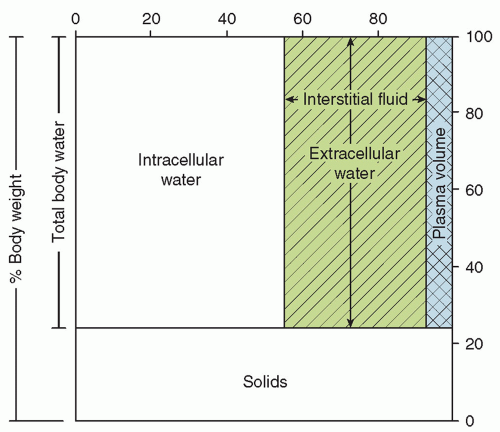
 FIGURE 19.1 Distribution of body water in a term newborn infant. |
postnatal changes in body water and its partition between ECW and ICW are influenced by developmental changes in neuroendocrine systems as well as the intake of water and electrolytes (18,19). Failure to allow the normal postnatal contraction of ECW in premature infants, often a result of inappropriately high water or electrolyte intake, may increase the risk of significant patent ductus arteriosus (PDA) (20), necrotizing enterocolitis (NEC) (21,22,23), and bronchopulmonary dysplasia (24,25). In the past, lack of postnatal weight loss has been associated with increased risk of bronchopulmonary dysplasia in very-low-birth-weight infants, but with improved early nutrition, postnatal weight loss is not inevitable, as the reduction in ECW is presumably offset by gain in lean body mass (26,27).
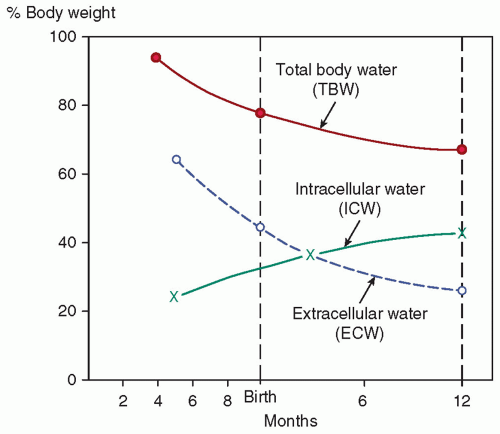 FIGURE 19.2 Changes in body water during gestation and infancy. Adapted from Friis-Hansen B. Changes in body water compartments during growth. Acta Paediatr Suppl 1957;46:1-68, with permission. |
TABLE 19.1 Changes in Body Water and Electrolyte Composition during Intrauterine and Early Postnatal Life | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
using direct measurements of transepidermal water loss (45). It is now understood that the higher IWL with radiant warmers arises from the lower ambient water vapor pressure and not from higher air velocity or a direct effect of nonionizing radiation on the skin. The same phenomenon explains the effect of phototherapy on IWL of infants in incubators operated by skin temperature servocontrol. The effects on IWL of radiant warmers and phototherapy are additive; the IWL with the combination is approximately twice as large as in an incubator without phototherapy (37,40).
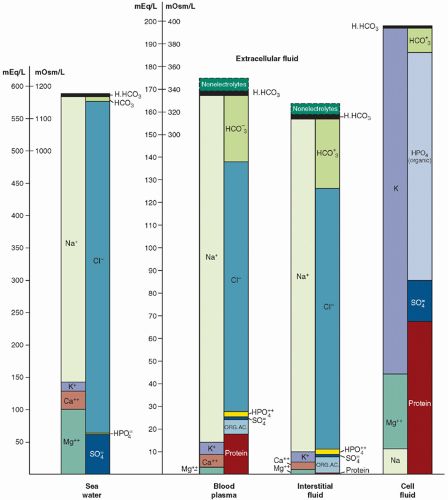 FIGURE 19.3 Ion distribution in seawater, blood plasma, and interstitial fluid, and in the intracellular fluid compartment. The similarity between seawater and extracellular fluid is striking. As noted by Macallum (28): “The vertebrate kidney, therefore, by its control over the concentration of the inorganic elements in the blood plasma and by its maintenance therein of the paleo-ratios, has thus perpetuated in the blood of vertebrates the ocean water of the early Cambrian if not of the late Proterozoic.” |
endotracheal tube) if respiratory support is required. If the temperature and water content of the inspired and expired gas are the same, the respiratory IWL will be entirely eliminated. Increasing ambient humidity, for example in an incubator, reduces total IWL, but respiratory IWL is decreased more than is cutaneous IWL (31); a threefold increase in ambient water vapor pressure, from an average of 7 to 25 mm Hg, resulted in a 30% reduction in total IWL. Increasing ambient humidity is facilitated by the design of certain recent models of incubators. The use of incubator humidification systems should not be overlooked as a way of reducing IWL and total fluid requirements (59). Modern incubators allow adjustment of the ambient humidity, which, in turn, affects IWL and water requirement.
TABLE 19.2 Factors Affecting Insensible Water Loss in Newborn Infants | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
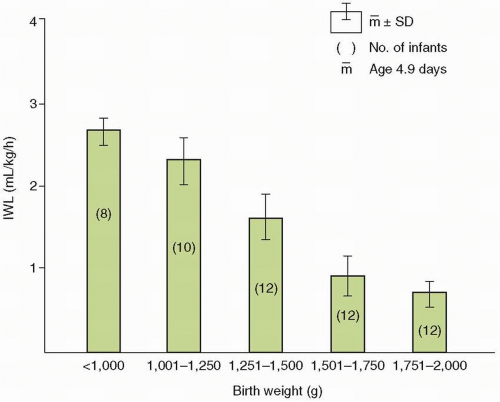 FIGURE 19.4 Relation between insensible water loss (IWL) and birth weight of 5-day-old (mean) infants in incubators. Data from Wu PY, Hodgman JE. Insensible water loss in preterm infants: changes with postnatal development and non-ionizing radiant energy. Pediatrics 1974;54:704-712, as redrawn in Shaffer SG, Weismann DN. Fluid requirements in the preterm infant. Clin Perinatol 1992;19:233-250, with permission. |
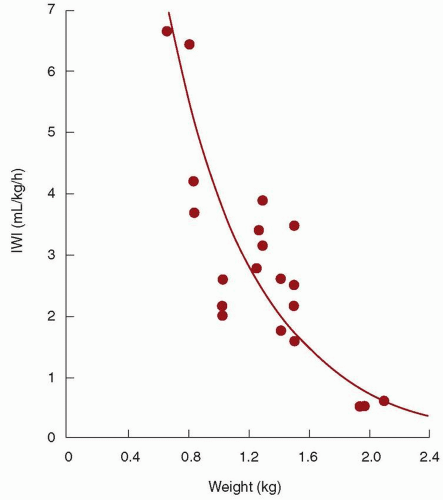 FIGURE 19.5 Insensible water loss (IWL) as a function of birth weight in premature infants nursed under radiant warmers. Adapted from Costarino AT, Jr., Gruskay JA, Corcoran L, et al. Sodium restriction versus daily maintenance replacement in very low birth weight premature neonates: a randomized, blind therapeutic trial. J Pediatr 1992;120:99-106. |
making appropriate adjustments in water intake with changes in care. Of all infants, premature and critically ill infants are the ones whose IWL is most profoundly influenced by these factors. This is especially true for the extremely premature infant. However, these are exactly the infants for whom precise maintenance of fluid and electrolyte balance is most important and for whom the margin for error is smallest.
TABLE 19.3 Average Insensible Water Loss (mL/kg/d) of Premature Infants in Incubators | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||



