ( )
) ) areas (48).
) areas (48).inspiratory effort and provide the mechanical initiation of machineassisted ventilation during the early phase of the infant’s inspiration. Currently used methods to signal the initiation of inspiratory effort are listed in Table 28.4. The current methodology allows transduction to be accomplished in as short a time as 30 to 50 milliseconds, approximately one-tenth the duration of the inspiratory phase of a spontaneous respiratory cycle (Fig. 28.7) (50). The means by which this signal is provided and the addition of other subtle but potentially important changes in the capabilities of particular ventilators differentiate one type of conventional neonatal ventilator from another (51). A list of available modes and their theoretical advantages is found (Table 28.5).
TABLE 28.3 Management Considerations | ||
|---|---|---|
|
TABLE 28.4 Available Mechanisms for Detecting Onset of Respiration | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
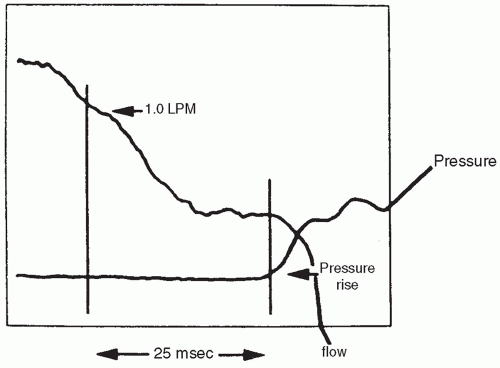 FIGURE 28.7 System response time, also known as trigger delay. The flow change trigger is set at 1.0 LPM. It took 25 milliseconds from the time this threshold was reached (vertical line on the left) until there was a measurable rise in airway pressure (vertical line on the right). From Donn SM, Sinha SK. Controversies in patient-triggered ventilation. Clin Perinatol 1998;25:49, with permission. |
machine-initiated tidal volume and flow patterns. Sensors monitor instantaneous flow rate and volume of gas from ventilator to patient; the applied pressure then changes according to the equation of motion. This system may allow for both greater patient comfort and reduction of peak airway pressure required to sustain ventilation, with less likelihood of overventilation compared to assist/control modes (52).
TABLE 28.5 Modes of Assisted Ventilation Via Endotracheal Tube | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
 FIGURE 28.8 Tidal volume tracings (Inspiration = Upward) demonstrating three patterns of ventilator interaction with spontaneous breathing. In this illustration, tidal volume of spontaneous breaths is less than that of ventilator breaths. A: Asynchronous intermittent mandatory ventilation (IMV) with ventilator breaths delivered during spontaneous expiration. During IMV, ventilator breaths occur at a constant rate, with random timing with respect to spontaneous breaths. B: Synchronous intermittent mandatory ventilation (SIMV) with ventilator breaths delivered early in selected spontaneous inspirations. During SIMV, ventilator breaths occur more irregularly, but the ventilator delivers the set rate synchronously with spontaneous breaths. C: Assist/control mode, with ventilatory breaths delivered early in all spontaneous inspirations. The assist/control mode delivers ventilatory breaths synchronously with all spontaneous breaths and may lead to increased ventilation. From Cleary JP, Bernstein G, Mannino FL, et al. Improved oxygenation during synchronized intermittent mandatory ventilation in neonates with respiratory distress syndrome: a randomized, crossover study. J Pediatr 1995;126:407, with permission. |
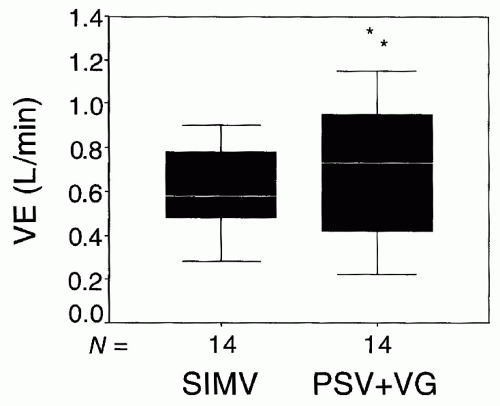 FIGURE 28.9 The relationship between the VE and the mode of ventilation (SIMV or PSV + VG). The difference between the two modes is significant (*p = 0.012). From Olsen SL, Thibeault DW, Truog WE. Crossover trial comparing pressure support with synchronized intermittent mandatory ventilation. J Perinatol 2002;22:461, with permission. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


