Infections in the neonatal period are frequently fatal and cause significant long-term morbidity among survivors if not treated appropriately and promptly. They are particularly problematic in premature neonates and for the neonate who has other morbidities. Of all the illnesses that affect neonates, infection is the one for which definitive treatment must be started before the diagnosis of the etiology can be confirmed using the technology presently available. Therefore, the neonatologist and other health care providers caring for neonates need to be aware of the subtle clinical presentations that indicate the possibility of infection, the most likely causative agents, the appropriate diagnostic tests, the optimal empiric treatment, and the measures that can be taken to prevent or modify the course of the disease.
Risk of illness due to the transmission of infections from pregnant mothers to their infants and from exposures to infections in the first few weeks of life has been recognized for centuries. That many neonatal illnesses were caused by infectious agents began to be understood in the 1800s. However, it has not been until the technical advances in medical microbiology of the past 50 years that the extent of this phenomenon has been truly appreciated. With the advances in diagnostics has come the ability for identification of exposures to infectious agents during pregnancy, the development of screening programs and institution of prophylaxis programs, and diagnosis of infection of the newborn. This has been particularly evident in the investigations of the transmission of HIV from mother to infant in which the development of PCR testing in the 1990s was necessary to define the risks of transmission and for appropriate diagnosis. Also, with the development of neonatology as a specialty, the emergence of the neonatal intensive care units (NICUs) and the advances in the ability to provide ventilator support and both invasive and noninvasive infant monitoring, along with advances in cardiac and other surgery, has significantly changed the survival of vulnerable children. With that, the epidemiology of neonatal sepsis has significantly changed over time (1,2,3). In North America, prior to the 1950s, group A β-hemolytic Streptococcus (GAS) was the predominant pathogen responsible for neonatal sepsis presenting within the first few days of life. Associated with better obstetrical care practices, infection with these bacteria became less frequent and Staphylococcus aureus and Escherichia coli became the most frequent isolates. Recognition of the risk factors for acquisition of these bacteria led to changes in antiseptic practices in the delivery room and in the newborn nurseries and the implementation of screening for maternal bacteriuria. Beginning in the early 1970s, Group B β-hemolytic Streptococcus (GBS) became the most prevalent bacteria in North America. Development of screening programs in pregnancy, treatment during labor and delivery of colonized and/or high-risk mothers and empiric treatment of high-risk infants where maternal prophylaxis was missed have significantly reduced the impact of this organism in the early neonatal period. During the past two decades, the most common infection causing neonatal sepsis has been coagulasenegative staphylococci associated with infected central venous or arterial catheters. However, the scene is again changing as a result of preventative strategies for catheter-related infections. The concerns now are becoming centered on infections with bacteria that are either overtly resistant to commonly used antibiotics such as methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococcus (VRE) or those in which antibiotic resistance can be induced with exposure to the antibiotic such as many of the extended-spectrum β-lactamase (ESBL) or carbapenamase-producing gram-negative bacteria (4,5,6,7). The emergence and spread of these bacteria has made the empiric treatment of sepsis in the neonate considerably more complex than it was only a decade ago.
Neonates are a special population from an infectious disease perspective due to several factors. They are the one patient population in which there is no resident bacterial population on their skin or at their mucosal surfaces (8). Colonization does begin rapidly within the first few hours of life, but the establishment of the infant’s permanent resident bacterial flora takes several months (9). Recent studies, in part due to the Human Microbiome projects (http://commonfund.nih.gov), have helped to detail how neonates acquire their normal bacterial flora. In general, infants acquire their resident bacteria from their mothers with gram-positive organisms being the initial colonizers followed shortly thereafter by gramnegative bacilli and then anaerobic organisms. The sequence of organism acquisition may vary depending on method of birth with those born vaginally acquiring their “pioneer” organisms from the maternal genital and enteric flora while those born by Caesarean section may acquire skin organisms first (10). Residence in an NICU tends to alter this somewhat with a delay in colonization likely related to increased antibiotic use and an increased chance of colonization with hospital-acquired strains of gram-negative bacteria (11,12). Colonization changes over the first year of life in an age-dependent way, which likely reflects the developing immune system. By 1 year of age, each child has established his or her resident bacteria pattern that appears to stabilize provided there is not excessive antibiotic pressure. Fungal colonization of the mucosal surfaces is inversely related to gestational age (GA) with infants of lower gestational ages having higher levels of colonization (13). In general, the source of early or initial fungal colonization is from the mother. Colonization of infants in NICUs after 2 weeks of life tends to originate from the NICU and may involve species different from those that are maternally acquired. Infants do acquire organisms that are sexually transmitted in adults, which may persist for months or years if not diagnosed and treated. However, not all sexually transmitted infections necessarily cause disease. Mycoplasma hominis and Ureaplasma urealyticum are two such organisms that are transmitted frequently to premature infants and can establish colonization of the respiratory tract, eyes, and vaginal tract in girls for several months without a clearly established role in infant illness (14,15). In general, recovery of a pathogen in the clinical context of disease usually means the neonate is acutely infected.
Neonates have a relative immune deficiency compared to both older infants and adults (16). A complete discussion of the immune system and its development is not the subject of this chapter. However, in brief, the immune system is divided into the innate immune system, which is present from birth and does not require a previous exposure of the individual to a specific pathogen, and the adaptive immune system that does. The innate immune system recognizes microbial pathogens through pattern recognition receptors (PRRs), which identify various molecular microbial components as “not being human” (17,18). In general, its components do not permanently change with exposure to microbes although there may be some changes associated with ageing. Neonates are almost exclusively dependent on the innate aspect of the immune system for the initial defense from infection, as they have no preexisting adaptive immunity (17,18). In general, they have a Th2 bias in their adaptive immune responses, which means that the Th1 response is relatively muted (19,20,21). Therefore, there is a relative reduction in the production of opsonizing antibodies, induction of cellular cytotoxicity, and macrophage activation. This, coupled with immature complement-activating systems and lower levels of fibronectin, results in higher risk of disease (22,23,24). Thus, there is a relative decrease in the ability of the neonate to defend against intracellular pathogens (e.g., mycobacteria, viruses, intracellular bacteria) and respond to many vaccines. Over time with exposure to multiple antigens, a more balanced response occurs. During the neonatal period, in addition to a Th2-biased immune response, it is usually the infant’s first exposure when exposed to a pathogen, so there is no memory response and all adaptive immune responses are primary. The detection of a primary immune response, such as a pathogen-specific IgM or IgA antibody, can be used to help make the diagnosis of infection.
The incidence of infectious diseases among neonates varies considerably depending upon the geographic location, the prevalence and incidence of infections in women of childbearing ages, the presence and utilization of screening programs and use of prophylactic antibiotics, whether an infant is born at term versus prematurely or extremely prematurely, and the various policies related to diagnosis and screening for infections as well as the infection prevention and control (IPC) procedures.
The consequences of infection depend largely on the timing of transmission to the infant (prenatally, perinatally, or after delivery), whether it is a primary maternal infection, the ability to make a quick and accurate diagnosis, rapid institution of appropriate antimicrobial agents, any underlying condition, and the gestational age of the newborn.
Infections in the newborn period are primarily acquired from the mother during gestation, during labor and delivery, or in the neonatal period. In addition, potential pathogens may be acquired from other family members, health care providers, contaminated equipment or supplies in the nursery or home, from visitors to the nursery or home, or in the community at large if newborn infants are taken out to areas such as shopping malls. The clinical presentations depend on the nature of the organisms involved as well as the timing and route of infection (25,26). For example, the effects of congenital rubella are dependent on the stage of development of the infant organ systems at the time of the infection because the major morbidity of rubella is due to progenitor cell loss (27). Infants who acquire bacterial infections prior to the onset of labor tend to present with clinical sepsis at birth or within a few hours of delivery while those who acquire the organisms at the time of delivery present with signs of sepsis days to weeks after delivery.
▪ CONGENITAL INFECTIONS
The neonate may be born with a known maternal history of a pathogen potentially causing congenital infection thus leading to the need to confirm the diagnosis, or alternatively, clinical findings in the infant trigger a suspicion that an infant has a congenital infection leading to the need to determine that diagnosis. Both scenarios require a treatment and management plan to be developed. Not all mothers who acquire an infectious agent during gestation will transmit the agent to their infants. Not all infants who acquire such an agent from their mothers will clinically manifest any signs of infection. The pathogenic nature of the infectious agent, the gestational age of the infant at the time of maternal infection, and maternal previous immunity to the agent all play important roles. Determining whether an infant is infected may be done prenatally by evidence of associated infant abnormalities on fetal ultrasound. For some infants, detection of the pathogen by amniotic fluid sampling may be helpful. However, the ultimate determination of infant congenital infection is in the immediate period after birth, irrespective of whether the infection was suspected prenatally or at the time of birth.
Classically, the agents that are most frequently associated with congenital infection have been referred to as the TORCH organisms (Toxoplasmosis, Other, Rubella, Cytomegalovirus and Herpes). Since the “other” in the mnemonic now stands for a significant number of potential pathogens, it is now considered to be somewhat limited, and a variety of mnemonics have been proposed to help ensure that all potential agents are considered when an infant presents with suspected congenital infection. However, use of maternal identifiable risk factors and knowledge of the local prevalence and incidence of potential infections is a more effective way of developing a diagnostic plan (28,29).
TABLE 44.1 Common Signs Associated with Congenital Infections
Sign
Infectious Agents to be Considered in the Differential Diagnosis
It is important for health care providers to consider whether there may be a congenital infection at the time of the initial examination of the infant. Clinical clues as to whether an investigation for congenital infection(s) is warranted and the most likely organisms are found in Table 44.1. Information concerning the specific agents including investigations and management follow.
Cytomegalovirus
Cytomegalovirus (CMV) is an enveloped double-stranded DNA member of the herpes virus family. It only infects humans. Like all herpes family viruses, it persists for life after the primary infection with periodic reactivations. It is a slow-growing virus, and it may take several days to be detected using viral cultures (30). There is only one serotype, but there are several different strains that can be detected with molecular analysis of DNA (31). To date, there is no licensed vaccine for prevention. It can be transmitted sexually, through breast milk, through close contact with infected oropharyngeal secretions, or blood transfusion. Young children excrete the virus in high titers and are a significant source of the virus for other children and adults. Therefore, there is an increased risk for seronegative pregnant women who care for infected young children or have their children attending day care (32,33,34,35). CMV is transmitted to the fetus through the placenta. It is the most common congenital viral infection in the United States and Canada (36,37,38,39,40). Seroprevalence studies among women of childbearing age have shown that the seroprevalence of CMV is 60% to 99%. Lower antibody prevalence is associated with upper socioeconomic status and living in highly developed nations or communities. Seropositivity also correlates with fecundity. The risk of symptomatic congenital CMV is highest when pregnant women acquire a primary CMV infection during pregnancy—on average 40% but ranging from 24% to 75% (32,33,34,35,39,41,42,43,44,45,46,47). The risk that a seronegative woman will acquire CMV during her pregnancy is from 0.7% to 4.2%, which is similar to that of nonpregnant women. The risk that a seronegative mother will seroconvert and have a subsequent pregnancy that is affected by CMV decreases from 25% to 4% when the interval between pregnancies extends from under 2 years to more than 4 years. The annual seroconversion rate in day care workers is from 8% to 12% depending upon the socioeconomic status of the day care attendees and the age of the day care providers. Women who reactivate their viral infection during pregnancy or who are reinfected with another strain may also transmit the virus to the fetus, but the deleterious effects on the fetus is considerably less with the possible exception of the incidence and severity of hearing loss (48,49,50,51). Unfortunately, more than 90% of pregnant women with primary CMV infection and close to 100% of those who reactivate will be asymptomatic. Those who do have symptoms generally have a mononucleosis-like disease. Fever, lymphadenopathy, weakness, myalgia, lymphocytosis, and/or elevation of some hepatic transaminases are some of the symptoms and signs that might trigger an investigation. Diagnosis of acute CMV infection in the mother can be done by determination of seroconversion during pregnancy, rising IgG titers, and/or the presence of IgM antibodies. IgM antibodies can persist up to 8 months, which might confuse the diagnosis early in pregnancy (52). CMV-specific IgG avidity is low in the months immediately after an acute infection and rises over time, so these tests may be of use when available (53). Determination of maternal acute infection helps determine if a fetus is at risk of congenital infection, but it is not diagnostic of fetal infection. Detection of the virus in high titers in the amniotic fluid is associated with fetal infection resulting in symptomatic infants at birth (54). The presence of lower viral titers has been seen in severely symptomatic infants, asymptomatic infected infants, and uninfected infants and so is not as predictive of infant disease. This has been shown somewhat dramatically in case reports of twins with dichorionic placentas and other multiple pregnancies in which the fetuses with high viral loads in the amniotic fluid were symptomatic at birth while the others with low viral loads were asymptomatic or not infected. Maternal treatment with ganciclovir or valganciclovir with or without the addition of anti-CMV antibody-rich intravenous immune globulin (IVIG) has been proposed as a method to reduce the effects of in utero CMV infection in the situation where CMV is detected in amniotic fluid. Although promising, to date, there is insufficient evidence to recommend these therapies routinely, but they may be considered by some clinicians on an individual basis (55,56,57,58).
Pathophysiology and Clinical Presentation
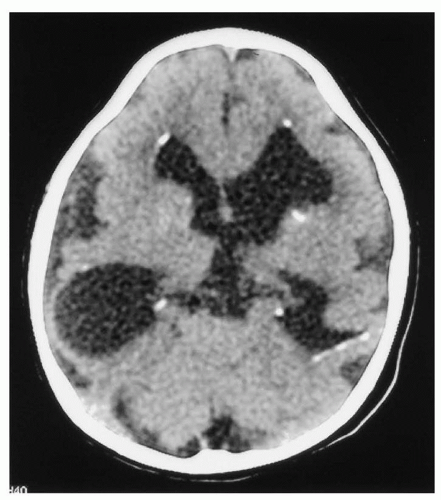
Overall, congenital CMV is estimated to affect 0.4% to 2.3% of all live births (59). It is one of the major nongenetic causes of sensory hearing loss and neurodevelopmental delay (60,61). Of these infants, only approximately 10% are symptomatic at birth or in the neonatal period (49,59). The mortality rate among symptomatic infants varies from 5% to 30% (60). It has been difficult to determine whether there is a difference in risk of disease based on the gestational age of the infant at the time of infection. Congenital CMV is a multisystem disease, and the following are seen in more than 50% of infants affected at birth: hepatosplenomegaly, jaundice, conjugated hyperbilirubinemia, thrombocytopenia, petechiae, microcephaly, seizures, hypotonia, intracranial calcifications, chorioretinitis, and unilateral or bilateral hearing loss (62,63,64). The intracranial calcifications seen in congenital CMV infections tend to be periventricular in location as is seen in Figure 44.1. Other neurologic abnormalities may include intraventricular hemorrhages, periventricular necrosis, cerebral hypoplasia, periventricular leukomalacia, hydrocephalus, and porencephalic cysts. Over time, neuromotor and psychomotor delay is diagnosed in approximately 50% of survivors. Infants with abnormal CT scans at birth have a 90% risk of developing one or more significant long-term neurologic sequelae (significant mental or psychomotor delay, seizures, cerebral palsy, or hearing loss) (65). However, 30% of symptomatic infants with a normal CT scan at birth will do so as well. Cerebral MRI scans may be both more sensitive and specific in predicting ultimate outcomes (66,67,68). Cranial ultrasounds will also detect a large number of abnormalities related to poor prognosis (67). Children who are asymptomatic and remain so until a year of age have similar neurologic testing as uninfected controls. Chorioretinitis is the most frequently diagnosed optic abnormality. Occasionally, this is the only abnormal finding. Although it is usually present at birth, some infants will develop it later in early infancy. Spontaneous resolution has been reported, but it usually progresses to significant visual impairment. Other optic abnormalities include optic atrophy, microphthalmia, cloudy cornea, corneal opacities, optic nerve hypoplasia, optic nerve coloboma, nystagmus, anophthalmia, and cytopia. Hearing loss can vary from mild to profound and occurs in about 50% of symptomatic survivors but also in from 7% to 13% of those with subclinical infections. Bilateral hearing loss is associated with maternal primary infection. It may be present at birth. Hearing deteriorates over the first 18 months in about 50% of infants. Dental defects have been observed in 40% of surviving symptomatic infants and 5% of asymptomatic ones. In addition, infants infected with CMV may develop pneumonia and/or colitis. A wide variety of other congenital malformations have been described in infants with congenital CMV but not shown to be related to the infection.
FIGURE 44.1 Computerized axial tomogram of a microcephalic 3-monthold boy with symptomatic congenital CMV following primary maternal gestational CMV infection. Shown are subependymal periventricular calcifications, enlarged ventricles and CSF spaces, and loss of periventricular and subcortical white matter volume.
Diagnosis
Diagnosis of congenital infection depends upon demonstrating the presence of the virus at birth (45). Generally, this is done by isolating the virus from saliva or urine specimens collected within 2 weeks of birth. Isolating the virus from specimens collected after 3 weeks of age may represent either congenital or perinatal infection. Therefore, it is important to consider the possibility of congenital infection soon after birth in order to make a definitive diagnosis of infection. CMV cultures using shell vials enable the diagnosis earlier. While CMV may be detected in urine by DNA, ELISA, or electron microscopy, viral culture remains the most sensitive method of diagnosis. CMV IgM antibodies are positive in approximately 70% of infected infants. To determine if CMV is present from blood samples, use of PCR from serum specimens is preferential with 100% sensitivity as opposed to culture (28%) and antigen detection studies (43%) (69). CMV can be detected from the blood spots on newborn screening cards by PCR testing and may be used for diagnosis if other samples were not collected during the 2-week diagnostic window with the appreciation that if not appropriately stored, there may be false-negative results due to degradation of the sample and false-positive results from crosscontamination from other cards (70,71).
Treatment and Management
The optimal treatment of congenital CMV infection remains to be determined (42). Ganciclovir and valganciclovir are the antiviral agents currently used for the treatment of symptomatic CMV-infected infants (72,73,74,75,76). They are generally recommended for use for viremic infants with a viral sepsis-like syndrome including pneumonitis, refractory thrombocytopenia, sight-threatening retinitis, and colitis. Infants with sensory hearing loss, microcephaly, and other central nervous system (CNS) manifestations, and other congenital CMV-related diseases may benefit from therapy. Determination of the CNS status of infants with CMV infection by cerebral MRI if possible, or CT scan or ultrasound if not, is important both for treatment decisions and for discussions of the infant’s prognosis with parents. Infants should be assessed by an ophthalmologist familiar with the ocular manifestations of congenital CMV. Infants should also have their hearing assessed. In addition, the infant’s complete blood count (CBC), renal and hepatic functions should be determined. Infants with severe congenital CMV can be treated with IV ganciclovir (6 mg/kg/dose administered IV every 12 hours) for 6 weeks; valganciclovir (16 mg/kg/dose administered orally every 12 hours) for 6 weeks or a combination of a short course of ganciclovir IV therapy followed by oral therapy with valganciclovir to complete a 6-week course. Whether a 6-month course of antiviral therapy would provide additional benefit is being studied, and preliminary results indicate that there may be additional benefit from a longer treatment course (75). Generally, CMV viral loads are not monitored during treatment, and viral loads will increase once treatment is discontinued. Infants diagnosed with congenital CMV should have close follow-up with developmental, hearing, and ophthalmologic assessments. Routine IPC precautions are sufficient, but health care providers should be adherent to hand hygiene recommendations.
Toxoplasmosis
Toxoplasmosis is caused by the protozoan Toxoplasma gondii, which is an obligate intracellular parasite (77,78). It is a zoonotic disease in that part of the life cycle of the pathogen involves infection of animals. The life cycle is somewhat complex. There is an enteroepithelial sexual phase that occurs only in felines and an extraintestinal phase that takes place in both the definitive host (e.g., cats) and intermediate hosts (e.g., humans). Susceptible cats acquire T. gondii through either ingesting oocysts or parasiteinfested tissues of other animals. Some of the organisms released in the cat’s intestines after ingestion invade the gut epithelial cells and undergo sexual differentiation into microgametes and macrogametes. These gametes then fuse to form a zygote. After a rigid wall forms around the zygote, it is excreted in the cat’s feces as an oocyst. Acutely infected cats will shed millions of oocysts daily for 1 to 3 weeks after infection. The parasites that do not undergo sexual differentiation can penetrate the gut wall and spread to other organ systems. This happens with susceptible animals and humans. The tachyzoite is the actively proliferating form that is found in organ systems during the acute phase of systemic infection. They gain access into the cytoplasm of cells, multiply rapidly, and cause the cells to burst, thereby releasing parasites to infect neighboring cells. This process leads to areas of necrosis that are usually surrounded by inflammatory cells. Over time, the process is halted by specific cellular and humoral immune responses in immunocompetent individuals. More extensive infection occurs among those who are immune suppressed. However, regardless of the host’s immune competence, T. gondii parasites can remain viable for years as slowly propagating bradyzoites inside cysts. The presence of these cysts is usually asymptomatic, and they are commonly found in the brain, eyes, myocardium, and skeletal muscle. However, they can reactivate and produce serious illness such as encephalitis and pneumonia in individuals if they become immune suppressed. Interestingly, of the three strain types: types I and II are generally involved in congenital infections and type II is also associated with HIV/AIDS while type III is found in animals (79).
Humans acquire T. gondii primarily through ingestion of oocyst-contaminated water, from contaminated soil, dust, or cat litter by inadvertent mouth contact with unwashed hands, or from consumption of cyst-containing raw or undercooked beef, pork, mutton, lamb, or chicken or contaminated raw eggs (80). Accidental contamination of laboratory workers has occurred. In addition, transmission has occurred through transfusion of infected blood, blood products, and organ transplant. However, the main route of human-to-human transmission is transplacentally.
The percent of women of childbearing age with antibodies to T. gondii varies considerably worldwide from 0% to 90% (77,81). The incidence of infections has decreased in some areas due presumably to changes in food production. Women living in lower socioeconomic circumstances or who work in soil-related professions have a higher likelihood of being seropositive. Lifelong vegetarians have a lower rate of seropositivity compared to those who eat meat. The likelihood of seropositivity increases with age. Interestingly, studies have not related current cat ownership to the risk of being seropositive, but it is considered to be a risk factor for a seronegative pregnant woman to acquire the organism. One significant risk for a seronegative pregnant woman is to move from an area of low prevalence to one that is high. Specific risks for acquisition of T. gondii in pregnancy include consumption of cured pork, raw meat (including tasting while preparing foods), eating unwashed raw vegetables or fruits, infrequent washing of hands or kitchen utensils after preparation of raw meat before handling another food items, contact with soil, and the cleaning of cat litter boxes (82).
The actual incidence of congenital toxoplasmosis is not known. Surveys have shown a minimal incidence of 0 to 10 per 1,000 live births with a lower incidence reported in North America compared with regions in Europe (83,84).
There is no vaccine against T. gondii. Prevention of congenital toxoplasmosis involves educating susceptible women how to avoid coming into contact with the parasite. Cats that are kept indoors and fed dried, cooked, or canned food have a low risk of becoming infected. That said, contact with cat feces should be avoided. Disposable gloves should be used when cleaning the litter box, and this should be done preferably by another household member. Kitty litter boxes should be emptied of feces daily, and periodically, the empty litter box should be disinfected with boiling water. Gardening is another risk activity for inadvertent contact with cat feces, so gloves should be worn and strict attention paid to hand hygiene. Children’s sand boxes should also be covered to avoid inadvertent contact with cat feces. Meat should be cooked appropriately. Women should avoid touching their eyes and mouth when handling raw meat and should wash their hands immediately afterward. Care should be taken to clean kitchen surfaces after preparation of meat-containing dishes. Fruits and vegetables may be contaminated with oocysts and so should be peeled and/or washed before being consumed. Secondary prevention includes identification and treatment of women who become infected immediately before or during pregnancy. Presently, only a few regions with high prevalence rates of toxoplasmosis, such as France, have a routine screening program in pregnancy.
Pathophysiology and Clinical Presentation
In pregnant women, the infection is asymptomatic in 80% to 90% (85). Lymphadenopathy is the most common clinical sign among those who do have symptoms (86). The involved lymph nodes are primarily in the head and neck and may often involve a single node. An estimated 1% to 5% of acute infectious mononucleosis is actually toxoplasmosis. Pregnant women may develop hepatitis, pneumonia, myocarditis, encephalitis, and deafness, but these manifestations are rare (87). Ocular involvement does occur, and when it does, it usually involves chorioretinitis and then retinochoroidal scars. Type I T. gondii infections are the ones that have been associated with severe ocular disease in immunocompetent individuals. Psychiatric complications including psychosis resembling schizophrenia, anxiety, and depression have been described in association with T. gondii acute infections. Fulminating disease is common in immunosuppressed patients such as pregnant women with advanced HIV infection (AIDS).
T. gondii causes transplacental infection in the fetus in around 1% if the infection occurred in the months immediately preceding the pregnancy, 10% to 25% of untreated pregnancies with acute infection in the first trimester, 20% to 54% in the second trimester, and 65% to 70% in the third trimester (86,88,89,90). Disease occurs despite the maternal immune response (91). Timely and appropriate maternal therapy reduces the risk of transmission by at least 50%, and the percentage of infants who manifest severe congenital toxoplasmosis is less if the mother receives therapy during pregnancy.
At least two-thirds of infants with congenital toxoplasmosis will not have apparent disease on general examination at birth (77,83,92,93,94,95,96,97). However, if carefully looked for, one-third of these infants will have some abnormality attributable to the infection such as an abnormal cerebrospinal fluid (CSF) examination with pleocytosis and/or elevated protein (20%), chorioretinitis (15%), or intracranial calcifications (10%). Over time, untreated infants will begin to show manifestations of the disease.
Symptomatic congenital toxoplasmosis can be mild, moderate, or severe at birth (77,98,99). It can involve multiple organ systems or present as an isolated abnormality, specifically hydrocephalus, hepatosplenomegaly, or prolonged hyperbilirubinemia. Between 25% and 50% of symptomatic infants are born prematurely. Only approximately 10% of affected infants have severe disease at birth, of whom 10% die and remainder generally have major neurologic abnormalities including mental retardation, seizures, spasticity, and visual defects. Systemic manifestations of congenital toxoplasmosis include fever, jaundice, anemia, hepatomegaly, splenomegaly, and/or chorioretinitis.
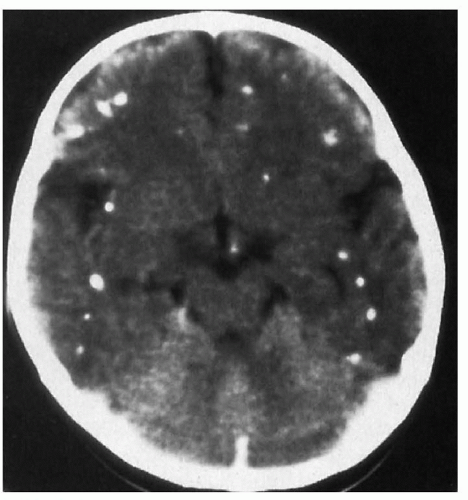
Neurologic abnormalities include encephalitis, seizures, hydrocephalus, and/or intracranial calcifications. CNS involvement is common. Parenchymal brain lesions usually involve a vasculitis of surrounding blood vessels resulting in thrombosis and infarction. If substantial, this can lead to obstruction of the aqueduct of Sylvius resulting in enlargement of the third and lateral ventricles and the development of hydrocephalus. Occasionally, hydrocephalus is the only manifestation of congenital toxoplasmosis. It may present at birth or later and be static or progress to requiring the placement of a shunt. Diffuse intracranial calcifications occur in 10% to 20% of infants but are found in up to 70% of those with symptomatic disease at birth as is seen in Figure 44.2. Although they may increase in number and size in some untreated infants, with treatment, 75% will decrease or totally resolve within a year. Other neurologic findings include bulging fontanelle, encephalitis, hydranencephaly, hypotonia, paralysis, spasticity, opisthotonus, microcephaly, swallowing difficulties, and/or proteinorachia. Radiologic CNS findings may show hydrocephalus, porencephaly, encephalomalacia, and/or cortical atrophy, which are consistent with an old insult during gestation. Alternatively but less commonly, they show single or multiple hypodense lesions with contrast ring enhancement, which imply an acute and active process.
FIGURE 44.2 Computerized axial head tomogram of a 5-month-old girl with congenital toxoplasmosis. Notice the diffuse parenchymal calcifications and the prominent subarachnoid space bilaterally.
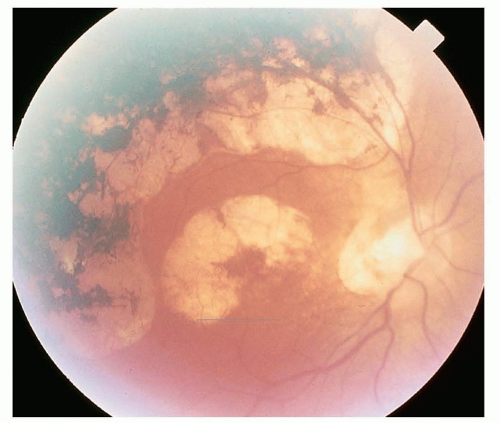
Ocular toxoplasmosis can have a multitude of clinical presentations, which may include chorioretinitis, chorioretinal scars, iritis, leukocoria, microphthalmia, nystagmus, optic atrophy, optic coloboma, retinal folds and traction detachments, granulomas in the posterior pole, strabismus, small cornea, and/or cataracts (100,101,102) (see Fig. 44.3). Chorioretinal scars are the most common finding and are usually detected at the periphery. Macular scars are seen in up to 75% and may be bilateral in one-quarter of cases. These patients have markedly decreased visual acuity.
Unfortunately, most infants with severe symptomatic congenital toxoplasmosis who survive will have significant sequelae despite therapy. This most commonly involves developmental delay and blindness. Those who are born with a subclinical infection and are not treated will all develop eye disease by 10 to 20 years of age and approximately 50% will go on to develop neurologic sequelae (77). Children born with subclinical infection who receive treatment have a better long-term prognosis, but 75% will still have some evidence of retinal disease although the clinical severity appears to be less. Both untreated and treated infants can have recurrences of ocular toxoplasmosis, but this is less frequent among treated infants (40% to 60% compared to 76% to 82%).
FIGURE 44.3 Multiple chorioretinal scars in a patient with a history of congenital toxoplasmosis. From Gold DH, Weingeist TA. Color atlas of the eye in systemic disease. Baltimore, MD: Lippincott Williams & Wilkins, 2001.
Diagnosis
Acute toxoplasmosis in an adult is not likely to be diagnosed clinically. Acute symptomatic infections are usually only investigated when the serologic testing for Epstein-Barr virus (EBV) infection or the Monospot is negative, and there is clinical concern about toxoplasmosis. Reactivation is usually suspected in compatible clinical situations when there is immune suppression and previous residence in a high endemic area. Generally, diagnosis is based on serologic testing; however, the organism can be isolated from tissues or detected with antigen detection studies and PCR techniques.
Serologic diagnosis of a recent infection in a pregnant woman and congenital infection in an “at-risk” infant is important to make but can be complicated due to the nature of the immune response to this pathogen and the sensitivity/specificity of the antibody testing (77,98,103,104,105,106). The Sabin-Feldman dye test is the traditional serologic test. A titer that is greater than 1:256 is considered positive. As this test requires live parasites to perform, it has been replaced by newer more laboratory friendly technologies that use killed antigens in most laboratories.
Toxoplasma-specific IgM antibodies can be measured by IFA, ELISA, or IgM immunosorbent agglutination assay (IgM-ISAGA). False-positive IgM-IFA or IgM-ELISA can occur in the presence of rheumatoid factor or other lipid factors in the blood that are extracted along with the parasite lipids during testing. Alterations in the ELISA testing by using a double sandwich technique (DS-IgM-ELISA) can correct this. Toxoplasma-specific IgM antibodies can be detected 1 to 2 weeks after acute infection. They also can be detected for several years after infection if the IgM-ISAGA or DS-IgM-ELISA methods are used. Therefore, the detection of toxoplasma-specific IgM antibodies in a single sample from an adult is not necessarily proof of a recent infection. Specificity testing can be helpful as highly specific IgM antibodies coupled with high titers of IgG antibodies (1:1,000 or higher) as measured by either the Sabin-dye test or IFA indicate a recent infection. Low specific IgM titers measured by DS-IgM-ELISA or IgM-ISAGA are generally more often found in individuals whose infection occurred several months previously. IgM-IFA tests are less sensitive and are positive in 60% to 70% of adults with acute infection and only 25% to 50% of infants with congenital toxoplasmosis. Toxoplasma IgG antibodies as measured by the dye test, IFA, or ELISA usually appear early in an acute infection and peak at around 2 months and then fall gradually but remain detectable for years afterward. In contrast, toxoplasma IgG titers measured by indirect hemagglutination assays are not detectable for several months after infection. A high IgG titer is suggestive of a recent infection but again is not necessarily proof of it. Avidity testing can be done to try to determine whether the infection is recent, and low avidity is seen in acute infections, and high avidity is seen in chronic ones. Low avidity can persist up to a year after acute infection. IgG avidity greater than 20% implies that the infection occurred more than 20 weeks previously. Therefore, a single positive high-avidity toxoplasma IgG titer in the first few months of pregnancy is indicative of a remote infection relative to the pregnancy. Antitoxoplasma IgA antibodies against one of the surface proteins of the tachyzoites are present in almost all acute infections and disappear after approximately 6 months to a year. They are rarely seen in patients with chronic infections. Similarly, specific IgE antibodies appear with acute infection and disappear over the next 4 to 8 months.
As stated previously, the determination that a pregnancy may be complicated by toxoplasmosis can be complex (107).
A recent T. gondii infection can be diagnosed in an immune competent pregnant woman if seroconversion is detected. The timing of the infection can be narrowed down to the time period between the negative specimen and the one in which antibodies were detected.
If the initial specimen was collected immediately prior to pregnancy or in early gestation, then the diagnosis of toxoplasmosis in pregnancy would be established.
If there is a longer time period between testing, the nature of the antibodies would need to be further characterized to determine whether the fetus is at risk of toxoplasmosis (see below).
Alternatively, if the initial specimen collected from a pregnant woman is positive, the determination of a fourfold rise or greater in antibody titers in a repeat serum sample collected 3 to 6 weeks later would also establish the diagnosis of toxoplasmosis in pregnancy.
For an immune competent pregnant women with no preceding serologic studies whose initial antibody titers are positive and stable on repeat testing, further studies of the nature of the antibody response is also necessary to determine whether the fetus is at risk.
Absence of IgM antibodies and a negative rheumatoid factor test would rule out a recent infection and the fetus would not be considered to be at risk
Positive IgM titers with high IgG titers of low avidity would indicate a recent infection, and the fetus would be considered at risk.
The presence of IgA or IgE titers would indicate a recent infection and the fetus would be considered at risk.
An immunodeficient pregnant women in whom toxoplasmosis is suspected may not develop a serologic response, and detection of the parasite in body fluids or tissues would be needed.
Specific diagnosis of intrauterine infection with T. gondii can be done with amniocentesis and ultrasound-guided cordocentesis (103,108). If available, samples can be sent for parasite isolation using tissue cultures or injection into mice which is the most sensitive method to determine fetal infection (≈80%). Fetal blood that is documented to be free of maternal blood contamination can be assayed for toxoplasma-specific IgM or IgA antibodies, but the sensitivity is low (≈20% to 50%). Congenitally infected fetuses may have high levels of total IgM and gamma-glutamyltransferase, and these results have been used along with results from abnormalities on fetal ultrasound to provide a tentative diagnosis of congenital infection when serology or culture studies are not available. Studies using PCR detection of T. gondii DNA in amniotic fluid have shown promise with high degrees of sensitivity (up to 98%) and specificity (90%) in some research laboratories (88,109,110,111). However, the PCR testing is not standardized, not all tests are equally sensitive, and interlaboratory variability can occur. PCR test results do have the advantage of a more timely result (1 day vs. 4 weeks for culture). Use of real-time quantitative PCR assays has shown that high parasite loads in the amniotic fluid correlate with more severe outcomes.
The serologic diagnosis of congenital toxoplasmosis in the infant is also not necessarily straightforward either (77,112). At birth, toxoplasma-specific IgM antibodies can be detected in 25% of congenitally infected infants if the IFA method is used. Other testing methods are recommended for this purpose. IgM tests are positive in congenitally infected in at least 75% of infants if the DS-IgG-ELISA or the ISAGA tests are performed. Congenitally infected infants who are IgM antibody positive may remain so for up to a year after birth. There is the possibility that passively transferred maternal IgG antibodies can suppress the infant’s capability to produce IgM antibodies. This may explain why some clearly congenitally infected infants will seemingly seroconvert after birth, and specific IgM antibodies are then detected later in infancy. Maternally transmitted IgG antibody titers drop by 50% each month and, depending upon the maternal titer, it may persist for at least a year after birth. Measuring infant’s IgG titers over time is another method to determine whether an infant has congenital toxoplasmosis. If the titers do not decline as expected, congenital toxoplasmosis should be suspected. Finally, most congenitally infected infants do produce specific IgA titers, and many produce IgE-specific antibodies. These tests can be useful in unclear cases. For infants with CNS disease, determining if there has been intrathecal production of specific IgG and/or IgA antibodies may be helpful.
In summary, infants born to mothers who have been demonstrated or suspected to have had toxoplasmosis in pregnancy or within 6 months of becoming pregnant should be investigated for congenital toxoplasmosis (77,103).
Infants should have IgM tests for T. gondii-specific IgM antibodies using DS-IgG-ELISA or the ISAGA
Immediately after birth
One month after birth if the initial IgM tests are negative
Infants should have IgG T. gondii-specific antibody titers obtained
Immediately after birth.
If IgM testing is negative, IgG testing should be repeated at 6 weeks and 3 months of age to determine if the titers are declining as expected.
Consultation with the medical microbiologist in the reference laboratory conducting the testing is recommended in interpreting the results of toxoplasma serologic testing in pregnancy and in the neonatal period and to help with arranging for PCR and other testing as necessary.
Treatment and Management
Treatment of acute toxoplasmosis is not usually undertaken except in the case of pregnant women. Women who are diagnosed with toxoplasmosis in the first half of pregnancy may elect to terminate their pregnancy. Although the risk of congenital infection is lower, those who are affected tend to be more severely so.
It is recommended that women, who elect to continue their pregnancy, be treated with spiramycin as soon as possible (89,90,107,113). Spiramycin is a macrolide antibiotic that is active against T. gondii and can cross the placenta and enter the cord blood and the placenta. Side effects are primarily maternal nausea, vomiting, and diarrhea. It is rated as a class c drug in pregnancy and is licensed for use in Canada and Europe in pregnancy and available for special access in the United States. The recommended dose is 1 g three times daily, which unfortunately does not seem to reliably provide antibiotic levels in fetal serum, placental tissue, or the amniotic fluid to inhibit the parasite. Studies of its effectiveness are inconclusive. It is thought to reduce the risk of intrauterine infection to the fetus, but it does not seem to affect the course of infection once it has occurred.
If the fetus has been shown to be infected, additional therapies are suggested for maternal treatment during the pregnancy. Presently, this includes the use of pyrimethamine and sulfadiazine. Pyrimethamine is an antimalarial drug and is a folic acid antagonist. It has a long half-life and achieves high tissue concentrations, particularly in brain. It causes bone marrow suppression that can result in anemia, granulocytopenia, thrombocytopenia, and pancytopenia, which on occasion is severe. Other side effects include a bad taste in the mouth, headache, and gastrointestinal side effects. The drug is known to be teratogenic in animals and so should be avoided in the first 5 months of pregnancy. Sulfadiazine acts synergistically with pyrimethamine against T. gondii and is also a folic acid antagonist. Bone marrow suppression is also a concern with its use, and patients frequently have rashes, crystalluria, hematuria, and renal failure, which is usually reversible with discontinuation of the drug. It is unknown whether this regimen reduces the transmission of T. gondii and, because of the toxicity, is only recommended in an attempt to treat a known infected fetus prenatally. It is thought to reduce the occurrence of severe congenital infection and increase the proportion of infants born with asymptomatic toxoplasmosis. If used, the combination is provided along with leucovorin supplements alternating monthly with spiramycin.
Although there are no clinical controlled trials to guide therapy, treatment protocols have been developed for congenitally infected infants that show effectiveness when compared to historical outcomes (97,101,102,114,115). The treatment of symptomatic infants during the first 12 months of life usually involves the use of pyrimethamine, sulfadiazine, and leucovorin. The dosages usually used are as follows: pyrimethamine 2 mg/kg/d orally for two doses as an initial loading dose following by 1 mg/kg (either daily or divided bid) for the first 6 months after birth and then on alternate days for the next 6 months (months 7 to 12); sulfadiazine 100 mg/kg/d orally divided into bid dosing for 12 months; and leucovorin 10 mg IM three times per week for 12 months. Some centers modify this treatment regime after the first 6 months of therapy so that the therapy from months 7 to 12 after birth involves alternating months of spiramycin therapy of 100 mg/kg/d in divided doses with months of pyrimethamine, sulfadiazine, and leucovorin. Infants with chorioretinitis or CSF protein elevations (≥1 g/dL) also generally receive prednisone or methylprednisolone (1.0 to 1.5 mg/kg/d orally divided bid) to reduce the inflammatory response while on antitoxoplasmosis therapy. Pyrimethamine serum levels do not vary significantly by age; therefore, there is no need to adjust the dosage other than by the weight of the child, which should be done weekly. Infants need to have their CBCs monitored weekly for the first 6 months of therapy and thereafter every other week when receiving pyrimethamine. The dose of leucovorin can be increased if the absolute neutrophil count (ANC) falls below 1,000 × 106/L. The pyrimethamine should be held if the ANC falls below 500 × 106/L. For infants who develop an allergy to sulfadiazine, clindamycin at a dosage of 20 to 30 mg/kg/d can be substituted. The usual presentation of allergy to sulfadiazine is skin rash, such as hives or allergic dermatitis. However, some infants can have sulfadiazine-induced leucopenia that presents with persistent leucopenia despite increased dosing of leucovorin and discontinuation of pyrimethamine. Children with glucose-6-phosphate dehydrogenase (G6PD) deficiency should receive clindamycin in place of sulfadiazine. Treatment of children on medication for seizures may be complicated. Pyrimethamine serum concentrations and half-life is reduced for infants who are also being treated with phenobarbital. Pyrimethamine overdosage can cause seizures. Sulfadiazine may increase the half-life of phenytoin due to interference with hepatic microsomal enzymes and so dosage adjustment is necessary. Use of sulfadiazine with carbamazepine or clonazepam may exacerbate bone marrow suppression and neutropenia. Finally, sulfadiazine is excreted via the renal system, and dosage adjustment is necessary for infants with renal impairment. Renal and hepatic function should be tested at the beginning of therapy and monitored every few months while on therapy.
Infants who are determined to have congenital toxoplasmosis and who are asymptomatic at birth also should be treated. The recommended treatment involves an initial 6-week course of pyrimethamine, sulfadiazine, and leucovorin in the same doses used for symptomatic infants. They then continue with alternating courses of spiramycin for 6 weeks and pyrimethamine, sulfadiazine and leucovorin for 4 weeks to complete a 1-year course of therapy. Monitoring for drug adverse effects while on pyrimethamine is similar to that described above.
For asymptomatic infants born to mothers with documented gestational toxoplasmosis for whom the suspected diagnosis of congenital toxoplasmosis is not yet confirmed, initial treatment with pyrimethamine, sulfadiazine, and leucovorin can be started while awaiting definitive study results. If the diagnosis is confirmed, then the treatment for asymptomatic congenital toxoplasmosis can be continued.
For healthy infants born to mothers with suspected but not confirmed gestational toxoplasmosis, spiramycin can be started while awaiting the definitive test results.
All infants with congenital toxoplasmosis who survive will need close follow-up in childhood for developmental issues and lifelong for ocular disease regardless of their initial presentation.
Rubella
Rubella (German measles, third disease) is caused by the rubella virus, which is an enveloped, single positive-stranded RNA virus. There is only one antigenic type known, but there are several rubella strains, which differ in their viral properties (hemagglutination, cell tropism), virulence and teratogenicity (27). Molecular techniques allow the differentiation between rubella virus strains, which is important in tracing epidemics and in determining whether an infection is caused by the wild-type virus or is related to the RA 27/3 vaccine strain (116). Humans are the only natural host, but some animals can be experimentally infected. Postnatally, transmission of rubella occurs by airborne spread of infected respiratory secretions. Direct contact with virus-containing urine or feces is less common. Transmission of rubella from mother to child is thought to be almost exclusively transplacentally. Natural infection is said to confer lifelong immunity, but asymptomatic reinfection in adults can occur in the situation of low antibody titers. Adults with vaccine-induced immunity are more likely to have clinical reinfection than those who had natural infection, even when stratifying for equivalent low antibody titers (117). Prior to institution of universally funded immunization programs, major rubella epidemics occurred about every 5 to 10 years (118). The last major epidemic occurred in the United States between 1964 and 1965. This resulted in approximately 20,000 cases of congenital rubella. The rubella vaccine was licensed in 1969 in the United States. In 1966, rubella became a notifiable disease and so the effect of the immunization program on congenital rubella risk is well documented (119,120,121). The incidence of postnatal rubella has decreased by 99% and that of congenital rubella syndrome (CRS) by 97%. The reason that there has not been the same reduction in congenital rubella incidence is that there is a disproportionate effect on the incidence of rubella among children less than 12 years of age. Not all older individuals were immunized, and childhood immunization against rubella does not occur worldwide (122,123,124). In addition, there are communities and groups who are conscientious objectors to immunization in general or to the MMR vaccine specifically. Therefore, there remains a continued risk of exposure, and from 10% to 20% (a significant proportion) of women of childbearing age are potentially susceptible to the virus. Case reporting for CRS is a passive program in most jurisdictions, and it is thought that the majority of cases go unreported. Therefore, the incidence of CRS is an estimate, which in countries with an immunization program is thought to be around 0.4 per 100,000 live births.
The risk of transmission of rubella to the fetus if a pregnant woman develops rubella or demonstrates subclinical infection during pregnancy is related to the gestation of the pregnancy (27,125,126,127). If this occurs within the first 12 weeks of gestation, the risk is around 80%, around 55% if the infection is between 13 and 16 weeks of gestation. It falls to around 35% if between 17 and 22 weeks and 30% if between 23 and 30 weeks of gestation. It then rises to 60% between 31 and 36 weeks and then to 100% if greater than 37 weeks of gestation. The development of congenital abnormalities is also dependent on the gestational age of the fetus at the time of the infection as detailed in the following section. Women who acquire rubella in the first 5 months of pregnancy may choose to have a therapeutic termination of pregnancy.
Pathophysiology and Clinical Presentation
In postnatal transmission, the virus initially multiplies in cells of the nasopharynx followed by a period of systemic viremia and shedding from the throat during which the placenta and fetus are infected. The risk of infection to the fetus and its consequences are determined by the serostatus of the mother and the gestation of the pregnancy at the time of the transmission to the fetus. How the fetus sustains such extensive damage is not completely understood. Placental vascular endothelial cells become necrotic and may result in virus-infected emboli (128,129). Thrombosis of the small blood vessels results in hypoxic tissue damage. Rubella-infected cells have reduced mitotic potential as a result of chromosomal breaks. They produce a growth-inhibiting protein and have mitochondrial changes that may result in alterations in cell metabolism. Finally, by altering the actin filament arrangements, the cytoskeletal microtubular system is altered (130). The virus establishes a chronic nonlytic infection of the fetus that can involve any organ system (131). It can induce apoptosis, but the role of this in the teratogenicity of the virus is not established. Focal lysis of cells without associated inflammation is seen and so it is a noninflammatory process resulting in necrosis of the heart, eyes, brain, and ears. The growth restriction seen in rubella is associated with actual reduction in cell numbers (132). Ongoing damage results in late manifestations, which are thought to be viral persistence in association with ineffective immune mechanisms including rubella-specific immune complexes, defective cytotoxic effector cell function, or autoimmunity (133,134,135,136,137). Two rubella-specific proteins (E1 and E2 proteins) found on the viral envelop are thought to be responsible for autoantibody production.
The clinical presentation in postnatal infection may be subclinical seroconversion that occurs in 20% to 50% but which still represents a risk of congenital disease for the fetus (133). For those who develop disease, symptoms start between 12 and 24 days (mean 18) from exposure and begin with a prodrome of malaise. A low-grade fever may be present from 1 to 5 days before the onset of the rash and usually resolves on the first day of the rash presents. The rash is similar to that of measles in that it typically presents of the face or occipital region as a macular papular rash that moves down the body over a 1- to 2-day period. It then disappears after 3 to 5 days. It is not as erythematous as that of measles and there is not the sandpaper feel to the rash as it resolves. There may be an associated conjunctivitis as well as postauricular, suboccipital, and posterior cervical lymphadenopathy. Among adults, arthralgias are also common. Some individuals can have a complicated illness. Pregnancy does not seem to affect the presentation of disease.
Congenital rubella infection may present with a wide variety of clinical findings at birth or the infant may appear normal at delivery and signs develop over time (118,130,132,134,135,136,137,138,139,140,141,142). The initial characterization of CRS as the triad of heart defects, cataract and hearing defects in association with maternal rubella infection in the first trimester of pregnancy has expanded considerably over time. The most common abnormalities in decreasing order of frequency are: sensorineural hearing loss, mental retardation, cardiac malformations and ocular defects. The development of late-onset CRS manifestations may be related to persistence or reactivation of the viral infection, the immune response, or consequences of vascular damage. Intrauterine growth restriction is present from 50% to 85% of infants. This may be the only initial sign. Most infants also have disturbances in postnatal growth, which is more pronounced among those with other congenital defects. Heart defects are seen more commonly in infants infected in the first trimester. Patent ductus arteriosus is found in 30% of affected infants and which may be associated with other cardiac defects, most commonly pulmonary valvular or artery stenosis. Pulmonary artery stenosis is the next most common heart defect and results from intimal proliferation. Other cardiac defects in CRS include coarctation of the aorta, atrial and ventricular septal defects, tetralogy of Fallot, ventricular aneurysm, myocarditis, and aneurysms of peripheral arteries. Hearing loss is the most common specific congenital defect. It is frequently seen as part of the CRS. It is usually bilateral. It may be present at birth or it may develop over time and be progressive. It is rarely seen if the maternal infection occurred after 17 weeks of gestation. Cataract is found in 35% of infants. It may be either unilateral or bilateral and is seen at birth or shortly thereafter, as part of the routine eye examination for the red reflex. In some cases, it may resolve spontaneously; however, most will require cataract surgery. Depending upon the other manifestations and the age at which the surgery is done, improvement in visual acuity may be disappointing. In addition, retinopathy is found in 35% to 60% of infants. It also may be present at birth or be detected later in life. It is often unilateral and has a distinctive “salt and pepper” appearance. Fortunately, it alone does not appear to affect visual acuity. Some infants may present with a cloudy cornea that usually spontaneously resolves. Glaucoma occurs in less than 10% of infants. It may be bilateral and, like the other ophthalmologic abnormalities, may be either present at birth or diagnosed later. It is important to assess infants over time for this problem as it leads to blindness if not appropriately treated. Many infants with cataract will also have microphthalmia. These infants have a higher risk of glaucoma. Other eye abnormalities that have been observed include iris hypoplasia, strabismus, and iridocyclitis. Approximately 5% in infants will develop an interstitial pneumonia which is thought to be immune mediated and which may be acute, subacute, or chronic. Approximately 20% of infants will have a transient meningoencephalitis, which may manifest with bulging anterior fontanelle, hypotonia, irritability, and seizures. CSF findings show a mononuclear pleocytosis, increased protein content, and rubella virus isolation in 30%. However, in approximately 35%, EEG abnormalities are detectable during the first year of life. Rarely, a progressive rubella panencephalitis can occur. This is a chronic infection that becomes symptomatic in the early teenage years. Some infants will present with microcephaly and/or intracranial calcifications and/or a large anterior fontanelle. Most infants will have neurodevelopmental issues. These range from developmental delay, speech defects in association with hearing loss, and behavior difficulties that may be associated with undiagnosed hearing loss. In approximately 5%, blueberry muffin spots may be transiently seen and some children will have chronic rashes from which rubella virus can be isolated. There are a number of dermatoglyphic abnormalities that serve as a marker for viral teratogenicity. There are also a number of genitourinary malformations that have been seen in CRS. These include cryptorchidism, testicular agenesis, scrotal calcifications, hypospadias, hydroureter, hydronephrosis, ureteral duplication, polycystic kidneys, renal agenesis, and renal artery stenosis with hypertension. Radiolucencies in the distal femur and/or the proximal tibia are found in radiographs in 10% to 20%. These resolve by approximately 3 months of age and are thought to be due to the direct inhibitory effect of rubella virus on bone and cartilage cells. More than 50% of symptomatic infants will have hepatosplenomegaly at birth that resolves over several weeks. Hepatitis may also occur in 5% to 10% which may, or may not, be associated with jaundice. Obstructive jaundice occurs in about 5% of infants. Some infants may have pancreatitis or intra-abdominal calcifications. There may be structural abnormalities of gastrointestinal tract that include esophageal, jejunal or rectal atresia, and some children will have chronic diarrhea. In infants with severe disease, thrombocytopenic purpura occurs at birth from 5% to 10%. Some children will have a transient anemia that may be hemolytic in nature. Rubella virus can infect fetal pancreatic islet cells resulting in the reduction of insulin secretion. Approximately 20% of children with CRS will develop insulin-dependent diabetes by 35 years of age (143,144). The majority of these individuals have circulating pancreatic islet cell cytotoxic or surface antibodies apparently triggered by the rubella virus. Other rare diseases include hypo or dysgammaglobulinemia, thymic hypoplasia, hypothyroidism, hyperthyroidism, thyroiditis, growth hormone deficiency, and precocious puberty.
Diagnosis
The diagnosis of post-natal-acquired rubella in a pregnant woman based on the clinical presentation was never assumed to be accurate and is even less so now after 45 years of immunization programs (145). Diagnosis is based on the results of laboratory serology or viral testing. Rubella-specific antibodies are produced by all classes of immune globulins (IgG, IgM, IgA, IgE, and IgD) following postnatal infection (146). All classes of specific antibodies are found early in the illness. In general, only specific IgG antibodies persist for life. IgM antibodies are detected shortly after infection and usually persist for 1 to 2 months afterward (147). Therefore, the presence of rubella-specific IgM antibodies in a sample collected within 1 month of a rash illness in a pregnant woman should be diagnostic of rubella infection. Approximately 50% will have rubella-specific IgM antibodies present on the day the rash presents, which rises to 90% by day 5 of illness. However, these antibodies have been reported to persist for years in some people. Also, the IgM response to rubella can be detected with other viral acute infections, specifically Parvovirus B19, CMV, and EBV and occasionally upon reexposure of an individual previously immune. Finally, IgM antibodies have been reported as persisting for several months following immunization, which may complicate the diagnosis of maternal infection in a second pregnancy in which the mother was immunized after the first if there is a short interval of time between them. A second method of determination of rubella infection in a pregnant woman by serology involves testing specific IgG antibody responses (148,149). IgG antibodies can be detected using a variety of methods including hemagglutination inhibition, ELISA, immunofluorescence, radioimmunoassay, hemolysis in gel, complement fixation, passive hemagglutination, and latex agglutination testing. Serum specimens taken as soon as possible after the rash has appeared or a suspected exposure has occurred and one taken 2 to 4 weeks later can be run in parallel to determine the appearance of specific IgG antibodies or a significant rise in rubella-specific titers (usually fourfold or greater). The serologic testing methods differ in the times following infection in their ability to detect antibodies. This may be useful in determining the timing of infection in complex cases. If ELISA, hemagglutination inhibition, or radioimmune assays are used, rubella-specific IgG can be detected as early as 2 days before the onset of the rash. Antibodies are not usually detected by passive hemagglutination until 15 to 50 days after rash onset, and these antibodies peak in titers at 6 to 7 months postillness. IgG avidity testing is now used to help determine whether a pregnant woman has recently become infected. IgG avidity is low in the first few months after infection or immunization but then rises and stays high thereafter (150). So, in confusing situations, a past history of immunization and recent history of exposure, the rubella IgG avidity testing can be used to determine if the IgG antibodies of the pregnant women represent a recent or past response. Interestingly, women produce IgG antibody directed against the E2 envelop protein which men do not and have higher levels of antibody production (151). Finally, viral detection using RNA PCR techniques can be done from maternal nasopharyngeal swabs, and the virus is reliably detected from these specimens up to 7 days after the appearance of the rash (152).
The diagnosis of congenital rubella involves both serologic testing and virus detection (153). The fetus is capable of developing IgM antibodies by 16 weeks of gestation. Prenatal diagnosis of congenital infection can be attempted by sampling fetal cord blood for the presence of rubella-specific IgM. This may be technically complex, and the sensitivity is low. Testing for IgM rubella-specific antibodies after birth is the more common method of serologic diagnosis. However, up to 20% of congenitally infected infants my test negative for rubella IgM antibodies at birth and a repeat test at around 28 days is needed for diagnosis (133,149). Rubella-specific antibodies will persist for 6 to 12 months after birth and so congenital rubella can be diagnosed in older infants by testing for their presence. Specific rubella IgG antibodies are also produced. The diagnosis of congenital rubella infection can be made in an infant with persistence of rubella-specific IgG antibodies in high titers beyond 6 to 12 months of age in the absence of circulating rubella in the community. Interestingly, rubella-specific IgG antibodies may not persist beyond 5 years of age in up to 20%. IgG antibodies produced by congenitally infected infants have lower affinity to rubella antigens compared to immunized adults. Also, older congenitally infected infants have higher levels of IgG antibodies directed to the E2 protein than against E1. Congenitally infected infants have diminished cellmediated immune responses to rubella compared to children and adults who acquired the infection postnatally, and infants infected earlier in gestation have lower responses than those infected later in pregnancy. These types of tests can be done in some settings if an investigation for congenital rubella is being done in an older infant or child. Rubella can be cultured from amniotic fluid, and the fluid and samples of the chorionic villus can be examined by electron microscopy for the presence of virus. However, the sensitivity of these tests is low, and PCR is the preferred method for determination of virus presence. Rubella can be detected by RNA PCR in fetal and placental tissues, amniotic fluid, chorionic villus samples, and fetal blood (152,154,155). These tests should be done between 6 and 8 weeks after the maternal infection to minimize the chance of a false-negative or a false-positive result.
The diagnosis of CRS is based on a combination of laboratory and clinical findings (153). Infants require a complete cardiac and neurologic evaluation, which should include an echocardiogram, neurologic imaging, and both an ophthalmologic and audiologic assessment. Infants should have a CBC, hepatic function tests, and radiographs of the long bones. Some recommend examination of the CSF. Infants with clinical abnormal findings consistent with rubella from whom the virus has been detected by PCR or has been isolated and/or has a positive rubella-specific IgM titer and/or has persistence of rubella-specific IgG antibody titers are considered to have confirmed CRS. Infants who do not have any congenital defects but who have laboratory evidence of congenital infection are considered to have congenital rubella infection. Infants with two or more of the eye, cardiac, or hearing clinical manifestations consistent with CRS with or without other commonly described abnormalities but without complete laboratory confirmation would be classified as having a CRS compatible condition.
Treatment and Management
There is no specific antiviral treatment of rubella. Management of infected individuals is supportive, usually involving multiple medical specialties. CRS patients frequently require corrective surgery. Children diagnosed with CRS or congenital rubella infection or CRS compatible disease should be monitored for the development of late-onset disease manifestations.
Prevention of infection via immunization programs to ensure that the incidence of rubella is low and that pregnant women are not susceptible to rubella is the hallmark of the strategy to combat congenital rubella (118,156,157). The most common vaccine strain used is RA 27/3 attenuated live rubella virus vaccine which is most commonly given in combination with vaccines for measles and mumps (MMR) or newer vaccines that also contain varicella (MMR-V). It produces an antibody response in more than 95% of individuals 12 months of age and older and is 90% effective at preventing disease for at least 15 years after immunization. It is safe to immunize a child or household contact with rubella vaccine if the pregnant mother is susceptible. A booster vaccine is usually given from 3 months to 4 years after the initial immunization as part of the routine childhood immunization schedule in jurisdictions where there is a rubella immunization program. Pregnant women whose rubella immune status has not been established should be screened at the first prenatal visit. Women found to be susceptible should be counseled regarding the risk of rubella and to seek care should they come into contact with another individual suspected or diagnosed with rubella or if they develop a febrile rash illness that is consistent with rubella.
Pregnant women who were seronegative should have rubella immunization immediately in the postpartum period. Immunization during pregnancy is to be avoided. Programs that provide this immunization prior to discharge from hospital are more successful than those that require immunization to be provided at a postpartum clinical visit. Some women may develop postimmunization arthritis or arthralgias in the postpartum period, particularly those with certain human leukocyte antigen class II (HLA-DR) phenotypes, in particular those with DR4 and either DR1 or DR2 (158). The rubella virus may be shed in breast milk and infect the neonate, but this is not a contraindication to postpartum maternal immunization.
Immunization during pregnancy is not advised. Over 700 women have been followed after inadvertently having been immunized either immediately before pregnancy or in the first 12 weeks of pregnancy (159). The vaccine virus was demonstrated to cross the placental barrier in a few cases, but the observed rate of CRS has been zero. In one case though, the infant excreted the vaccine virus for several months. Susceptible pregnant women should avoid contact with children with CRS or congenital rubella infection for the first year of the infant’s life. Infants suspected to have or to have been proven to have congenital rubella should be placed on contact precautions for the first year of life unless they have been shown to have negative rubella cultures on two occasions taken 3 months apart (157).
Syphilis
It was once stated that “to know syphilis is to know medicine” because of the wide range of clinical presentations due to this bacteria. Treponema pallidum (TP) is the causative agent of syphilis (160). It is a gram-negative spirochete that only naturally infects humans but can cause disease in other primates, pigs and rabbits in the laboratory setting. It does not grow on conventional media. There is no animal model for the study of pathogenesis of congenital syphilis. It is universally susceptible to penicillin, third-generation cephalosporins, and macrolide antibiotics. Syphilis is a sexually transmitted disease among adults, and congenital syphilis results primarily from transplacental transmission from an infected mother to her infant. The prevalence of syphilis among adult childbearing populations varies considerably. Worldwide, maternal syphilis is suspected to complicate 1 million pregnancies (161). The risk of congenital syphilis is dependent upon the prevalence of syphilis in the local adult populations, the stage of maternal disease, maternal coinfection with HIV and, to a great extent, the effectiveness of maternal prenatal screening and treatment programs (162). Syphilis can be transmitted throughout gestation, but the risk of transmission increases as gestation progresses (163). Transmission occurs between 60% and 100% of pregnancies when mothers have primary or early secondary syphilis. Mothers in the latent and latelatent stages transmit in 40% to 8% of pregnancies, respectively. In the past decade, the rate of congenital syphilis in the United States has varied from 8 to 10 cases per 100,000 live births.
Pathophysiology and Clinical Presentation
Once the spirochete crosses the placental barrier, it widely disseminates throughout the fetus (164). The manifestations of congenital syphilis are a result of the host responses to T. pallidum (165,166,167). Regardless of the organ system involved, the pathologic appearance of infected tissue shows perivascular infiltration by lymphocytes, plasma cells, and histiocytes-producing obliterative endarteritis and extensive fibrosis. Placentas in which the pregnancy is complicated by syphilis tend to be relatively large with focal villitis and, in those infants who are symptomatic at birth, a necrotizing funisitis (168). A few infected live born infants may have clear manifestations of illness at birth, usually presenting with vesicular or bullous skin lesions and/or hepatosplenomegaly. Most infants though are asymptomatic in the early neonatal period. Approximately 60% of affected infants will develop some clinical manifestation of congenital syphilis by 3 months of life. The development of “snuffles,” a thick purulent nasal discharge that is highly infectious and teeming with spirochetes, along with palmar and plantar bullae (also highly infectious) and splenomegaly is a highly suggestive clinical presentation of congenital syphilis and usually is seen beginning around week 3 of life. Osteochondritis and periostitis may be seen in the long bones or in the ribs. This may be present at birth in an otherwise asymptomatic infant. In some instances, this may result in fracture, and the infant will decline to move the affected limb (pseudoparalysis of Parrot). Other signs are less specific and include fever, lymphadenopathy, pneumonitis, irritability, meningitis, hepatosplenomegaly, hepatitis, jaundice, pancreatitis, glomerulonephritis or nephrotic syndrome, hemolytic anemia, disseminated intravascular coagulation (DIC), thrombocytopenia, and failure to thrive. Pneumonia due to syphilis classically shows complete opacification of both lung fields if not treated (pneumonia alba). The hemolytic anemia may be associated with cryoglobulinemia, immune complex formation, and macroglobulinemia and be refractory to treatment and last for months. The hepatosplenomegaly is caused by extramedullary hematopoiesis and inflammation. The associated jaundice is caused by hemolysis and/or hepatitis. The hepatitis associated with syphilis usually has high alkaline phosphatase, transaminases, and γ-glutamyl transferase concentrations that worsen transiently but significantly with penicillin treatment. Some children may have fulminant sepsis like presentations with hypoglycemia, lactic acidosis, encephalopathy, and DIC in association with hepatic failure. Hepatic abnormalities may persist for up to a year after treatment. Premature infants are more likely to develop severe early disease than are term infants. However, signs may not develop until puberty in some infected children. These late signs include alterations of the permanent teeth (Hutchinson teeth—peg-shaped and notched upper central incisors; mulberry molars—multicuspid first molars), interstitial keratitis, secondary glaucoma, eighth nerve deafness, saddle nose deformity due to scarring by syphilitic rhinitis, cranial nerve palsies, developmental delay, hydrocephalus, epilepsy, optic nerve atrophy, frontal bossing, saber shins (anterior bowing of the mid tibia), and Clutton joints (synovial effusions of the knees).
Diagnosis
T. pallidum can be detected with immunohistochemical stains or PCR performed directly from the placental tissue. However, diagnosis is made via diagnostic laboratory testing, and management decisions are based on maternal treatment history and the infant’s initial evaluations.
An infant has congenital syphilis if he or she has physical, laboratory, or radiographic signs of syphilis (confirmed/highly probably congenital syphilis) or the child was born to a mother with untreated, inadequately treated or suboptimally treated syphilis (presumed congenital syphilis) (169). Laboratory diagnosis requires demonstration of T. pallidum by PCR, dark field microscopy, fluorescent antibody stains, or other specific stains in infant or placental tissues (170). Alternatively, if antibody testing of the infant’s serum (not cord blood) shows a fourfold higher titer than a simultaneously tested maternal sample by either Rapid Plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) measurements, then the diagnosis is thought to be likely correct. The RPR may not be reactive if the mother had recently acquired the disease. IgM antibody testing is often unreliable given the high levels of both false-positive and false-negative test results.
In addition to serologic testing, infants who are suspected as having congenital syphilis need to be assessed with long bone radiographs, CSF examination, CBC, and liver enzyme determinations. The criteria used to diagnose congenital neurosyphilis include CSF mononuclear pleocytosis (≥25 cells/mm3), elevated protein concentration (>150 mg/dL in term infants and >170 mg/dL in premature infants), and a reactive CSF VDRL (171,172). These tests are actually neither sensitive nor specific. The elevated CSF WBC has a sensitivity of 38% and a specificity of 88%. The elevated CSF protein has a sensitivity of 56% and a specificity of 78%. The CSF VDRL has a sensitivity of 54% and a specificity of 90%. If available, the most sensitive and specific test is examination of the CSF by PCR testing.
Screening serologic testing for syphilis traditionally used RPR and VDRL as the initial test, and the diagnosis of positive syphilis serology was then confirmed using specific treponemal antigen testing (the most usual one used being the TP passive particle agglutination assay—TPPA). However, this sequence of laboratory tests has changed in many laboratories in recent years for screening for syphilis. The development of more automated treponemal-specific testing has led to their use first followed by using the RPR and VDRL for confirmation. The sensitivity and specificity of these new tests, which are the TP-ELISA test and the TP-CMIA (TP-specific chemiluminescent immunoassay), are both reported to be 100% and 95%, respectively (173). The VDRL and RPR tests are still used to evaluate response to therapy and are the tests that should be used to determine whether the infant requires investigation and treatment for congenital syphilis and for follow-up monitoring the infant’s status.
Management and Treatment
Management and treatment algorithms are based on a combination of the results of investigations of syphilis of the mother, treatment she has received, syphilis testing of the infant, and results of hematologic, CSF studies, hepatic function studies, and radiologic evaluation of the infant (174). All infants born to mothers with reactive RPR/VDRL and positive specific treponemal antibody tests should have a complete physical examination and a VDRL or RPR test to compare titers with that of the mother. All infants should have follow-up titers done until either they are negative or they have reached a serofast state. Not all children need to be treated for congenital syphilis, and the management plans are based on the results of testing and treatment records of the mother and the physical examination of the infant.
No treatment is needed for the infant only in the situation where the mother has received adequate treatment with penicillin before pregnancy with a demonstrated low stable titer (serofast) of VDRL ≤1:2 or RPR ≤1:4, and the infant’s physical examination is normal.
Infant given benzathine penicillin G, 50,000 U/kg IM as a single dose.
The mother has received adequate treatment with penicillin before pregnancy with a demonstrated low stable titer (serofast) of VDRL ≤1:2 or RPR ≤1:4, and the infant’s physical examination is normal, but there are concerns that the infant will not return for follow-up.
The mother has received adequate treatment with penicillin during pregnancy more than 4 weeks prior to delivery and demonstrated a reduction of the VDRL or RPR ≤1:4; the infant’s VDRL or RPR is the same or less than fourfold higher than the maternal titer, and the infant’s physical examination is normal.
Infant to receive treatment for congenital syphilis which is aqueous penicillin G, 50,000 U/kg IV every 12 hours × 7 days if 1 week of age or younger and every 8 hours if older than 7 days. Alternatively, procaine penicillin G 50,000 U/kg IM daily × 10 days. Note if 1 day of therapy is missed, the entire course should be restarted.
Mother has received adequate treatment with penicillin during pregnancy more than 4 weeks prior to delivery, but the infant’s VDRL or RPR is fourfold or more higher than the maternal titer or the infant’s physical examination is abnormal.
Mother received adequate treatment but within 4 weeks of delivery.
Mother did not receive treatment.
Maternal treatment was not documented.
Maternal treatment course involved a nonpenicillin drug was used.
There is maternal evidence or relapse or reinfection with similar or increase in maternal VDRL/RPR.
Routine IPC precautions can be used for otherwise healthy infants with proven or suspected congenital syphilis. However, those with skin or mucus membrane lesions should be placed on contact precautions until 24 hours after the initial dose of antibiotics has been given (174). In many countries, congenital syphilis is a reportable disease, and public health officials will conduct contact tracing to identify and treat other infected individuals.
Borrelia burgdorferi (Lyme Disease)
Borrelia burgdorferi is another spirochete but one that is transmitted to humans in North America through the bite of the ticks (Ixodes scapularis [dammini] and Ixodes pacificus) (175). There are two other species of Borrelia that may cause Lyme disease in Europe and Asia (Borrelia afzelii and Borrelia garinii), but B. burgdorferi will be the primary Borrelia species discussed as the illnesses produced are generally similar. There has been considerable controversy concerning Lyme disease over the past decade including the risk to the infant when acute infection occurs during pregnancy. As well, the more widespread finding of infected ticks has increased over the past decades, and the area in North America where endemic transmission occurs continues to expand. In addition, infections with the other illnesses transmitted by these ticks (babesiosis and human granulocytic anaplasmosis) have also been increasingly described in new regions. On occasion, mixed infections can occur. All these tick borne illnesses can affect pregnant women.
Pathophysiology and Clinical Presentation
The clinical presentation of untreated Lyme disease after the neonatal period involves three general stages (175). The first stage occurs within 7 to 28 days of the tick bite and involves the development of a characteristic rash, erythema migrans (EM), at the tick bite site. This occurs in approximately 80% of infected patients. The second stage involves early dissemination of the spirochete and is manifested by multiple EM lesions along with neurologic and/or cardiac findings. The neurologic findings may include meningitis, unilateral or bilateral facial nerve palsies, and peripheral motor and/or sensory neuropathies. The cardiac findings usually involve first-degree atrioventricular block. During the first and second stages, the spirochete can be recovered from the blood in up to 50% of cases. Late Lyme disease may develop months to years after the initial infection and is characterized by intermittent or persistent arthritis usually involving one or more large joints, specifically the knee, along with subtle cognitive disturbances, which may indicate encephalopathy, or polyneuropathy involving spinal radicular pain or distal paresthesias. B. garinii may be responsible for a more severe form of chronic encephalomyelitis. Some patients demonstrate a prolonged post-Lyme disease syndrome that can be debilitating and for which the cause and treatment has not yet clearly been determined. Re-infections can occur with subsequent bites by infected ticks among individuals who have been appropriately treated during previous primary or secondary stages of illness.
Since Borrelia are spirochetes and a blood borne phase with dissemination clearly occurs, there is concern of transplacental transmission to the fetus during those times. At present, there has not been a congenital Lyme disease syndrome identified. Specifically, studies done in highly endemic areas involving more than 3,700 pregnancies have not shown an association with maternal-positive Lyme serology and/or history of tick bite in pregnancy with adverse pregnancy outcomes including fetal malformations (176,177,178,179). However, the spirochete can be transmitted to the fetus when the mother is not treated, and there is one case report in which this occurred despite penicillin therapy in the first trimester (180,181). Postnatally, there is no evidence of mother-to-child transmission through breast milk or close contact.
Diagnosis
Diagnosis of the first stage of Lyme disease in pregnant women is made clinically based on the presence of EM and a history or either tick bite or residence in/travel to a known endemic area within the preceding weeks (175). Diagnosis of later stages of illness is also based on clinical suspicion and history of likely exposure. Serologic testing is recommended for symptomatic pregnant women with a history of likely exposure. In some localities, testing for human granulocytic anaplasmosis and/or babesiosis should also be considered. Screening for Lyme disease in pregnancy of asymptomatic women without a recent history of exposure is not recommended. Serologic testing is usually done by a two-step procedure by diagnostic laboratories in that a positive ELISA or immunofluorescent assay is confirmed by an IgG and IgM Western blot. A newer ELISA test (VisE C6 peptide ELISA) is being evaluated as a single step test. There may be variation in the sensitivity and specificity of tests between laboratories, but this is usually minimal. Individuals who are suspected to be infected with strains other than B. burgdorferi should be tested with the VisE ELISA. Individuals in the early stage of the disease may have a negative serologic test. Individuals who have been treated early in their illness may not develop antibodies. Individuals who have had symptoms more than 2 months may have negative IgM antibodies but will be seropositive with the IgG Western blot. Positive IgG antibodies will decline over time with and without treatment but remain detectable for several years. The rate of decline of antibodies is not useful as an indication of effectiveness of treatment.
Despite the low probable risk of infection, infants born to pregnant women who had the diagnosis of a primary or second stage of infection during pregnancy will likely need to be assessed for Lyme disease even if the mother received treatment. In asymptomatic infants, this can be done by obtaining serial serologic tests for Lyme disease to document decline and disappearance of maternal transplacental antibodies. These may persist for several months, and the parents will need to be appropriately counseled. PCR testing is possible and in the situation in which the infant is unwell and Lyme disease is clinically suspected, consultation with the microbiologist at the laboratory coordinating the diagnostic testing is recommended to facilitate testing and to ensure that it is appropriately done in an accredited laboratory.
Treatment and Management
The treatment of pregnant women found to have clinical Lyme disease depends upon the stage of the disease and whether neurologic involvement is present (175). For primary illness involving EM, oral amoxicillin 500 mg three times daily for 14 to 21 days or cefuroxime axetil 500 mg twice daily for the same time period if allergic to amoxicillin. For those with neurologic symptoms, either intravenous ceftriaxone (2 g daily) or cefotaxime (2 g three times a day) for 14 to 28 days is recommended. Pregnant women whose only neurologic manifestation is facial nerve palsy could be treated with oral amoxicillin. Arthritis is treated with either oral or intravenous antibiotics for 30 to 60 days. Women who are found to be seropositive for Lyme disease in pregnancy and are asymptomatic do not require treatment. Women who have had a recent tick bite do not require antibiotic prophylaxis.
There are no management or treatment guidelines for the infant found to be infected with B. burgdorferi. Consultation with a specialist in pediatric infectious diseases would be recommended.
Pregnant women should be counseled regarding prevention of tick bites by avoiding tick-infested areas or, if this is not possible, reducing the risk of contact by using protective clothing, insect repellants (DEET containing repellants are considered to be safe in pregnancy), and by daily complete examination of the body for ticks and rapid removal of any found to be attached.
Varicella Zoster
The varicella-zoster virus (VZV) causes the primary infection varicella (chickenpox) and a distinctive illness associated with reactivation— herpes zoster (shingles) (182,183,184). It is an enveloped double-stranded DNA virus in the herpes family. There is only one serotype, but there are a few distinct strains. It is a highly infectious virus. Prior to 1995, it was estimated that 95% of pregnant women were immune to varicella. The epidemiology has changed with the introduction of the varicella vaccine for children. The incidence of disease among children has dropped dramatically in jurisdictions that have universal childhood immunization programs that include varicella vaccine (185,186). Therefore, the risk of exposure to varicella is low. However, immunization coverage has not been universally high and vaccine-induced immunity following a single childhood immunization has been shown to wane somewhat over time. Although there is now a booster dose program in place in most jurisdictions, there may currently be a lower percentage of immune women in the childbearing ages than there was previously. In addition, women from tropical countries have not likely been immunized nor have they likely been exposed to the virus. Therefore, varicella remains of concern (187). The incubation period ranges from 10 to 21 days after exposure with the majority of individuals developing illness between 14 and 16 days after exposure. Individuals are most infectious on the day immediately before and the day the rash develops. Transmission occurs from exposure to infected respiratory secretions, which may be airborne. Individuals with zoster can transmit the virus to susceptible individuals who have direct contact with the zoster lesions. Immune-suppressed individuals can develop disseminated zoster and transmit the virus through infected respiratory tract secretions in the same manner as individuals with primary varicella. The estimated incidence of gestational varicella infection prior to the institution of routine varicella immunization in children in the Unites States was 1 to 7 per 10,000 pregnancies (188). The actual incidence of zoster in pregnancy is unknown but is estimated to be 0.5 per 10,000 pregnancies. Congenital varicella syndrome is rare. The risk of congenital varicella syndrome is estimated to be less than 0.5% of maternal infections occurring before 12 weeks of gestation, 2% if the mother acquired varicella between 13 and 20 weeks of gestation, and 1% if she acquired it after that period (189,190). However, approximately 25% of newborns whose mothers contracted varicella in the last 3 weeks of gestation will have clinical infection. The risk of congenital varicella syndrome or clinical infection if the mother developed zoster during pregnancy is unknown but is suspected to be negligible.
Pathophysiology and Clinical Presentation
In postnatal transmission, VZV is transmitted from infectious secretions through either the conjunctiva or nasal/oral mucosa (184,187,191). Primary infection of the respiratory tract is followed by viral replication in the regional lymph nodes and tonsils for 4 to 6 days and is then spread systemically to other internal organs. There is then a secondary viremia, which is associated with cutaneous involvement and the development of the characteristic rash. In pregnancy, infection of the fetus occurs during either the first or second viremic stage. The sites of infection in the fetus are not clear. Fetal chickenpox is thought to occur based on the findings of cutaneous scars. After resolution, there is subsequent infection of the dorsal root ganglia, which may result in cell destruction of the nerve tissue.
Very few postnatal varicella infections are subclinical; however, infections in young children less than a year of age may be missed as they tend to have very few lesions. Typically in the postnatal period, the illness consists of fever, malaise, and a distinctive pruritic rash (191). There may be a prodromal period of fever, malaise, and/or myalgia 1 to 4 days before the development of the rash. The rash usually starts of the face and trunk and moves outward to the extremities. It is characterized by successive crops of macules that develop into papules and then into vesicles. The initial vesicles are classically described as “teardrops on a red base.” Over the next 24 hours, they gradually crust over. The rash characteristically shows a combination of vesicles, papules, and crusted lesions of different sizes seen at the same time. New lesions appear daily over 3 to 5 days. Once the lesions are crusted over and no new lesions have appeared over a 24- to 48-hour period, the individual is no longer considered to be infectious. Morbidity and mortality increases with age. Although adults account for only about 2% of clinical varicella cases, 25% of the mortality due to varicella occurs in this age group. Complications include the development of varicella pneumonia which is described more frequently among pregnant women, encephalitis, bleeding diathesis, and secondary bacterial skin infections, particularly necrotizing fasciitis due to GAS.
Zoster tends to initially present with nerve root pain along a dermatome followed within days to weeks by the appearance of a papular/vesicular rash. It is usually unilateral and involves one or two adjacent dermatomes. Rash extending beyond two dermatomes implies a disseminated VZV reactivation.
VZV transmission occurs to the fetus via the transplacental route. There is some in vitro evidence that it may result in chromosomal breaks in the fetal cells, in particularly fetal leukocytes (192). There is also suspicion that there is an increase in the incidence of leukemia among infants exposed to varicella in gestation; however, the numbers involved are too small to confirm the association (193).
The congenital abnormalities associated with gestational varicella are primarily cutaneous, musculoskeletal, neurologic, and ocular (183,189,190). The most common skin abnormalities are cicatricial lesions. Limb abnormalities include hypoplasia, atrophy, and/or paresis. Limb hypoplasia is usually unilateral involving the leg. However, involvement of the arm, mandible, or hemithorax has been described. Rudimentary digits can be seen. The pathophysiology of the limb abnormalities is thought to be as a consequence of a neuropathy resulting from damage to the dorsal ganglia and anterior columns of the spinal cord. Cutaneous scars are found on hypoplastic limbs, the trunk, or the opposite extremity (see Fig. 44.4). CNS findings more commonly include microcephaly, cortical and cerebral atrophy, psychomotor retardation, seizures, and foal brain calcifications. Other findings that have been observed include low birth weight, autonomic dysfunction manifesting as loss of bowel and urinary sphincter control, dysphagia, intestinal obstruction, and Horner syndrome. Unilateral or bilateral ocular abnormalities are also common. These include optic nerve atrophy, cataracts, chorioretinitis, microphthalmos, and/or nystagmus. The mortality rate during the first few months of life among infants with congenital varicella syndrome is reported to be 30%. Among the survivors, 15% will develop zoster sometime in the first 4 years of life.
FIGURE 44.4 Limb atrophy and cicatricial skin scarring in an infant with congenital varicella syndrome. From Knipe DM, Howley PM, eds. Fields virology, 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2013.
Diagnosis
In the postnatal patient, varicella and zoster are generally diagnosed by the clinical appearance of the rash (187). Laboratory confirmation is not frequently needed. Testing that should be done when the diagnosis is in doubt include serologic tests for varicellaspecific IgG and IgM antibodies and/or isolation by viral culture or detection of VZV-specific antigen by immunofluorescence staining of cell scrapings or detection of the virus in the lesions by PCR testing. IgM varicella-specific antibodies can be detected for several months after the acute infection and may be found at the time of clinical zoster. There have been a number of varicella-specific IgG tests developed, but what is routinely used now in most laboratories is the ELISA test, which has a high level of sensitivity and specificity. Two samples collected a week apart can be used to demonstrate increasing IgG titers. If the first sample is collected late in the course of the illness, a single high IgG antivaricella titer is considered the diagnosis of recent infection in association with a compatible clinical picture.
Prenatal diagnosis of congenital varicella syndrome is made by a combination of results of ultrasonography looking for congenital abnormalities and detection of VZV DNA by PCR from fetal blood or amniotic fluid (194). The VZV PCR can be done between 17 and 21 weeks of gestation and is very sensitive to detect infection. A detailed anatomic ultrasound investigation should be done at a minimum of 5 weeks after the maternal infection to detect any abnormalities. A negative VZV PCR and a normal result of the ultrasound examination indicate that congenital VZV infection or congenital varicella syndrome is unlikely. A positive DNA PCR indicates that there is a risk of disease, and the fetal ultrasound should be repeated between 22 and 24 weeks of gestation. If the second ultrasound is normal, then the risk of congenital varicella syndrome is remote.
Postnatal diagnosis of congenital varicella syndrome depends on the history of maternal disease in the first or second trimester, the presence of compatible congenital abnormalities, and evidence of infant infection. Infant infection is confirmed by detection of VZV DNA from blood taken or the presence of VZV-specific IgM antibodies in the infant’s blood obtained shortly after birth or the persistence of VZV-specific IgG beyond 7 months of age. The development of zoster during infancy is only seen in congenitally infected infants and so would be diagnostic.
Treatment and Management
Treatment considerations of varicella have evolved over the past 10 years (182,195). Children receiving treatment with oral acyclovir will have a shortened course of illness and period of infectivity. Pregnant women with varicella pneumonia or other varicellarelated complications need admission to hospital and treatment with IV acyclovir (10 mg/kg every 8 hours). There have not been any controlled studies addressing the treatment of uncomplicated varicella in pregnancy. The American Academy of Pediatrics does not recommend treatment with acyclovir in this situation citing safety concerns. However, acyclovir has been used frequently to treat varicella, zoster, and herpes simplex infections in pregnancy without significant adverse effects. Therefore, many experts would recommend the treatment of any pregnant women with uncomplicated varicella with oral acyclovir (20 mg/kg four times daily for 5 days). Whether treatment would reduce the risk or the severity of congenital varicella syndrome is unknown.
At this time, there are no recommendations for routine serologic screening of pregnant women. Many obstetricians obtain a verbal history of exposure and do serologic testing of those who are unsure of their status. Varicella vaccine should not be given in pregnancy, but it can be safely used in the postpartum period. Mothers who do not know whether they have had varicella or varicella vaccine should be tested for IgG antibodies to VZV if a known or suspected exposure has occurred. The majority will likely be found to be immune. Those found to be nonimmune and who have a known exposure to VZV can be provided with varicella immune globulin if the exposure was within 10 days. The current formulation in the United States and Canada is VariZIG, and the adult dose is 625 units, given IM. If VariZIG or a similar product is not available, IVIG at a dose of 400 mg/kg has been used. Whether the use of either of these products will prevent congenital varicella syndrome is unknown.
There are no antiviral treatment recommendations for children born with congenital varicella syndrome.
Parvovirus B19
Human Parvovirus B19 is a small, nonenveloped, single-stranded DNA virus that does not grow on conventional cell lines but can be propagated in erythroid progenitor cells (196). There are many different genotypes, but only B19 is the antigen type currently recognized to cause disease in humans (197). It is spread primarily from respiratory secretions. The incubation period is usually between 4 and 14 days but has been described to extend to 21 days. Infections are more common in the winter months, and there are epidemics every 4 to 5 years. Serologic surveys of Parvovirus B19 immunity among pregnant women vary from 30% to 80% depending upon the country surveyed, the socioeconomic status of the mothers, the number of siblings the mother had, and the mother’s exposure to children (198,199,200). From 1% to 7% of seronegative women are estimated to seroconvert during pregnancy. Higher rates occur during winter months in an epidemic year. Rates are higher for women whose professions put them in contact with large numbers of children, that is, day care providers and teachers. Although transmission of the infection to the infant is suspected to be between 20% and 50%, fortunately, the actual risk of to the fetus of disease from maternal infection is relatively low with a less than 10% risk of adverse pregnancy outcome (201). In the case of twins, discordant disease states can occur with one infant being severely affected and the other being essentially normal. The primary outcome is fetal loss if the infection occurs in the first 20 to 22 weeks of gestation. The estimated risk of hydrops fetalis when a mother acquires Parvovirus B19 in pregnancy is around 2% (95% CI:1.2% to 5.9%).
Pathophysiology and Clinical Presentation
It is the causative agent for fifth disease or erythema infectiosum, a syndrome usually seen in children associated with a characteristic immune-mediated “slapped cheek” rash (196,197). The rash is lacy or reticulated, spreads to the trunk and extremities, and may last up to 2 weeks. It also may reappear with exposure to sunlight, temperature changes, or emotional stress. There may also be a number of other rash presentations associated including erythema multiforme. Some adults will have an influenza-like illness, and there is also frequently an associated immune-mediated symmetrical arthritis usually involving the hands but may also involve the wrists, ankles, and knees. However, half of infected adults have a subclinical presentation. It is associated with aplastic crisis in sickle-cell anemia and other hemolytic diseases and, importantly for neonatology, hydrops fetalis. It produces a lytic infection in human erythroid progenitor cells due to tropism for erythrocyte P antigen (globoside). Individuals who are “p” phenotype are naturally resistant to Parvovirus B19 infection (estimated to be 1 per 200,000) (196,202). Globoside is also found on megakaryocytes, endothelial cells, placenta, fetal liver, and heart cells. B19 also binds to other glycophospholipids found on granulocytes as well as kidney, liver, heart, and bowel cells. Therefore, infection with this virus tends to involve multiple organ systems. For infants, the suppressed fetal bone marrow leads to chronic anemia, which is not well tolerated by the fetus, and congestive heart failure develops leading to severe anemia. Parvovirus B19 may also directly affect the cardiac muscle function, which may also contribute to the disease (203). A number of other congenital abnormalities have been reported among infants with Parvovirus B19 infection, but causation has not been established.
Diagnosis
The diagnosis of infection is frequently made clinically in children when they present with a characteristic rash (197). The presence of Parvovirus B19-specific IgM antibody is the usual method of diagnosing new or recent infection. It is present within 4 days of the rash appearing and lasts for approximately 4 months. Parvovirus B19 IgG antibodies can be detected by the 2nd week of the illness. Seroconversion in pregnancy can be determined by comparing serologic test results of samples collected at the time of maternal disease or 2 to 3 weeks after suspected exposure with stored samples collected in early pregnancy. Also, Parvovirus B19 can be detected in blood samples using PCR technology, but the virus may be detectable by this method for several months following the acute infection. Women found to have seroconverted during pregnancy are followed closely. In those for whom a suspicion of the development of hydrops fetalis is made, diagnosis of fetal infection can be made by a combination of testing the fetal blood for Parvovirus B19 IgM antibody and finding Parvovirus B19 DNA by PCR testing of amniotic fluid. Diagnosis of infection in the infant is made primarily by the detection of Parvovirus B19-specific antibody or the presence of Parvovirus B19 DNA in blood or tissues (204).
Treatment and Management
There is no specific treatment for Parvovirus B19. Although there was one published case in which IVIG was successfully used, this is not currently a recommended therapy (205). Essentially, the management of the hydropic fetus may include in utero blood transfusions (196). Postnatally, treatment is supportive and involves partial exchange transfusions or simple transfusions of packed red cells until the hemoglobin is stabilized. Infants diagnosed with hydrops fetalis should be delivered in a facility with neonatal tertiary care. These infants are difficult to manage in the early neonatal period. The majority will need respiratory assistance and mechanical ventilation, and this may be complicated by the presence of pulmonary edema as well as large pleural effusions and peritoneal ascites. These may need drainage urgently to facilitate resuscitation. The clinical criteria for deciding to do intrauterine fetal blood transfusion is complex as approximately two-thirds of infants diagnosed with Parvovirus B19-associated hydrops fetalis will have the hydrops resolve without specific treatment. Most of these were not those severely affected. Approximately one-third of affected fetuses also have thrombocytopenia. Therefore, if intrauterine transfusions are done, it is important to check the fetal platelet count and be prepared to administer platelets as exsanguination can occur during the procedure if the fetus is thrombocytopenic. In general, there are no long-term sequelae for those infants who recover, although there have been recent reports of adverse neurodevelopmental outcome although it is not clear whether this is related to the severity of illness in the neonatal period. They are not at risk of chronic infection. Individuals with active Parvovirus B19 infections should be placed on droplet precautions. Congenitally infected infants do not need to be put on additional precautions if the hydrops has resolved by the time of birth (206).
Malaria
There are five recognized strains of plasmodia parasites that can cause human malaria: P. falciparum, P. ovale, P. vivax, P. malariae, and P. knowlesi (207,208). These parasites have a complex life cycle involving developmental stages in both the anopheline mosquito vector and the human host. In brief, sporozoites are injected into the human skin along with the saliva at the time of a bite by an infected mosquito. They are transported to the liver via blood stream dissemination. Within the liver, they invade the hepatocytes and rapidly divide until mature schizonts are formed. These schizonts all contain thousands of daughter cells (merozoites). This phase of infection is termed the exoerythrocytic stage. The schizonts then rupture, the timing of which is species specific; the shorted time period involves P. falciparum, which takes from 6 to 16 days. This releases the merozoites into the blood stream where they invade the erythrocytes (erythrocytic stage). The merozoites mature within the erythrocyte from ring forms, to trophozoites to mature red cell schizonts and are then released. The majority of merozoites from the schizonts then reinfect the surrounding erythrocytes, and the erythrocytic cycle starts over again. The timing of this process differs for different species of parasites and is 24 hours for P. knowlesi, 48 hours for P. falciparum, P. vivax, and P. ovale, and 72 hours for P. malariae. Some of the merozoites differentiate into male or female gametes, which then are ingested by an anopheles mosquito during another blood meal. The sexual forms complete their life cycle within the midgut of the mosquito and then travel to the salivary glands to be injected into the human host at the next meal. In P. vivax and P. ovale infection, some of the parasites are not released from the hepatocytes with the initial infection and form hypnozoites that can remain dormant for several months or years before being released. Neither P. falciparum nor P. malariae form hypnozoites, but P. malariae infection can be complicated by a late relapse several years after the initial infection despite this. The distribution of the various malarial parasites is not static, and there are areas now seeing renewed endemic disease. Also, the resistance to antimalarial drugs is also expanding and changing quite rapidly. Malaria in pregnancy is a major problem in several regions of the world, and it is estimated that 10,000 women and 200,000 infants die as a result of malarial infections during pregnancy (209). The risk of severe disease, maternal death, and poor pregnancy outcome is highest among primigravidas living in high prevalence endemic regions, among pregnant women in hypoendemic regions and among pregnant women who travel from a malaria-free (such as most of North America) or low endemic region to a high endemic region during their pregnancy (210,211,212,213). P. falciparum is the species associated with the greatest risk followed by P. vivax.
Pathophysiology and Clinical Presentation
The degree of illness associated with malaria is based on the degree of parasitemia during the erythrocyte phase, which is, in turn, related to the species of parasite with P. falciparum producing the highest parasite load, the degree of previous specific immunity to the parasite and the status of the immune system in general. Pregnant women have a greater risk than do nonpregnant women. Pregnant women who are also HIV seropositive have an even greater risk of severe disease (214,215,216). Women who live in highly endemic regions are more likely to have experienced one or more episodes of malaria and so are more likely to be partially immune. They are still at risk of acquiring malaria but are less likely to have severe disease. Women who leave areas of high endemic activity lose this partial immunity over time and are therefore more susceptible if they return. The reason that primigravida women have a great risk of severe disease in highly endemic regions is that, at least for P. falciparum, there is a pregnancy-specific immunity to malaria. Erythrocytes infected with certain clones of P. falciparum have the ability to sequester in the intervillous spaces of the placenta (217). Placental malaria occurs in approximately 40% of affected primigravida pregnancies (range 16% to 63%) compared with approximately 20% in multigravidas (range 12% to 33%) (218,219). Placental infection can be detected even in the situation where peripheral smears do not yield the parasite. Pregnancy tends to select for those clones that have the ability to infect the placenta (pregnancy-associated malaria), and with successive pregnancies in endemic areas, women become partially immune to these clones. Interestingly, women make specific antibodies to these clones while men do not. These specific P. falciparum clones express a class of variant surface antigens (VSAs) that result in the parasite-infected erythrocytes having the ability to adhere to chondroitin sulfate A, found on the syncytiotrophoblast lining, leading to syncytial degradation and occasionally localized villus destruction. Placental infection can also occur with P. vivax, but the mechanism appears to be different (220). Placental infection with P. falciparum has been suspected to influence neonatal immune responses to malarial challenge in the first year of life along with altered susceptibility to other pathogens and some vaccines (21). Infants born to primigravida mothers with placental malaria have a more balanced general Th1/Th2 immune response to antigen challenges over all compared with other infants. Placental malaria appears to affect transplacental antibody transfer and so infants have lower titers of antibodies at birth to a number of viral and bacterial pathogens, thus increasing their susceptibility to them earlier in the neonatal period. Interestingly, it is the infants of multiparous mothers who developed placental infection in more than one pregnancy who appear to have the greatest altered response to malaria during infancy resulting in increased susceptibility and risk of more severe disease. It may be that there is a genetic factor at play here as well.
The symptoms of malaria in the pregnant woman are similar to those of the nonpregnant adult (207,221). Almost all nonimmune individuals will present with fever. Once established, the fevers may be clearly periodic and reflect the cyclical release of parasites from the infected erythrocytes into the blood, which tends to become synchronized after the first few cycles. The time periods then reflect the species involved with periods of fever being every 24 hours for infection with P. knowlesi, 48 hours for P. falciparum, P. vivax, and P. ovale, and 72 hours for P. malariae. Frequently, the patient has chills, sweats, headaches, myalgias, fatigue, nausea, abdominal pain, vomiting, diarrhea, and/or cough in association with the fever spikes. Pregnant women are more likely to have severe hypoglycemia (58%) compared with nonpregnant women (8%). In the situation of severe malaria, there is significant anemia, jaundice, sequestration of erythrocytes in the brain (cerebral malaria) and kidney (black water fever) leading to death (222,223). Mothers remain at higher risk of severe disease for 2 to 3 months after delivery. However, in situations where the mother is partially immune, the infection may be asymptomatic with only anemia as a clinical sign that the infection has occurred. For the fetus, maternal infection can result in low birth weight (10% to 20%) or fetal loss (6% to 8%).
Congenital infection can occur with all species, but P. falciparum and P. vivax are the two species in which this has been described most frequently. For mothers who are partially immune, the actual risk of transmission to the fetus is low (0.1% to 1.5%); however, it may be as high as 10% for previously nonimmune mothers. In endemic areas, distinguishing congenital infection from mosquito-borne disease is not always possible. In nonendemic areas, that a mother had malaria is not always appreciated. Infants with congenital malaria generally present in the first 2 months of age with irritability, fever, anemia, thrombocytopenia, hyperbilirubinemia, splenomegaly, hepatomegaly, feeding difficulties with vomiting, and/or diarrhea. Infants with congenital P. vivax malaria may present at several months of age.
Diagnosis
The clinical diagnosis of malaria and of congenital malaria is based on the presence of maternal or infant symptoms, maternal present or past residence or visit to an endemic area and clinical suspicion of disease based on unexplained maternal anemia and/or thrombocytopenia. The standard method of determining if malarial parasites are present, their speciation, and the degree of parasitemia is examination of Giemsa-stained thick and thin blood smears (224,225). If examined by an expert, the specificity and sensitivity are excellent although low levels of parasitemia may be missed, which can happen in the situation of placental malaria where the burden in the blood is low as the parasites are sequestered in the placenta. Species identification is based on the characteristics of the parasites on the thin blood smear. The degree of parasitemia can be recorded as the number of parasites per microliter of blood or the percent of erythrocytes infected. Rapid detection tests and molecular diagnostic testing can also be done in some situations.
Infants born to mothers who were successfully treated for malaria do not need to be routinely screened at birth but should they develop any signs compatible with the disease, they should be tested. However, even asymptomatic infants born to mothers with suspected or diagnosed malaria not successfully treated, should have testing done as soon as possible after birth. In all cases where malaria is suspected, the placenta should be submitted for examination for the malarial parasites.
Treatment and Management
Treatment choices of malaria in pregnancy depend on the suspected or identified species, the degree of parasitemia if P. falciparum is suspected, and the clinical illness (226). Adverse effects in pregnancy of most antimalarial drugs have not been extensively studied. However, the potential severity of the disease and risk of maternal and fetal mortality dictate that treatment with these compounds should not be withheld. In general, management of a pregnant woman with malaria residing in nonendemic regions should be done in consultation with an infectious disease specialist or travel medicine specialist. Treatment protocols vary over time as resistance patterns change. The CDC Web site is a reference source most commonly used to help guide therapy based on prevalence of various malarial species and the antimalarial resistance patterns in the regions (http://www.cdc.gov/malaria). However, pregnant women with severe disease due to P. falciparum are usually treated with therapy that may include clindamycin with either artesunate or quinine (227). Quinine is associated with hypoglycemia, which can adversely affect the fetus. Chloroquine can be used for chloroquinesensitive malarial strains. The use of doxycycline and primaquine is generally contraindicated in pregnancy and while breastfeeding.
There are limited clinical studies to guide therapy (226). As stated previously, the choice of medications is dependent on the malarial species. One suggested treatment guideline is as follows, but treatment of an infant with congenital malaria is best done in consultation with an expert in infectious diseases:
Mild infections or parasitemia with chloroquine-sensitive P. vivax, P. ovale, P. malariae, or P. falciparum:
Chloroquine orally 10 mg/kg for the first dose, followed by a second dose of 5 mg/kg after 6 hours then 5 mg/kg once a day for the next 2 days.
Primaquine is not needed for additional treatment as there is no tissue phase in congenital malaria.
Severe infection or infections with chloroquine-resistant P. falciparum
Quinine IV in 5% dextrose with the first dose being 20 mg/kg given over 4 hours in an ICU setting followed by 10 kg/kg every 8 hours IV until the medication can be given orally to complete a 7-day course, plus
Clindamycin 10 mg/kg as a first dose then 5 mg/kg/dose given three times per day for 7 days of treatment, also given IV until medication can be given orally.
Supportive therapy includes hydration and monitoring for hypoglycemia.
Preventive strategies include deferment of travel by pregnant women to areas in which malaria is endemic. If travel is necessary, then measures should be taken to reduce exposure to mosquitoes, along with use of insect repellent and malaria chemoprophylaxis. Pregnant women should be advised to seek medical assessment if signs or symptoms compatible with malaria occur. Women should also be advised to report the details of any travel to a malarial area (both travel previous to and during the pregnancy) when presenting for delivery.
Tuberculosis
Mycobacterium tuberculosis, the causative agent of tuberculosis, is an acid-fast staining aerobic bacteria (AFB) (228). It is found worldwide and is the leading cause of illness and death. It is estimated that more than 2 billion people are infected with M. tuberculosis (about one-third of the world’s population), 9 million develop tuberculosis disease, and 2 million die of it each year (229). In North America, the highest prevalence of infection and incidence of disease are among new immigrants from high endemic countries and among the some First Nation communities in northern and western Canada (230). There is a close association between HIV infection and tuberculosis (231). The prevalence and incidence of tuberculosis in pregnancy is not known nor is the incidence of congenital tuberculosis.
Pathophysiology and Clinical Presentation
The pathophysiology of tuberculosis in pregnancy is similar to that of the nonpregnant woman (232). Pregnant women are no more likely to contract tuberculosis or reactivate latent disease more frequently than those who are not pregnant. The usual route of infection is inhalation of the bacteria with deposition in the lung. The actual infectious dose is not known but may be as low as 10 organisms. Replication in the lung occurs over several weeks. Some bacteria spread to regional lymph nodes via infected macrophages and from there may be disseminated to other areas in the body including the genital area and the placenta, if a woman is pregnant. After 1 to 3 months, the body can mount a cell-mediated immune response and control the infection. At that point, the tuberculin skin test becomes positive. The affected regions in the lung are essentially walled off by deposition of fibrin and calcium, but viable M. tuberculosis bacteria remain. At this stage, the individual is considered to have latent tuberculosis (LTBI). These bacteria are responsible for reactivation tuberculosis if the individual becomes immune suppressed. Congenital tuberculosis occurs through two mechanisms (233). The first is dissemination to the placenta if a woman is infected during her pregnancy or if she develops reactivation disease during her pregnancy. Primary infection of the mother during pregnancy tends to result in more severe disease for the fetus. The second mechanism is by direct infection from previously established maternal genitourinary tuberculosis. Infection can start at the time of menarche and may be asymptomatic for a long period. The ovaries, fallopian tubes, the uterus, and the cervix can all be infected. The most common symptom is infertility and so this route of infection for the infant occurs less often.
Maternal primary infection with M. tuberculosis is commonly asymptomatic or the illness produced is so mild that it is unrecognized (234,235). Only approximately 30% will have any pulmonary symptoms, which is usually just nonspecific cough. Some will develop retrosternal or pleural chest pain. Fever can be present and usually occurs as low-grade increases in temperature occurring for several days or weeks. Malaise, and fatigue and weight loss can occur, but these symptoms may not be easily distinguished in early pregnancy. In primary pulmonary tuberculosis, the chest radiograph may be normal, just show hilar adenopathy, show hilar adenopathy with a collapsed right middle lobe or show a pneumonia with or without hilar adenopathy and with or without pleural effusion. The changes in the chest radiograph take months to resolve. Maternal reactivation disease may only present with weight loss, cough, and fatigue. Over time, fever and night sweats occur in approximately 50%, chest pain in 30%, dyspnea in 30%, and hemoptysis in 25%. Chest radiographs are helpful in the diagnosis as most patients will have abnormalities present and so are appropriate to do in pregnant women as part of the investigation of potential tuberculosis (236). In tuberculosis reactivation, infiltrates are classically seen in the apical-posterior segments of the lungs in 80% to 90% of cases. Alternatively, infiltrates are seen in the superior segment of the lower lobes or the anterior segment of the upper lobes. Cavitation occurs in 20% to 40%. Granulomas due to M. tuberculosis can occur in other organs in addition to the genitourinary system, particularly bone and brain.
Congenital tuberculosis can present at birth or in the first few weeks of life (233). The clinical signs are related to the location and the size of the granulomatous lesions. Approximately 75% will have hepatomegaly in association with liver function abnormalities. A primary complex in the liver or caseating hepatic granuloma is diagnostic of congenital tuberculosis. Around 70% will have respiratory symptoms, most with an abnormal chest radiograph with infiltrates and 50% with a miliary pattern of disease. Occasionally, an infant will have a rapidly progressive pulmonary illness with the development of cavitary lesions. Other nonspecific findings include fever in approximately 50%, lymphadenopathy in approximately 40%, abdominal distention in 25%, and lethargy in 20%. One feature that has been described in from 15% to 20% of congenitally infected infants is tuberculosis of the ear presenting with chronic discharge. In approximately 10%, papular skin lesions will be seen. Other abnormalities that occur less frequently are apnea, vomiting, jaundice, seizures, cyanosis, and petechiae.
Diagnosis
The diagnosis of tuberculosis in pregnancy is based on clinical suspicion based on symptoms and a history of either direct exposure or residence in an area or region of higher tuberculosis prevalence. Miliary tuberculosis can be difficult to diagnose as the signs and symptoms may be nonspecific and so a high index of clinical suspicion based on likelihood of disease exposure is essential. Most cases of tuberculosis are acquired in the home or in crowded places. Pregnant women who are HIV seropositive should be tested for tuberculosis. Similarly, pregnant women diagnosed with tuberculosis should be offered HIV testing.
General screening for tuberculosis in low prevalence areas is not indicated (237). Testing should be done for women who are symptomatic, and tuberculosis is in the differential diagnosis. It should also be done in situation where there is an indication for prompt treatment of LTBI. These would be women who have a high risk for progression to active disease due to being immune suppressed (HIV, on immune suppressive therapy for other conditions, etc.) and those suspected to have been recently infected.
Diagnosis for LTBI in pregnancy includes a chest radiograph with appropriate shielding of the fetus along with either tuberculin skin testing (TST) or interferon gamma release assays (IGRAs) (237). IGRAs have been recently introduced, and there is no indication that they are either less sensitive or less specific in pregnant women. The TST requires a trained individual to interpret the test. The interpretation of the TST is dependent on the size of the induration at the test site measured 48 hours after the planting of the antigens, immune competence of the mother, and the risk of infection:
A test is positive if the induration is ≥5 mm for women
With HIV infection
With a known close contact with an actively contagious individual
Abnormal chest radiograph typical of previous tuberculosis
Immunosuppressed
A test is positive if the induration is ≥10 mm for women
With clinical conditions that increase the risk of reactivation
Silicosis
Chronic renal failure requiring dialysis
Diabetes mellitus
Malignancies
Underweight
Injection drug users
Jejunoileal bypass
who are foreign born from countries where the incidence of tuberculosis is greater than that 25/100,000 population
who are residents or employees in high-risk settings
Prisons, jails, and other detention facilities
Health care facilities
Microbiology laboratories
Homeless shelters
who have both a low risk for contracting tuberculosis and exposure to nontuberculous mycobacteria (Canadians)
A test is positive if the induration is ≥15 mm for women in the United States who have a low risk for contracting tuberculosis but a high risk of exposure to nontuberculous mycobacteria (residents in the southern United States).
Neither the TST nor the IGRAs have been systematically studied for the diagnosis of congenital tuberculosis. Use of the IGRAs has been reported to be helpful in the early diagnosis of congenital tuberculosis when the TST was negative. For children exposed to tuberculosis in the perinatal period, the TST does not usually reliably become positive for a few months.
For suspected congenital tuberculosis and for the diagnosis of clinically symptomatic tuberculosis in pregnant women, bacterial cultures are preferred (237). Cultures of tissues including the placenta once delivered, fluid, or drainage from suspected infected sites should be sent to the microbiology laboratory specifically for acid fast bacilli (AFB) stains and AFB culture. For pulmonary tuberculosis in pregnant women, serial sputum samples should be sent. For infants, tracheal aspirates and gastric washing would be necessary as they do not produce sufficient sputum for culture. Blood cultures collected in blood culture tubes designed for mycobacterial isolation may be helpful in some cases. Smears are now usually stained with acid-fast fluorochrome dye, auramine O, which has better sensitivity than the classic Ziehl-Neelsen stains. Rapid probes can now be used to confirm the diagnosis on specimen samples, which are positive on staining and on cultures when growth is detected. Compared with other bacteria, it is relatively slow growing taking from 7 to 21 days to grow in liquid media and 2 to 6 weeks on solid media. Determination of drug sensitivity takes an additional 2 to 4 weeks of testing.
Treatment and Management
Asymptomatic pregnant women who are diagnosed with LTBI may, or may not, be offered therapy during pregnancy depending upon the risk assessment that is made as to whether she is likely to progress to active disease (237). For those not treated during pregnancy, treatment is usually deferred for 3 months after delivery to reduce the risk of maternal hepatitis. At the time of starting treatment in the postpartum period, the mother should be reassessed for the development of active, contagious disease. For women treated for LTBI in pregnancy, the usual medications that are given include isoniazid with pyridoxine supplementation or rifampin. The most common complication of these medications is hepatitis, and women should be monitored regularly for this. Other rarer complications include neuropsychiatric problems that can involve mania, depression and memory problems, peripheral neuritis, seizures, thrombocytopenia, hemolytic anemia, fever, and rash.
Women with uncomplicated active tuberculosis in pregnancy are treated in the same manner as nonpregnant women with the use of isoniazid, rifampin, and ethambutol as the first-line drugs (238,239). In the situation where there may be drug-resistant tuberculosis or the mother is coinfected with HIV, alternative regimens may be used, and their care is usually done in conjunction with an expert in tuberculosis and/or HIV care. Isoniazid, rifampin, and ethambutol are considered to be acceptable for use in pregnant women as there have not been any associated teratogenic effects. Hemorrhagic disease in the infant has been reported with rifampin use in pregnancy (240
Only gold members can continue reading. Log In or Register to continue