A central objective of perinatal medicine is survival of the infant without neurodevelopmental impairment. Improvements in obstetrics and neonatology have greatly reduced neonatal mortality in recent decades, and traumatic brain injury has decreased as well as spina bifida. However, increasing survival of extremely low gestation infants and those with previously lethal conditions has meant that, overall, the incidence of neurologic disorders in infants has not been substantially reduced. Brain injury during pregnancy, delivery, and the newborn period is an important cause of permanent disability and laboratory, and clinical research is beginning to deliver treatments that can prevent brain injury or assist recovery of the brain after injury. In addition to cerebral disorders, there is increased need for accurate diagnosis and prognosis in neuromuscular disorders so that families and rehabilitation services can plan ahead and genetic counseling can be given before the next pregnancy. Because windows of therapeutic opportunity require early diagnosis and have serious consequences if missed, neurologic assessment and diagnosis has acquired a new urgency for the neonatologists.
In this chapter, we discuss the clinical neurologic examination of a newborn infant and outline how to approach common neurologic problems as they present to a neonatologist, including the following:
The full-term infant with encephalopathy after birth asphyxia
The full-term infant in good condition at birth who later develops seizures
The preterm infant with respiratory distress at high risk for intraventricular hemorrhage (IVH)
The preterm infant in apparently good condition but at high risk for periventricular leukomalacia (PVL)
The newborn infant with marked hypotonia with or without muscle weakness
Congenital malformations of the nervous system, bacterial and viral infections, and metabolic derangements are discussed in Chapters 35, 38 and 44.
▪ NEUROLOGIC EXAMINATION OF THE NEWBORN INFANT
The neonatologist needs to know the gestational age of the infant and the postnatal age if the infant is not newborn. The nervous system is in continual development; the brain of an infant at 26 weeks of gestation is anatomically and functionally very different from the brain of an infant at 40 weeks. The pathogenesis of brain injury, anatomic site, clinical presentation, diagnosis, prognosis, and treatment possibilities are very different between 26 and 40 weeks, in ways that they are not between 5 and 10 years of age. Muscle tone and reflexes develop with gestational age.
In addition to the neonatologist’s usual detailed review of the pregnancy, labor, and delivery, the history must include a review of the family medical history and complications encountered during past pregnancies, including a history of congenital anomalies, stillbirths, and genetic or syndromic conditions. The following neurologic examination is modified from that developed by Dr. Lilly Dubowitz (1).
In urgent clinical situations, the neonatologist must examine immediately and will have to adapt the order and content of the examination to the infant’s clinical status. However, in stable situations, the state of quiet alertness is best, not too hungry and not too sleepy, optimally around 2 hours after feeding. There should be sufficient, but not excessive, light. The examiner’s hands should be warm.
Much information can be gained by careful observation without touching:
Is the infant excessively irritable? If crying, is the character of the cry unusual?
Are there external signs of congenital anomaly?
Are there signs of injury, for example, bruising or swelling?
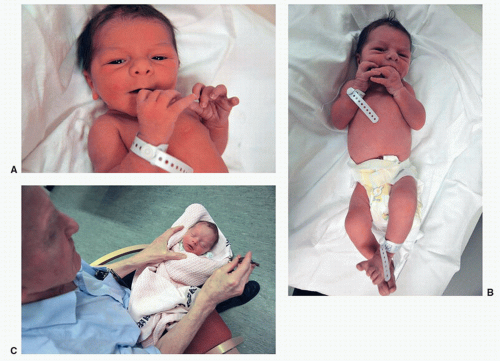
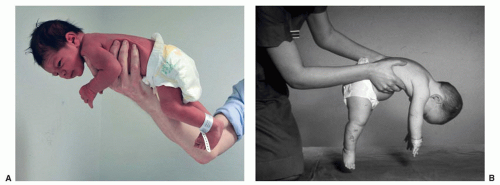
What is the infant’s spontaneous posture? A term infant will usually have flexed limbs (Fig. 46.1B).
Are there spontaneous movements of the limbs? Are there tremors or rhythmic movements?
Are eye movements in all directions and coordinated? Is there nystagmus?
Level of Consciousness
If the neonatologist is lucky, the infant is already awake, alert, and responding to sound, light, and touch.
Reaction to Sound
However, if the infant appears to be asleep, it is useful to begin by shaking a rattle or a bell about 15 cm from each ear. Usually, this will stimulate movement of the limbs or face. This stimulus is about 80 dB and will therefore provide evidence that the infant is not completely deaf. If the sound is repeated a number of times, the infant will eventually stop responding. This “habituation” is a normal response. A healthy term infant will orient toward the source of sound by turning the head toward it (Fig. 46.1C).
Reaction to Visual Stimulus
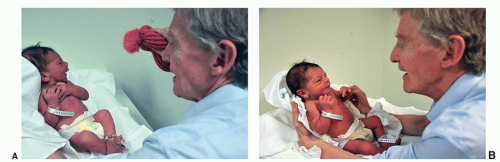
Shining a light in front of a newborn infant will normally induce blinking. If the eyes remain open, pupillary constriction can be observed. If the eyes remain closed, holding the infant vertically and away from bright lights may open the eyes. A healthy, alert term infant will move the eyes (track) to follow a red object (Fig. 46.2A) or a face (Fig. 46.2B) moving horizontally across the visual field. This maneuver may need to be repeated if the infant is not initially in the optimal state; it also reveals abnormal eye movements such as nystagmus, sunsetting, etc.
Examination of the Head
The tension in the anterior fontanelle increases during crying, but a continually tense fontanelle, even when the infant is held upright, suggests raised intracranial pressure. The head circumference should be reviewed and if over 37 or under 32 cm at term, should be remeasured carefully (fronto-occipitally).
Passive Tone in the Limbs
With the infant supine, pull the wrists gently vertically in sequence; observe the angle at the elbow. A term infant will hold the elbow at 100 degrees or less, and an infant under 32 weeks of gestation will have an elbow angle greater than 140 degrees.
Popliteal angle can be measured by flexing each thigh over the abdomen and then, with one finger behind the heel, attempting to straighten the knee. The popliteal angle at term is around 110 degrees, but before 32 weeks is over 140 degrees. Leg traction is measured by holding the foot and lifting the leg vertically. A term infant will hold the knee at 140 degrees, but in an infant of less than 32 weeks, the angle will be larger. Note asymmetry.
Tone in the Neck and Trunk
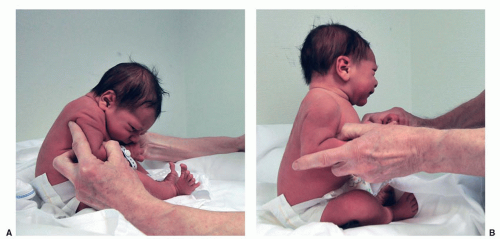
Hold the infant in the sitting position, and then move the trunk slightly forward and allow the head to flex onto the chest (Fig. 46.3A). Wait 30 seconds. A healthy term infant will try to lift the head to the vertical but may not manage or maintain this (Fig. 46.3B). A preterm infant will not achieve this.
FIGURE 46.1 A: This term infant is awake, alert, and looking around. B: This term infant shows a normal posture with arms flexed, hands open (not fisted), and legs semiflexed. C: Shaking a bell beside the head to arouse the infant from sleep and check response to sound.
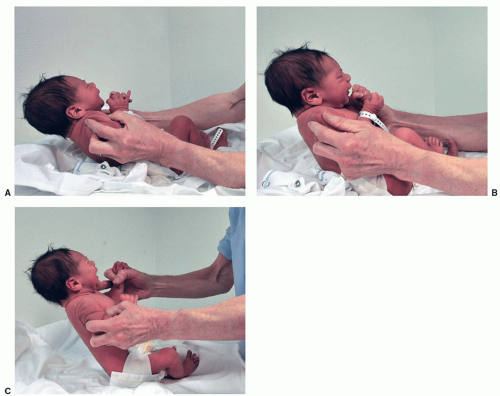
Gently incline the infant backward 30 to 40 degrees. A healthy term infant will maintain the head in line with the trunk (Fig. 46.4A-C), but a preterm infant will not. Neck flexion is normally as good as, or better than, neck extension.
With the infant supine, use gentle traction holding the wrists to pull the trunk up to 45 degrees to the horizontal. A healthy term infant will flex the head in line with the trunk. Preterm infants and those with hypotonia cannot achieve this. It is important to differentiate “head lag” due to general hypotonia from neck extensor hypertonia, in which neck flexion is present but is overcome by tense neck extension.
When in prone suspension (Fig. 46.5A), a healthy infant will normally hold the head in line with the trunk. A hypotonic infant lets the head flop down (Fig. 46.5B), while neck extensor hypertonia will keep the head above the line of the trunk.
FIGURE 46.2 A: The infant is visually following a red object moving horizontally. B: The infant is visually following a face moving horizontally.
Primitive Reflexes
The history of feeding will give important information on the presence of several integrated functions of the nervous system. If the infant has not yet been fed, the sucking reaction to a gloved finger is an important sign. The rooting reflex is elicited with a gentle stroke to the side of the mouth.
The Moro reflex is elicited by holding the infant supine with arms crossed, at a slight angle to the horizontal and then allowing the upper trunk and head to drop toward the horizontal. In a normal term infant, the arms abduct and extend and then adduct and flex (Fig. 46.6A-C). In a normal premature infant, the abduction and extension will occur, but the subsequent adduction and flexion against gravity may be limited. We reserve testing for the Moro reflex for infants with suspicion of brachial plexus injury, for example, after shoulder dystocia. If there is full flexion of the biceps and the whole shoulder can be lifted (deltoid), as in the Moro reflex, this rules out the commonest brachial plexus injury, Erb palsy. Erb palsy involves C5 and C6 and weakens the biceps, deltoid, and supinator muscles (Fig. 46.6D). Asymmetric movement may also be due to pain from a fracture or bone/joint infection. Asymmetric movement is not usually a feature of unilateral cerebral infarction (unlike adult stroke).
FIGURE 46.3 A: From sitting, the infant is gently flexed forward. Initially the head flexes onto the chest. B: The infant tries to extend the head in line with the trunk.
FIGURE 46.4 A: The infant is gently tilted backward and manages to hold the head in line with the trunk. B and C: The infant is tilted further backward and continues to keep the head in line with the trunk without head lag.
FIGURE 46.5 A: In ventral suspension, a healthy infant holds the head in line with the trunk without head lag. B: In ventral suspension, this “floppy infant” has dangling head and limbs.
FIGURE 46.6 A: In preparation for the Moro reflex, the head and the hands are in the midline. B: The Moro reflex. The head is allowed to fall backward. The arms abduct and extend. C: The Moro reflex. After abduction, the arms then flex and adduct and the hands return to the midline. D: Right-sided brachial plexus injury (Erb palsy). The biceps, deltoid, and supinator are flaccid.
TABLE 46.1 Neurologic Examination in the Preterm Infant Differs from That in the Full-Term Infant
Posture is more extended.
Muscle tone is reduced in the neck/trunk and in the limbs.
Muscle strength is reduced.
Sucking and swallowing reflexes are often inadequate for nutrition until 34 wk, and coordination of sucking, swallowing, and breathing may not be present before 32 wk.
Breathing is more periodic with lower gestational age.
The Moro reflex consists only of abduction and extension before 32 wk, and below 28 wk, may be limited to opening of the hands.
Reaction to sound is present down to 24-26 wk of gestation, and some orientation may be found at 28 wk.
Blinking to light is present at 25-26 wk, but pupil constriction may not be present below 29 wk of gestation. Visual fixing and following are usually present from 32 to 36 wk.
Tendon Reflexes
Patellar reflexes can be elicited using two fingers. Clonus at the ankle is an indication of abnormality if maintained for more than three beats. We have not found the grip reflex, the stepping reflex, or the placing reflex useful for neurologic diagnosis.
Neurologic examination in the preterm infant differs from that in a term infant (Table 46.1).
Certain physical signs, if definitely present, should alert the neonatologist (Table 46.2).
▪ DIAGNOSIS OF BRAIN DEATH IN NEWBORN INFANTS
Until recently, diagnosis of brain death in newborn infants (<7 days) was not considered sufficiently reliable to be used for legal purposes. In 2011, the American Academy of Pediatrics and the Society of Critical Care Medicine published guidelines for determination of brain death, which included infants greater than 37 weeks of gestation under 30 days of age (2). Table 46.3 summarizes the clinical criteria. Investigations such as EEG or blood flow studies were not considered to be obligatory. Diagnosis of brain death was not considered to be reliable in infants of less than 37 weeks of gestation.
TABLE 46.2 Warning Signs in Neonatal Neurology
Persistent hypotonia in a term infant (see section on hypotonia).
Persistently increased muscle tone. This may be seen in infants with moderate encephalopathy after birth asphyxia (see section on encephalopathy), traumatic subarachnoid hemorrhage, and meningitis.
Asymmetric reflexes or movements.
Persistent absence of visual following on repeated examinations under optimal conditions. The eyes must be examined for microphthalmia, cataract, retinoblastoma, nystagmus, etc.
Persistent inability to become awake, alert, and responsive (see section on encephalopathy).
Persistent inability to suck and swallow (see section on hypotonia).
TABLE 46.3 Criteria for Diagnosis of Brain Death in Newborn Infants
Gestational age 37+ wk
Identified cause of encephalopathy with reversible causes excluded, e.g., sedative drugs, metabolic intoxication, neuromuscular blockade
Temperature, oxygenation, pCO2, and blood pressure normalized
Flaccid tone with no response to painful stimuli
Pupils midposition or fully dilated and unresponsive
Corneal, cough, gag reflexes absent, sucking and rooting reflexes absent
Oculovestibular reflex (ice water ear irrigation) absent
Apnea. No spontaneous respiration, despite pCO2 rising to 60 mm Hg (8 kPa) and pCO2 increasing by 2.6 kPa
This examination must be confirmed by a second examination at least 24 h later.
▪ THE FULL-TERM INFANT WITH ENCEPHALOPATHY AFTER BIRTH ASPHYXIA
Birth asphyxia means a critical shortage of oxygen during labor and delivery sufficient to produce a lactic acidosis and delay the onset of respiration. Thus, the criteria for birth asphyxia involve low Apgar score, low pH, and increased base deficit. In a much-cited article on the link between birth asphyxia and subsequent cerebral palsy, an Apgar score of 6 or less for more than 5 minutes and a base deficit of greater than 12 mmol/L or pH below 7.0 were chosen as criteria for significant asphyxia (3). Continued need for ventilation at 10 minutes is also evidence that the Apgar score could not have been higher than 6 at 10 minutes. Birth asphyxia does not, per definition, mean that the brain has been injured. A low Apgar score with normal pH and base deficit in umbilical cord blood suggests that the low Apgar score is not due to hypoxia during the hour before delivery and may be due to another cause such as infection, antenatal injury, or congenital anomaly. It is particularly helpful to have both arterial and venous cord blood samples because compression of the umbilical cord (or a knot) may result in normal pH in venous blood from the placenta but low pH in arterial blood from a hypoxic fetus.
Neonatal Encephalopathy
Encephalopathy means a clinically apparent disturbance in brain function. In the context of a newborn infant, the tone, activity, and responsiveness of the infant are abnormal (4). Clinical seizures are not an essential criterion, but, if present, they indicate encephalopathy. The term neonatal encephalopathy is used because, initially, the clinician can recognize the disturbance in brain function, but causation requires more time for investigation.
The term hypoxic-ischemic encephalopathy (HIE) is used when encephalopathy follows delivery with persistently low Apgar scores, a significant metabolic acidosis, and no evidence of other causes of encephalopathy. In some centers, clinical signs of encephalopathy are sufficient, but in other centers, electroencephalography (EEG) is used as confirmation. Modern amplitude-integrated EEG (aEEG) equipment is sufficiently user friendly that a busy neonatologist or neonatal nurse can apply electrodes and can produce useful aEEG recordings with acceptable impedance, particularly if needle electrodes are used in emergency settings. It is important that all term or near-term infants with significant birth asphyxia are urgently assessed neurologically because a provisional diagnosis of HIE now means that the infant should receive therapeutic hypothermia as soon as possible.
Pathophysiology of Hypoxic-Ischemic Encephalopathy
Animal models of HIE have been important in understanding pathophysiologic processes. Myers (5) pioneered such studies in pregnant monkeys in the late 1960s and distinguished between acute total asphyxia and prolonged partial asphyxia.
The acute total asphyxia model involved opening the uterus just before term, clamping the umbilical cord and preventing the fetal monkey from breathing. Blood pressure briefly rose then rapidly decreased, as did pH, which was below 7.0 after 10 minutes. Base deficit typically reached 16 mmol/L by 12 minutes. If cord clamping lasted less than 10 minutes, the fetus could be resuscitated without neuropathologic injury. If cord clamping lasted between 10 and 25 minutes, the fetus could be resuscitated but with neuropathology in the spinal cord, brainstem, and thalamus. If cord clamping continued beyond 25 minutes, the fetal monkey could not be resuscitated.
Prolonged partial asphyxia was produced either by inducing hypotension in the pregnant monkey with halothane anesthesia or by using intravenous infusion of oxytocin to produce prolonged, frequent uterine contractions. If prolonged partial asphyxia was maintained for 2 to 4 hours, the fetal monkey could be resuscitated but usually developed extensor posture and seizures. Neuropathology showed a completely different pattern from that resulting from acute total asphyxia, there being widespread injury to the cerebral hemispheres, particularly frontally and occipitally, the watershed areas between the two main cerebral arteries, and no injury to the brainstem and spinal cord. Basal ganglia injury was only seen in fetal monkeys who had experienced prolonged partial asphyxia followed by acute total asphyxia.
In a newborn pig model, reducing oxygen saturation to around 30% for 45 minutes resulted in encephalopathy with seizures and widespread neuropathology in basal ganglia, thalamus, cortex, and hippocampus (6).
Uterine Contractions and Fetal Hypoxia
During labor, every uterine contraction compresses the arteries bringing oxygenated blood from the mother’s circulation to the placental bed. Normally, the human fetus tolerates this arterial compression because the uterine contractions are short enough and the relaxation periods are long enough to avoid critical fetal hypoxia. In human obstetrics, examples of sentinel events corresponding to acute total asphyxia are umbilical cord prolapse, uterine rupture, shoulder dystocia, and placental abruption. Prolonged partial asphyxia may be seen in the postmature fetus (>42 weeks) in labor with an aging placenta, an intrauterine-growth restricted fetus in labor with placental insufficiency, and in cases of uterine hypertonus due to excessive doses of intravenous oxytocin. In practice, it is likely that many fetuses are subjected to longer than 25 minutes of partial hypoxia but with briefer periods of more severe hypoxia.
Anaerobic Metabolism
Initially, hypoxia-ischemia results in cells switching energy production from aerobic metabolism in the mitochondria to anaerobic glycolysis in the cytoplasm. Glycolysis produces less than 10% of the ATP per gram of glucose than does aerobic metabolism. Thus, essential functions can be maintained for a time during severe hypoxia but at the cost of rapid consumption of glucose and buildup of lactic acid.
Posthypoxic Cell Death and Secondary Energy Failure
An important realization in the 1980s was that processes continued to injure and kill brain cells for hours and days after oxygenation and circulation had been restored. These processes include free radical injury, calcium entry, excitotoxicity from extracellular glutamate, inflammation, and apoptosis. Magnetic resonance spectroscopy showed that the energy status of the brain was restored after resuscitation but then declined after about 24 hours (7). These insights provided a window of opportunity and models of neonatal hypoxic-ischemic brain injury then enabled testing of therapies.
Clinical Signs of HIE
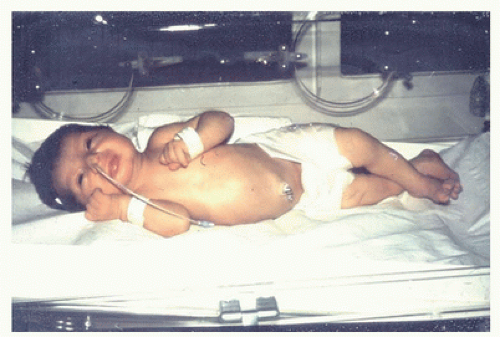
After resuscitation, the neonatologist must look for abnormal neurologic signs to see if encephalopathy develops. The pattern of clinical signs allows the neonatologist to grade the severity of encephalopathy. This was first systematized by Sarnat and Sarnat (4) and is summarized in Table 46.4. The Sarnat grading concerns patterns, and it is not necessary to have all the features listed to allocate a grade. For example, some infants with grade 3 encephalopathy do not have clinical seizures, but they are completely unresponsive and hypotonic and require ventilation. Not all infants with grade 2 encephalopathy have clinical seizures. Some will show hypotonia, but others show pathologically increased trunk tone with neck extensor hypertonia, hands held in a fist, legs adducted, and exaggerated knee and ankle tendon reflexes (Fig. 46.7).
TABLE 46.4 Grade of Neonatal Encephalopathy
Grade 1 (Mild <24 h)
Grade 2 (Moderate)
Grade 3 (Severe)
No seizures
Clinical seizures
Persistent seizures
Mild alterations in tone
Marked abnormalities of tone
Severe hypotonia
Suck intact
Weak suck
Absent suck
Exaggerated Moro
Moro incomplete
Moro absent
Pupils react normally
Pupils constricted
Deviated, dilated, or nonreactive
Hyperalert
Reduced responsiveness to sound, light, touch
Unresponsive
Jittery, tremor on handling
Reduced activity
Distal flexion, proximal extension
No activity
Extended
Impaired breathing
Modified from Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol 1976;33:696-705; Levene MI, Sands C, Grindulis H, et al. Comparison of two methods of predicting outcome in perinatal asphyxia. Lancet 1986;8472:67-69; Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomized trial. Lancet 2005;365:663-670; Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med 2005;353:1574-1584.
Since moderate and severe grades have a poor prognosis and mild encephalopathy does not, two combinations of signs have been used as criteria for moderate/severe HIE (Table 46.5) (8,9,10).
Following resuscitation, encephalopathy develops with signs changing over time. Initially, some severely injured infants hyperventilate, probably because of lactic acidosis. The majority have not demonstrated clinical seizures within the first 6 hours but have done so by the end of the 1st day of life. Some infants show grade 2 encephalopathy signs and then improve, reaching normality within 3 to 5 days. Others will first be in grade 2 and then worsen to grade 3 without ever normalizing.
FIGURE 46.7 A 3-day-old infant with hypoxic-ischemic encephalopathy. The head is partly extended, the arms flexed with the hands tightly fisted, and the legs are extended and adducted.
TABLE 46.5 Combinations of Signs Used as Criteria for Moderate or Severe HIE
Reduced responsiveness with hypotonia or incomplete reflexes
Abnormal pupil response, heart rate, or respiration (10)
Electroencephalography to Support a Diagnosis of HIE
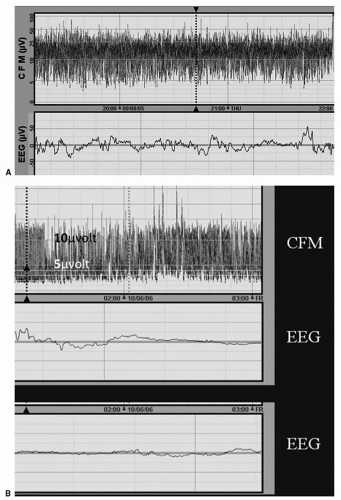
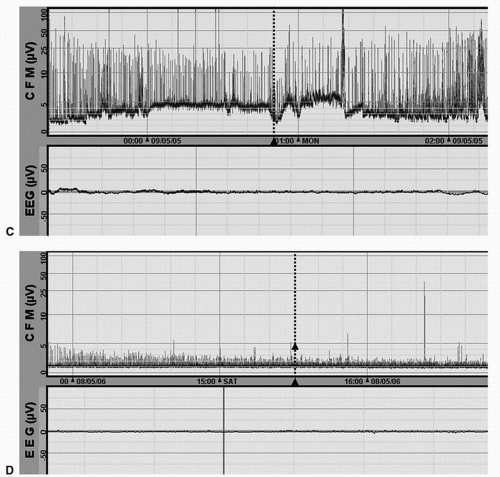
The rapid confirmation of encephalopathy has been facilitated by the use of aEEG. In addition to being relatively straightforward to apply, the screen display shows, in a compressed form, the amplitude and pattern of EEG over several hours. The awake full-term infant has continuous EEG activity, with the amplitude being well over 10 µV (Fig. 46.8A) (11). The mildest response to a hypoxic insult is for the EEG to change from continuous to discontinuous, that is, having periods where the EEG is less active and the amplitude reduces for some seconds and then reverts to the previous normal amplitude (Fig. 46.8B). This is called “discontinuous normal voltage.” If the injury is more severe, the EEG reduces to a low-voltage background with periodic brief bursts of normal amplitude for 1 to 2 seconds with longer periods (over 20 seconds of very low-voltage background in between) (Fig. 46.8C). This is “burst suppression.” If the disturbance is even more severe, there are no bursts, only continuous low-voltage activity. If the disturbance is worse still, there is no electrical activity at all (flat trace) (Fig. 46.8D).
aEEG is valuable because it provides an objective record that can be reviewed by an expert if there is doubt. Animal modeling of hypoxia-ischemia shows that during severe hypoxia-ischemia, the EEG becomes a flat trace or very low voltage. After reoxygenation, the amplitude of the EEG gradually increases over time, the speed of normalizing being inversely proportional to the severity of the brain injury on subsequent neuropathologic grading (6). If one waits long enough in some cases, the EEG will show continuous normal amplitude activity even in the presence of severe brain injury and subsequent cerebral palsy. Continuous aEEG during the first 72 hours is valuable in confirming encephalopathy and in showing trends.
Clinical Chemistry to Support a Diagnosis of HIE
Elevated creatinine, liver enzymes, and cardiac troponin I; prolonged coagulation times; and thrombocytopenia indicate multiorgan dysfunction, useful evidence of total body hypoxia.
Neuroimaging in Diagnosis of HIE
Cranial ultrasound should be done on admission, as it may show evidence of antenatal injury or anomaly, for example, dilated ventricles, corpus callosum agenesis. Apparently normal anatomy on cranial ultrasound on days 1 to 2 does not exclude encephalopathy.
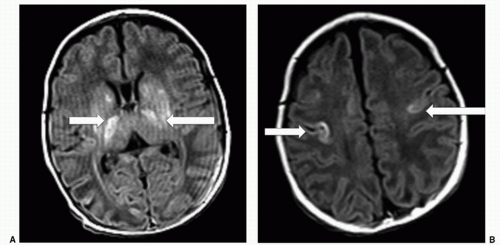
Cerebral magnetic resonance imaging (MRI) taken 4 to 14 days after birth is valuable in confirming HIE and in excluding congenital anomalies and prenatal developmental disturbances. In HIE following acute total asphyxia, MRI typically shows abnormal signal in the basal ganglia and thalamus (BGT) and absence of myelin signal in the posterior limb of the internal capsule (PLIC) (Fig. 46.9A). The brainstem and rolandic cortex may also show abnormal signal (12,13,14) (Fig. 46.9B). Following a more prolonged period of hypoxia, there is typically abnormal signal in the watershed areas (frontal and occipital cortex and subcortical white matter). In severe cases, brain injury in both distributions may be seen in the same child.
Prediction of Outcome in Birth Asphyxia and HIE
An Apgar score of 0 at 10 minutes was followed by death or disability in 94% (15).
In the original study by Sarnat and Sarnat (4), infants with grade 2 encephalopathy who normalized within 5 days had normal developmental outcome, whereas those who had not normalized by 7 days died or were neurodevelopmentally abnormal, typically with cerebral palsy. Overall, grade 2 HIE has been associated with later disability in 20% to 40% and grade 3 HIE with a very high rate of death or disability. The figures vary widely, probably reflecting different definitions of grade 3 and different thresholds for withdrawing life support.
Lactic Dehydrogenase
Lactic dehydrogenase (LDH) sampled within 6 hours of birth gives prognostic information. In one study, all infants with HIE and LDH values less than 2,085 U/L survived without disability, whereas those who died or were disabled had a median LDH value of 3,555 U/L (IQ range 3,003 to 8,705) (16).
Doppler Cerebral Blood Flow Velocity
While ultrasound images are being obtained, pulsed Doppler can be used to measure Pourcelot resistance index, (systolic velocity minus diastolic velocity)/systolic velocity on the anterior cerebral artery. After about 24 hours of HIE, there is pathologic cerebral vasodilatation with, paradoxically, the highest cerebral blood flow being found in the most severely injured infants. This cerebral vasodilatation may be reflected in a low cerebral resistance index (below 0.55). A low cerebral resistance has been found to have a positive predictive value for death or disability of 84% (17).
Electroencephalography
Van Rooij (11) showed that aEEG at 6 hours was predictive of outcome. If the trace showed very low voltage or a flat trace at 6 hours, only 5 out of 65 had normal outcome. If the aEEG had normalized by 24 hours, then 5 out of 6 had normal outcome. If there was burst suppression at 6 hours, 6 out of 28 had normal outcome or mild disability later, and all of these had achieved normal aEEG by 24 hours. All of those who still had burst suppression at 24 hours had poor outcome. The usefulness of aEEG at 6 and 24 hours has been further confirmed in a meta-analysis of prognostic tests (18).
Neuroimaging
Cerebral ultrasound and CT do not provide sufficient detail of injured areas to be useful for prognosis in a clinical setting. On conventional MRI, abnormal signal in the BGT is highly predictive of subsequent cerebral palsy, as is absence of myelin signal in the PLIC. The severity of basal ganglia lesions is useful in predicting the severity of subsequent motor impairment. In a large study of 175 infants with HIE and basal ganglia lesions, the predictive accuracy of severe BGT lesions for severe motor impairment was 0.89 (13). Abnormal PLIC signal intensity predicted the inability to walk independently by 2 years (sensitivity 0.92, specificity 0.77, positive predictive value 0.88, negative predictive value 0.85). Brainstem injury was the only factor with an independent association with death.
Abnormal signal in the cortex and white matter, in the absence of basal ganglia and thalamic abnormality, is not so predictive of cerebral palsy (only 5 out of 84), but severe changes were associated with cognitive impairment, epilepsy, and visual impairment, and there were a variety of behavioral and communication problems (14).
Other Conditions That Can Mimic HIE
Not every infant born with low Apgar scores has suffered critical hypoxia; a number of long-standing disorders of the nervous system can present with a hypotonic infant who does not breathe. This is especially true of congenital myotonic dystrophy and congenital muscular dystrophies and myopathies. Molybdenum cofactor deficiency and isolated sulfite oxidase deficiency can cause seizures of prenatal onset, so that the infant is observed to have seizures very soon after birth (19). High-dose magnesium, benzodiazepine, or opiate therapy to the mother may produce low Apgar scores and a hypotonic, poorly responsive infant but without a severe metabolic acidosis, burst suppression, or seizures. Rarely, severe birth trauma can injure the brain to such an extent that there is delayed onset of respiration. If there is a consistent sequence of obstetric sentinel events, fetal distress, low Apgar score for more than 5 minutes, marked lactic acidosis, clinical encephalopathy, low voltage or burst suppression EEG, and initial cranial ultrasound showing normal anatomy, the diagnosis of HIE is not in doubt. In the cases where important pieces of the HIE jigsaw are missing, other investigations need to be considered including MR imaging, blood levels of ammonia, uric acid and amino acids, urine sulfite reaction and S-sulfo-L-cysteine, and organic acids (see also Chapter 38).
FIGURE 46.8 A: The upper trace shows aEEG with about 3 hours of EEG compressed. In this healthy term infant, there is continuous activity with the upper margin being above 10 µV and the lower margin above 5 µV. The lower trace shows a few seconds of the “raw” EEG with continuous activity at normal voltage. B: The upper trace shows an EEG with the upper margin above 10 µV, but the lower margin is below 5 µV. The lower two traces of “raw” EEG show periods with reduced activity and periods with normal activity. This is discontinuous normal voltage.
FIGURE 46.8(Continued)C: Burst suppression. The upper trace (aEEG) shows the baseline (dark line) has a low upper margin around 5 µV. The vertical lines are brief “bursts” of higher voltage. D: Flat trace. The upper trace shows the base line is around 0 and the lower trace (raw EEG) shows no activity.
FIGURE 46.9 A: T1-weighted MRI axial scan at 8 days. There is abnormal signal (white) in the BGT. The myelin signal in the PLIC is absent. B: The same infant with MRI section at a higher level. There is abnormal signal in the rolandic cortex.
Evidence Base for Therapeutic Hypothermia in HIE
For many decades, the one aspect of neonatal care on which all nurses and neonatologists were agreed was that it was harmful to let a sick baby get cold. It had been known for decades that being cooled during hypoxia protected the brain. This had made possible some early open heart surgery. The demonstration of a lengthy posthypoxic cascade of molecular and cellular processes ending in cell death raised the question of whether hypothermia after hypoxia might reduce brain injury.
First Laboratory Evidence of Hypothermia’s Benefit
The first convincing demonstration in a newborn animal model was in the newborn pig in 1995. Temporary bilateral carotid artery occlusion produced, on MR spectroscopy, severe depletion of energy nucleotides that returned to normal for some hours and then declined in irreversible secondary energy failure. Posthypoxic cooling to 35°C prevented secondary energy failure (20). More research in rats, sheep, and pigs showed that cooling by 2 to 6 degrees for 6 to 72 hours reduced neuropathologic injury, neurobehavioral deficits, cerebral edema, excitotoxic amino acids, free radical indicators, inflammation, and apoptosis. Furthermore, no adverse effects of cooling were identified.
Pilot Clinical Trials
Evidence from three species of newborn animal made it ethical to start clinical trials in human infants in 1998. Because there was still concern that cooling might have harmful effects, the brain was cooled more than the rest of the body using a cooling cap, thereby lowering rectal temperature to 34.5°C. Blood pressure rose during active cooling and could fall significantly during rapid warming (21). Heart rate fell by an average of 14 beats/°C, and rates of 70 to 80 were tolerated without evidence of inadequate perfusion.
Large Randomized Trials
The first large randomized trial (CoolCap) of selective head cooling for 72 hours enrolled infants with asphyxia, signs of encephalopathy, and abnormal aEEG (9). This trial showed a reduction in death or disability at 18 months in the infants who had less severe EEG changes at enrollment. The next trial was conducted by the US National Institute of Child Health and Development Network and used cooling of the whole body to 33.5°C (10), showing significant reduction in death or disability. The TOBY (Total Body Hypothermia) trial cooled the whole body of the infant at 33.5°C for 72 hours, showing a significant increase in survival without neurologic impairment (22). All three of these early trials have followed up infants and have evidence that the protection at 18 months lasts into the school years. A meta-analysis of hypothermia trials in intensive care settings has confirmed that hypothermia reduced both disability and mortality (23) (Table 46.6).
Only gold members can continue reading. Log In or Register to continue