● FETAL HETEROTAXY WITH LEFT AND RIGHT ATRIAL ISOMERISM
Definition, Terminology, and Incidence
Situs Solitus and the Right-Sided and Left-Sided Organs
The embryologic development of abdominal and thoracic structures follows a spatially controlled and coordinated manner, leading to well-defined right-sided and left-sided anatomic positions within the body (1). Right-sided structures include a major part of the liver, the inferior and superior venae cavae, the right atrium with its appendage, and a trilobed right lung with an eparterial bronchus (see Table 6.2) (Fig. 30.1). Left-sided structures include the stomach, the spleen, the left atrium with its appendage, the pulmonary veins, and a bilobed left lung with a hyparterial bronchus (see Table 6.2) (1). Normal development and positioning of abdominal and thoracic organs is referred to as situs solitus (solitus means common) for the visceral arrangement, and levocardia (heart on the left side) for the thoracic arrangement of organs (1–4). For situs and segmental approach refer to Chapter 6.
Situs Inversus
Situs inversus refers to a mirror-image arrangement of the visceral and thoracic structures to that of situs solitus and is discussed at the end of this chapter.
Situs Ambiguous
Any arrangement of visceral and/or thoracic organs other than situs solitus or situs inversus is referred to as situs ambiguous (unknown or complex situs). Situs ambiguous, unlike situs solitus or inversus, is often associated with various anomalies, including anomalies of the spleen, either as asplenia or as polysplenia. The term cardiosplenic syndrome was first used to describe situs ambiguous associated with anomalies of the spleen. Since the spleen is not always abnormal in situs ambiguous and cannot be reliably used for classification, the term heterotaxy syndrome has been suggested (3, 4) for the changes in the abdominal situs. Heterotaxy syndrome (in Greek, heteros means different and taxis means arrangement) is a general term that is used to describe the complete spectrum of abnormal organ arrangement, including conditions such as asplenia and polysplenia (Figs. 30.2 and 30.3) (1). Since many pathologists observed that the subgroups of asplenia and polysplenia are better classified by describing the atrial morphology than the abdominal changes, the term right and left atrial isomerism (in Greek, iso means same and meros means turn) has been suggested and used (5) (Figs. 30.2 to 30.4). Visceral heterotaxy involves an irregular arrangement of the nonpaired solitary abdominal organs. Isomerism of the thoracic organs is characterized by a rather symmetric arrangement of the otherwise asymmetric structures, including the atria and lungs (2), thus allowing a classification into two main groups: bilateral left-sidedness, also called left atrial isomerism (or earlier polysplenia) (Fig. 30.2), and bilateral right-sidedness, also called right atrial isomerism (or earlier asplenia, or Ivemark syndrome) (Fig. 30.3).
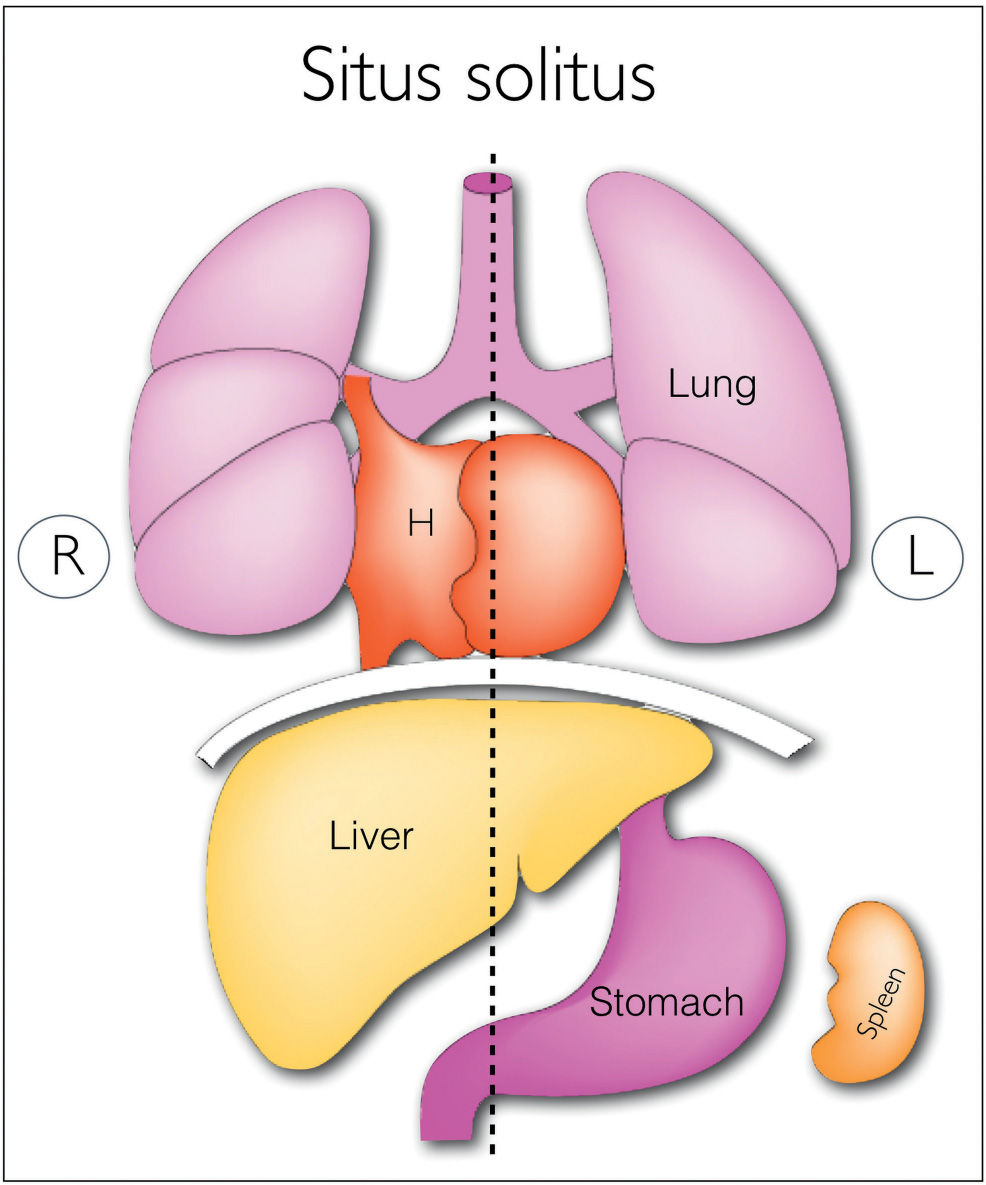
Figure 30.1: Schematic drawing of normal situs (situs solitus) showing the thoracic and abdominal organs in their normal left (L) and right (R) positioning. The right lung is trilobed while the left lung is bilobed. Stomach and spleen are on the left side. Liver is on the right side. About one-third of the heart (H) is on the right side and two-thirds on the left side. The inferior and superior venae cavae are draining into the morphologic right atrium along the right side of the chest. (Modified from Fliegauf M, Benzing T, Omran H. When cilia go bad: cilia defects and ciliopathies. Nat Rev Mol Cell Biol. 2007;8:880–893, with permission.)
Incidence of Disease
Heterotaxy syndrome, including right and left atrial isomerism, is found in between 2.2% and 4.2% of infants with congenital heart disease (6, 7). In fetal series, left isomerism is more common than right isomerism. In postnatal series, right isomerism is more common owing to an increased incidence of in utero demise of fetuses with left isomerism due to complete heart block and hydrops (2). Fetal heterotaxy has an increased risk of recurrence in subsequent pregnancies, and that risk has been reported in up to 10% in some series (8). A genetic etiology for heterotaxy recurrence that may include autosomal dominant, autosomal recessive, X-linked, and single gene disorder, especially primary ciliary dyskinesia, has been suggested (1, 9–13). Recurrence of heterotaxy in families is not limited to the specific anomaly but may involve the full spectrum, including right or left isomerism and situs inversus.
Prenatal Suspicion of Heterotaxy Associated with Right and Left Atrial Isomerism
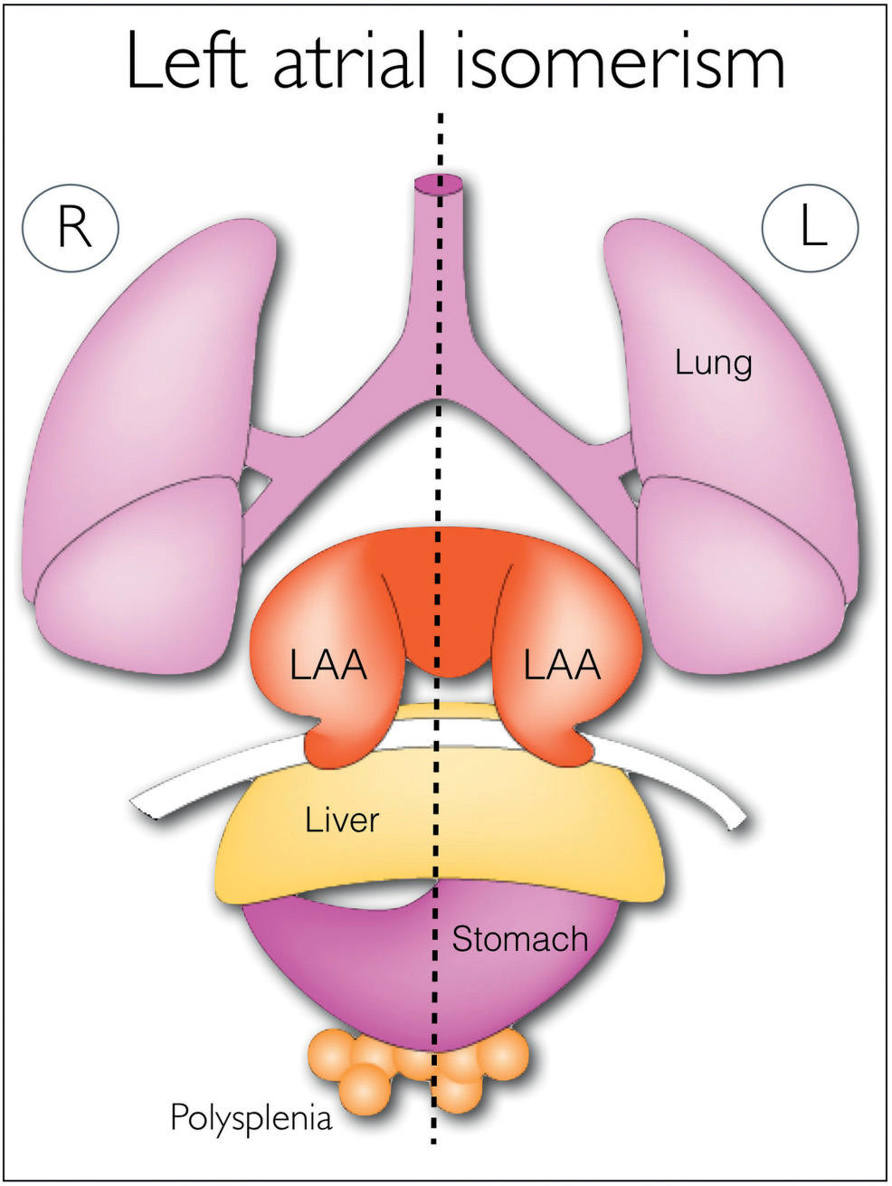
Figure 30.2: Schematic drawing of thoracic and abdominal organs in left atrial isomerism (polysplenia). In left atrial isomerism, also termed bilateral left-sidedness, the two lungs are morphologic left lungs with two lobes in each. Note the presence of bilateral left atrial appendages (LAA). The location of the liver and stomach can be left-sided (L) or right-sided (R). Polysplenia is also commonly seen. In many cases of left atrial isomerism, there is an interruption of the intrahepatic part of the inferior vena cava with azygos continuation. See text for details. (Modified from Fliegauf M, Benzing T, Omran H. When cilia go bad: cilia defects and ciliopathies. Nat Rev Mol Cell Biol. 2007;8:880–893, with permission.)
Suspecting the presence of isomerism in the fetus may be easy when careful examination of the chest and abdomen is performed, but the accurate classification into right or left isomerism remains challenging, as there are no typical pathognomonic cardiac malformations for these anomalies. The identification of the right or left atrial appendage on prenatal ultrasound may be possible in some conditions (14) (Fig. 30.5) but cannot be reliably used for classification (2). One of the most reliable signs remains the evaluation of vessel arrangement in the upper abdomen (see what follows) as is commonly used in postnatal echocardiography (15). In general, a reliable suspicion of right or left isomerism can be attained by assessing vessel arrangement in the upper abdomen in combination with intrathoracic findings. The main impact on outcome, however, is primarily dependent on the specific cardiac malformation rather than the actual classification. According to the authors’ experience, there are four common ways in which fetal isomerism is suspected and confirmed:
1. Fetal heart and stomach on opposing sides of the body, leading to the suspicion of situs abnormality and thus directing detailed ultrasound examinations of the chest and abdomen (Figs. 30.6 and 30.7)
2. The presence of complex cardiac malformation on an ultrasound examination, prompting a targeted segmental evaluation of the fetal situs and heart (Figs. 30.6 and 30.7)
3. The presence of complete heart block or other fetal arrhythmia with or without fetal hydrops on an ultrasound examination, which leads to a targeted evaluation of cardiac and abdominal anatomy (Fig. 30.8)
4. The detection of an anomaly of the venoatrial connection affecting either the inferior vena cava or the pulmonary veins, leading to a segmental evaluation of the cardiac anatomy (Figs. 30.7 and 30.9)
The main prenatal ultrasound features for left and right isomerism are presented in the following sections.
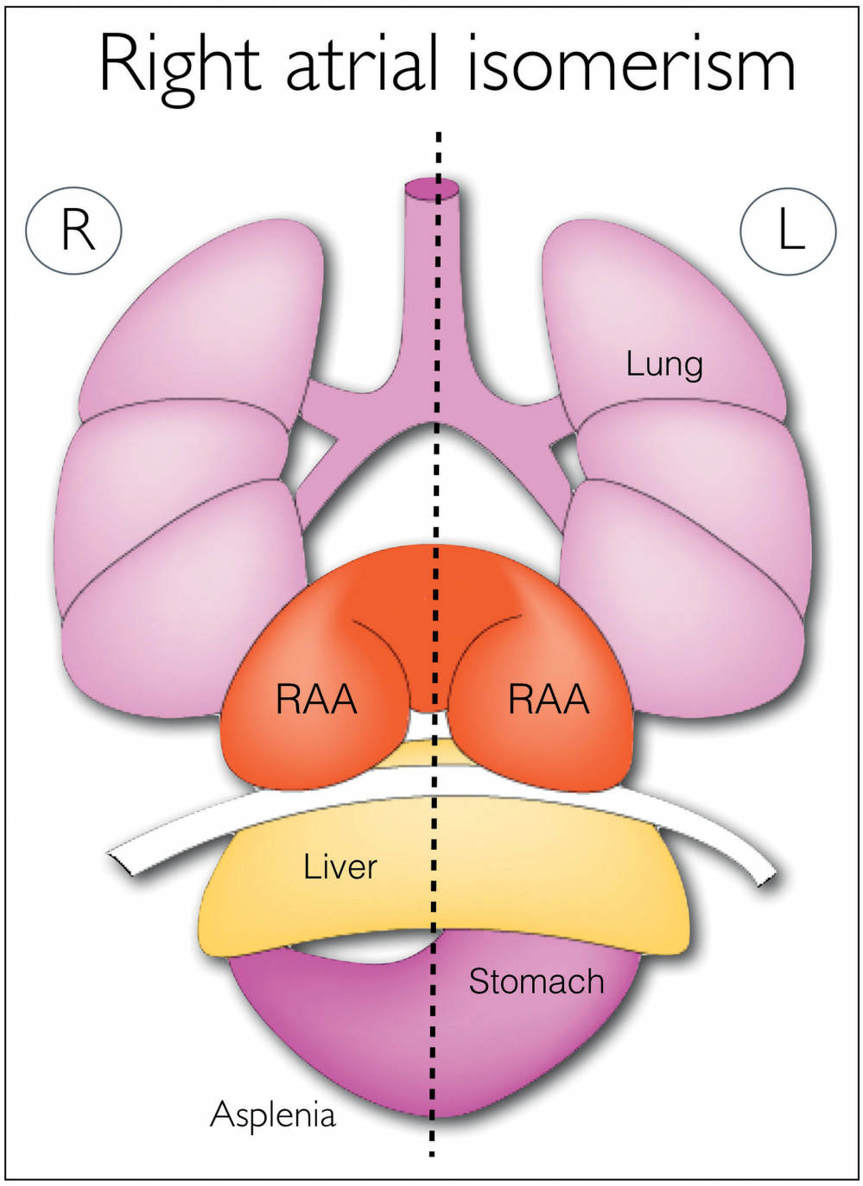
Figure 30.3: Schematic drawing of thoracic and abdominal organs in right atrial isomerism (asplenia). In right atrial isomerism, also known as bilateral right-sidedness, the two lungs are morphologic right lungs with three lobes each. Note the presence of bilateral right atrial appendages (RAA). The liver and stomach can be left-sided (L), right-sided (R), or in the midline position. There is commonly asplenia in association with right atrial isomerism. In many cases of right isomerism, abnormal connection of the pulmonary veins can be present. See text for details. (Modified from Fliegauf M, Benzing T, Omran H. When cilia go bad: cilia defects and ciliopathies. Nat Rev Mol Cell Biol. 2007;8:880–893, with permission.)
Ultrasound Findings in Left Atrial Isomerism (Polysplenia)
Left atrial isomerism is associated with the presence of “double” left-sided structures with the underdevelopment or absence of right-sided structures. One of the most common associations with left isomerism is the absence of the intrahepatic part of the inferior vena cava, a finding that is present in 80% to 90% of cases (2, 4). The inferior vena cava is interrupted at its suprarenal part and connects with the azygos (or hemiazygos) venous system (Figs. 30.9 to 30.11), which drains the abdominal venous blood to the heart. The azygos (or hemiazygos) vein is then dilated with its typical course side-by-side and slightly posterior to the descending aorta along the spine. The dilated azygos passes through the diaphragm and typically drains into the superior vena cava (see Fig. 31.18) or less commonly to a persistent left superior vena cava in the upper chest (Fig. 30.10). This condition, termed interruption of the inferior vena cava with azygos continuation, can be detected as a “double vessel” sign in a cross section of the upper abdomen (15, 16) (Fig. 30.9) or in a four-chamber view behind the heart (Fig. 30.10) (17). A parasagittal view of the abdomen and chest can also demonstrate the azygos vein posterior to the descending aorta (Fig. 30.11), and color Doppler can demonstrate the opposite direction of flow in the azygos vein and the adjacent descending aorta (Fig. 30.11). The hepatic veins may connect directly into the right atrium in the absence of an inferior vena cava.
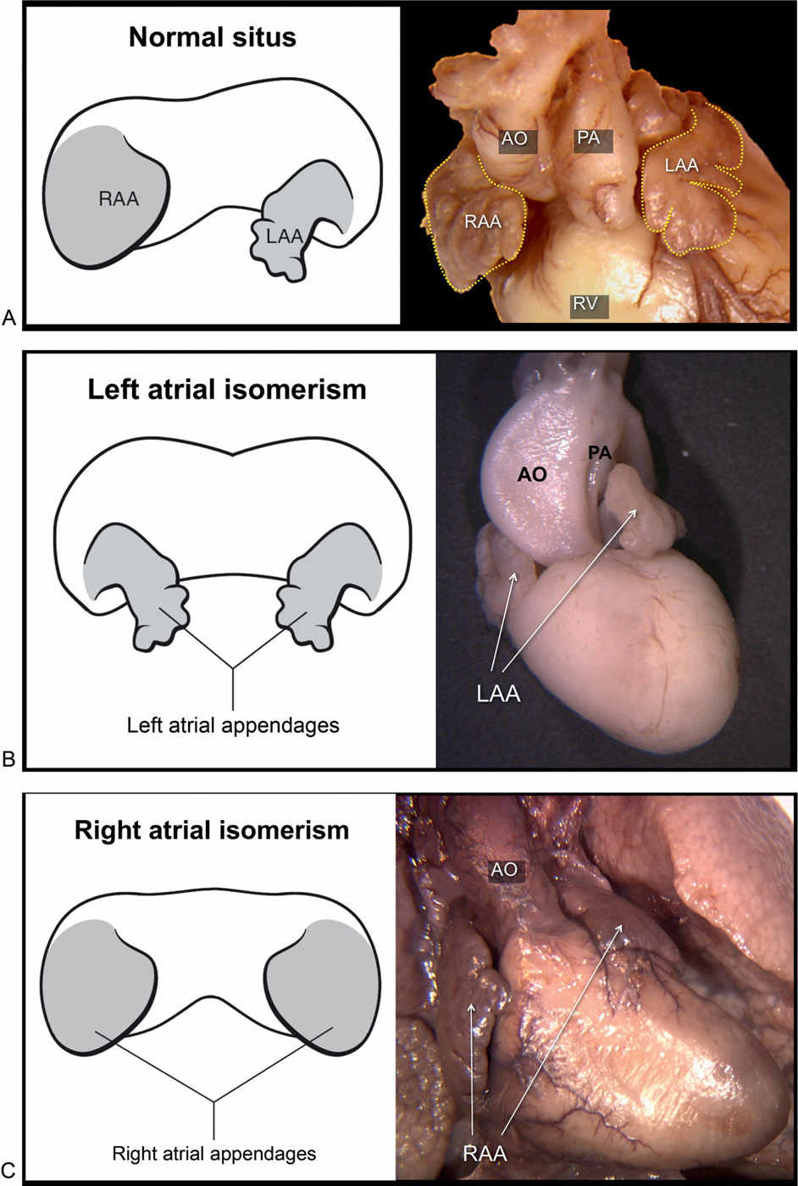
Figure 30.4: A represents an anterior view of a schematic drawing and an anatomic specimen of a normal fetal heart, demonstrating the right atrial appendage (RAA) with its broad pyramidal shape and its wide junction with the right atrium, and the left atrial appendage (LAA) with its fingerlike hook shape and its narrow junction with the left atrium. B represents an anterior view of a schematic drawing and an anatomic specimen of a fetal heart with left atrial isomerism, demonstrating two morphologic left atrial appendages with their typical fingerlike hook shape and narrow junction with the atria. The dilated aorta (AO) and narrow pulmonary artery (PA) are part of associated cardiac malformation. C represents an anterior view of a schematic drawing and an anatomic specimen of a fetal heart with right atrial isomerism, demonstrating two morphologic RAA with their typical broad pyramidal shape and wide junction with the atria. The single vessel arising from the heart is a dilated aorta as part of associated cardiac malformation. RV, right ventricle.
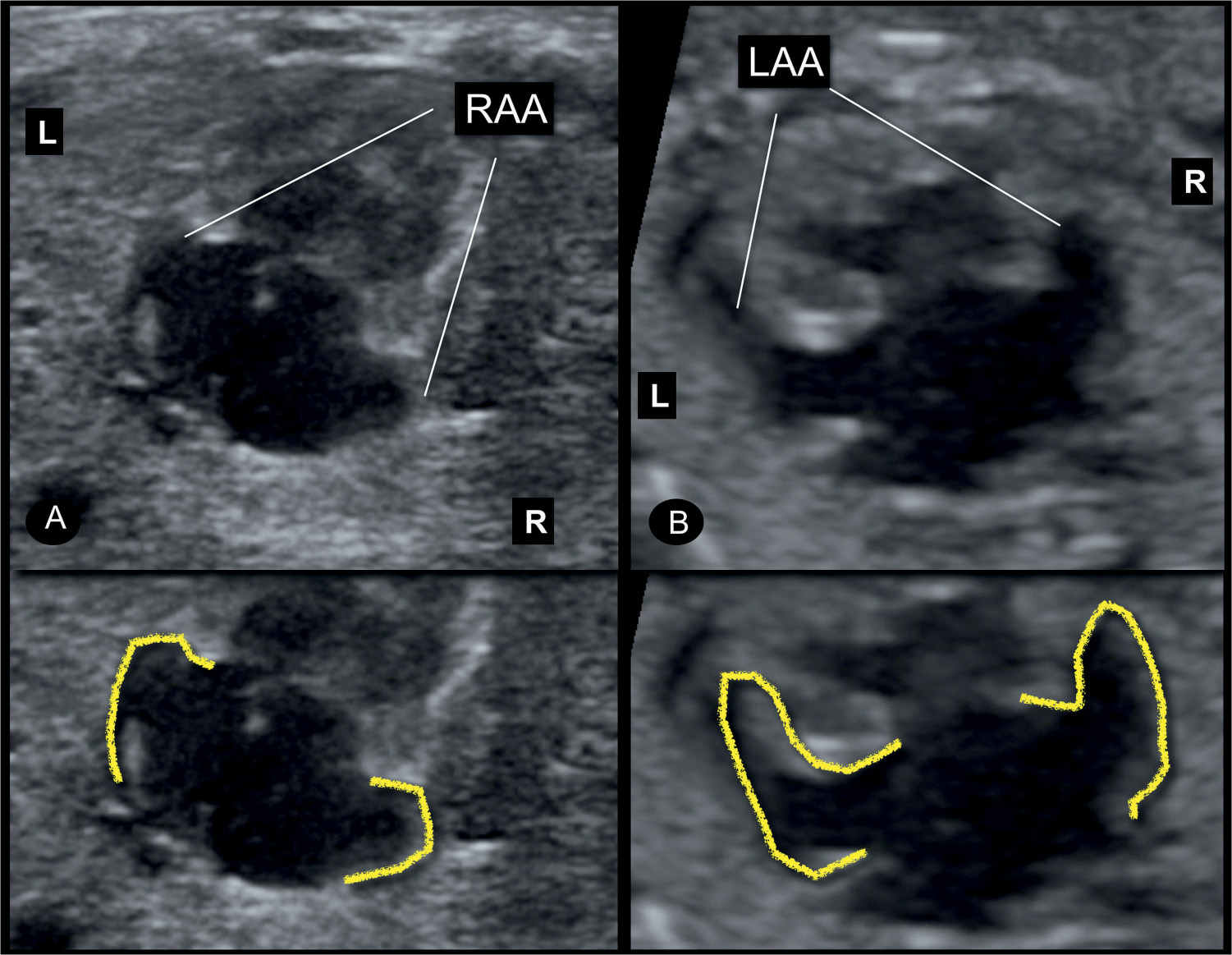
Figure 30.5: Apical four-chamber views of two fetuses with right (A) and left (B) atrial isomerism. Note the broad pyramidal shape of the bilaterally symmetric right atrial appendages (RAA) in A and the fingerlike hook shape of the bilaterally symmetric left atrial appendages (LAA) in B. It is rather difficult to recognize atrial morphology on ultrasound examination, and the diagnosis should be performed by relying on other ultrasound features. L, left; R, right.
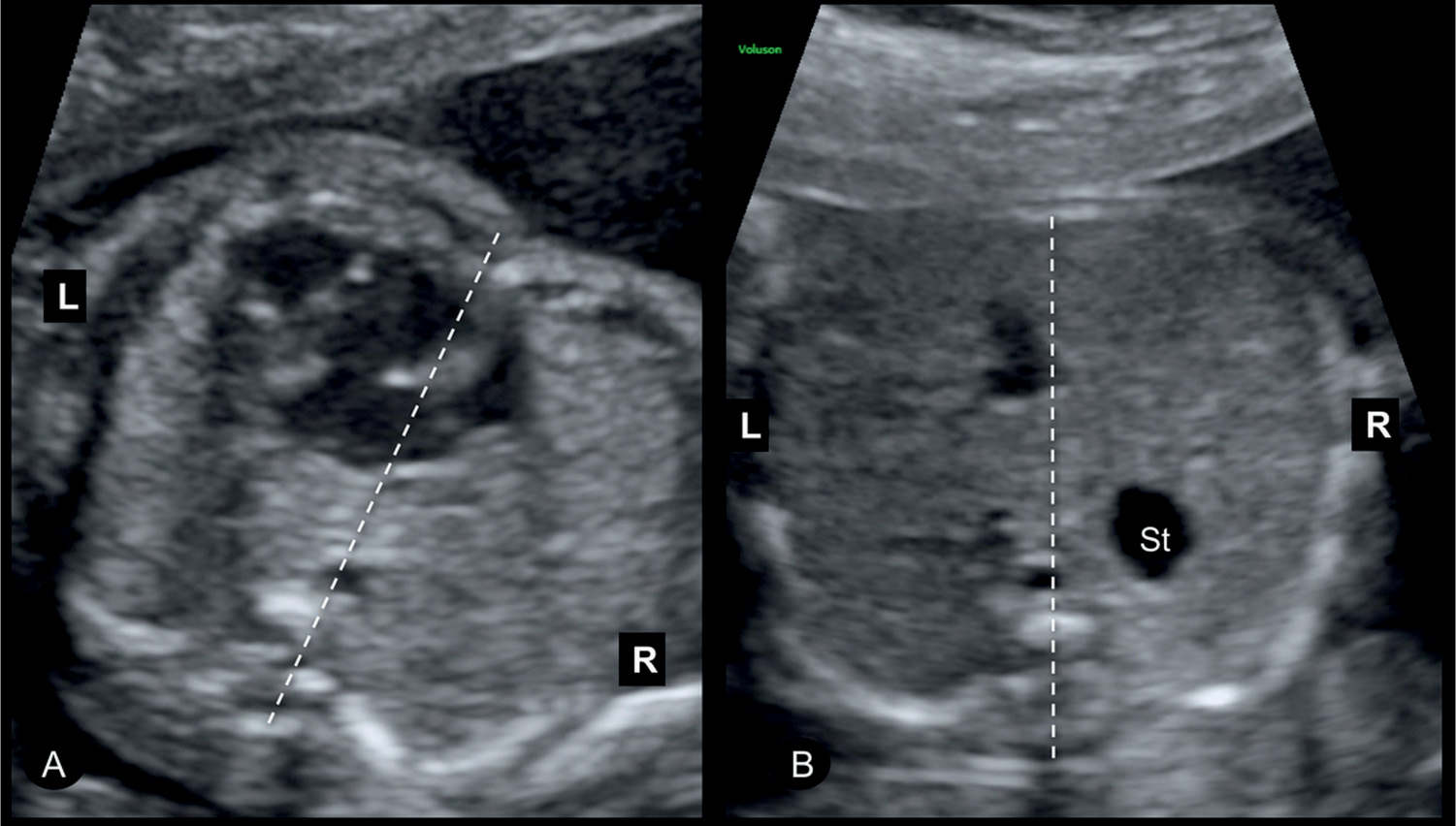
Figure 30.6: Axial views of the fetal chest (A) and abdomen (B) in a fetus with heterotaxy syndrome. Heterotaxy was suspected on ultrasound examination by the presence of the heart in the left side of the chest (A) and the presence of the stomach (St) in the upper right abdomen (B). Note the presence of an abnormal four-chamber view suggesting a complex cardiac malformation. L, left; R, right.
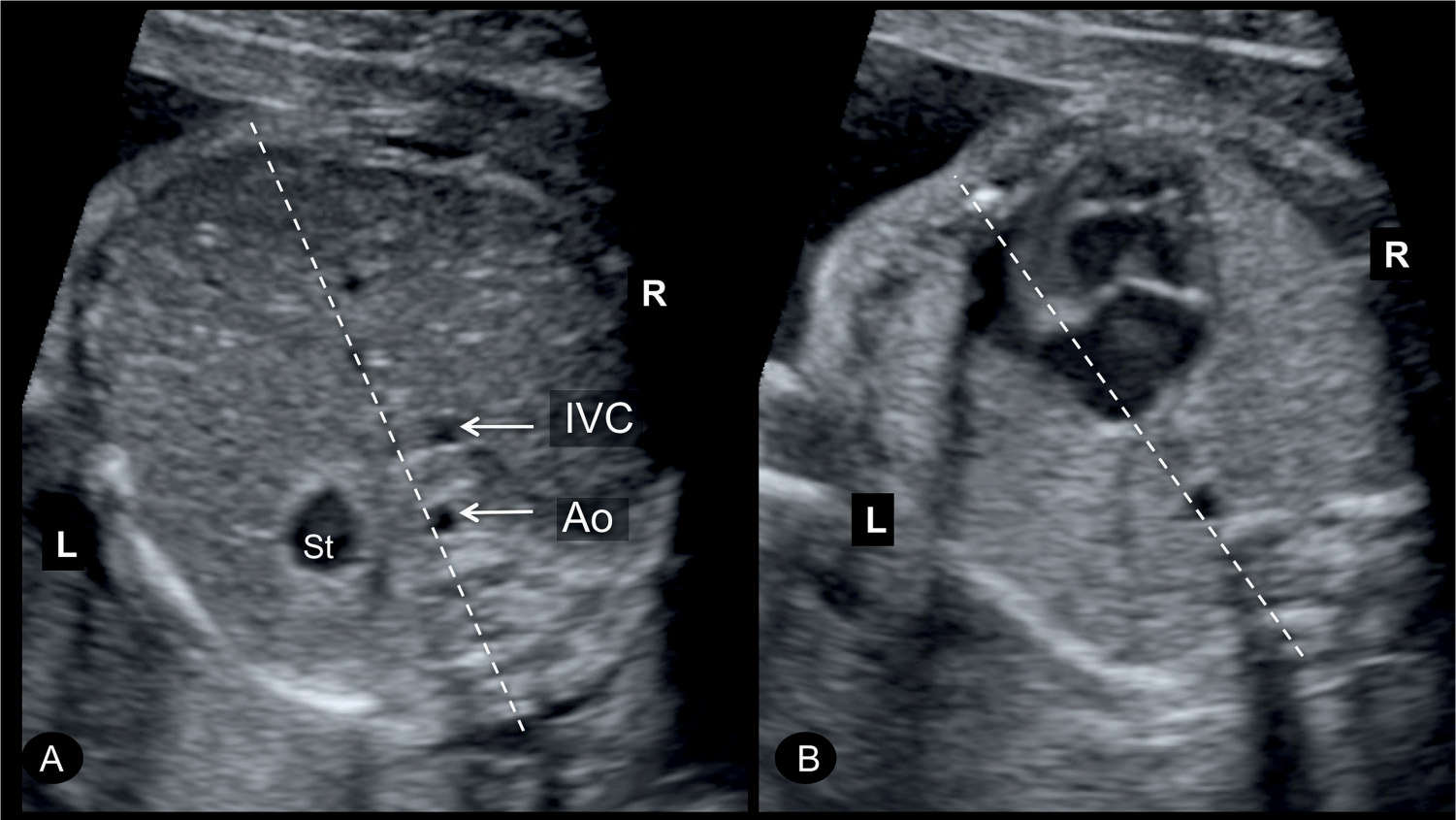
Figure 30.7: Axial views of the fetal abdomen (A) and chest (B) in a fetus with heterotaxy syndrome. Note the presence of the stomach (St) in the upper right abdomen (A) and the heart in the left side of the chest (B). The heart is abnormal showing a single ventricle. Note the descending aorta (Ao) and inferior vena cava (IVC) are on the right side. L, left; R, right.
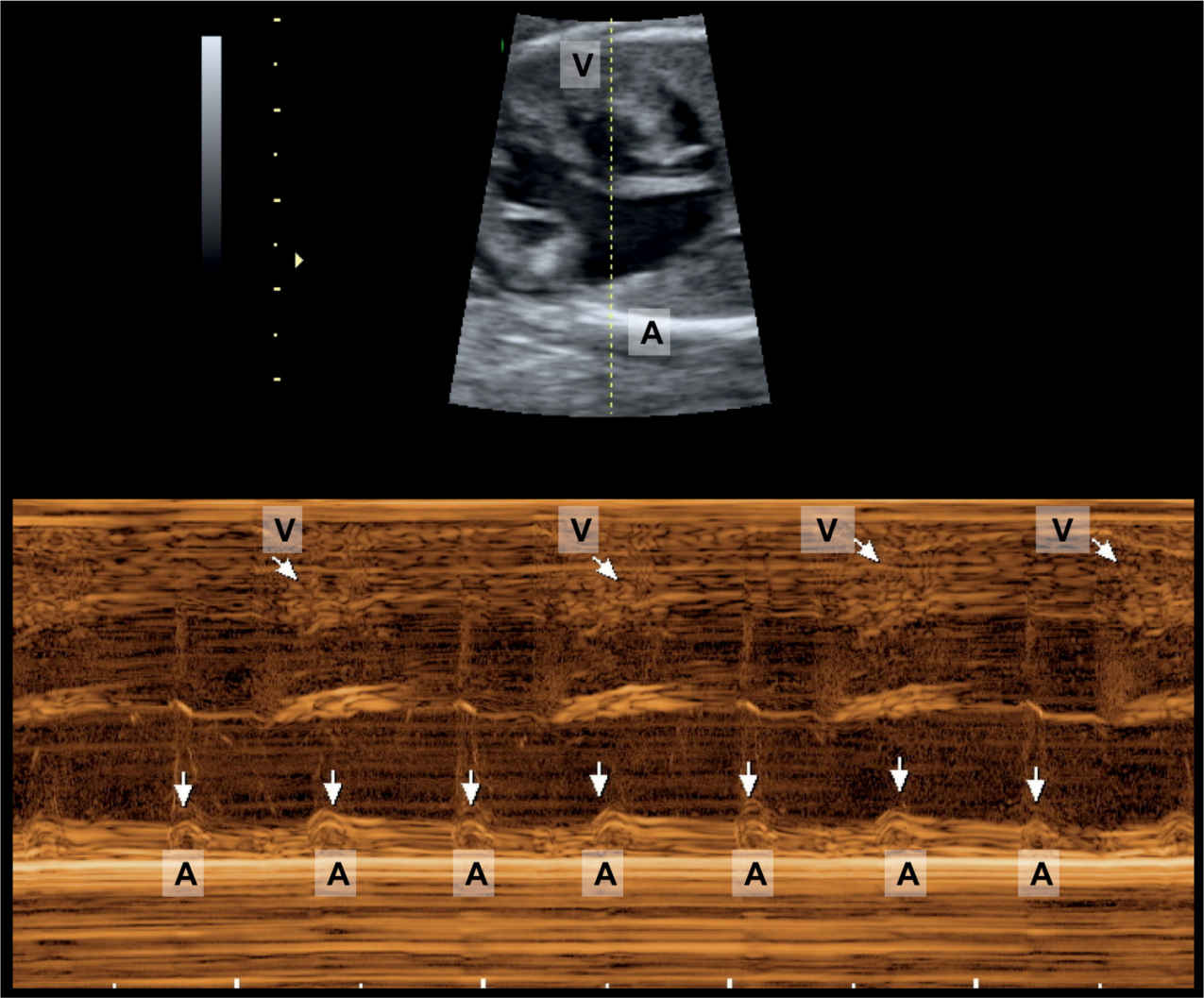
Figure 30.8: M-mode ultrasound across the fetal heart in a fetus with heterotaxy syndrome (left isomerism) initially suspected on ultrasound examination by the presence of heart block and congenital heart disease (atrioventricular septal defect). M-mode ultrasound shows a regular atrial (A) rhythm (vertical arrows) and a slow ventricular (V) rhythm (oblique arrows).
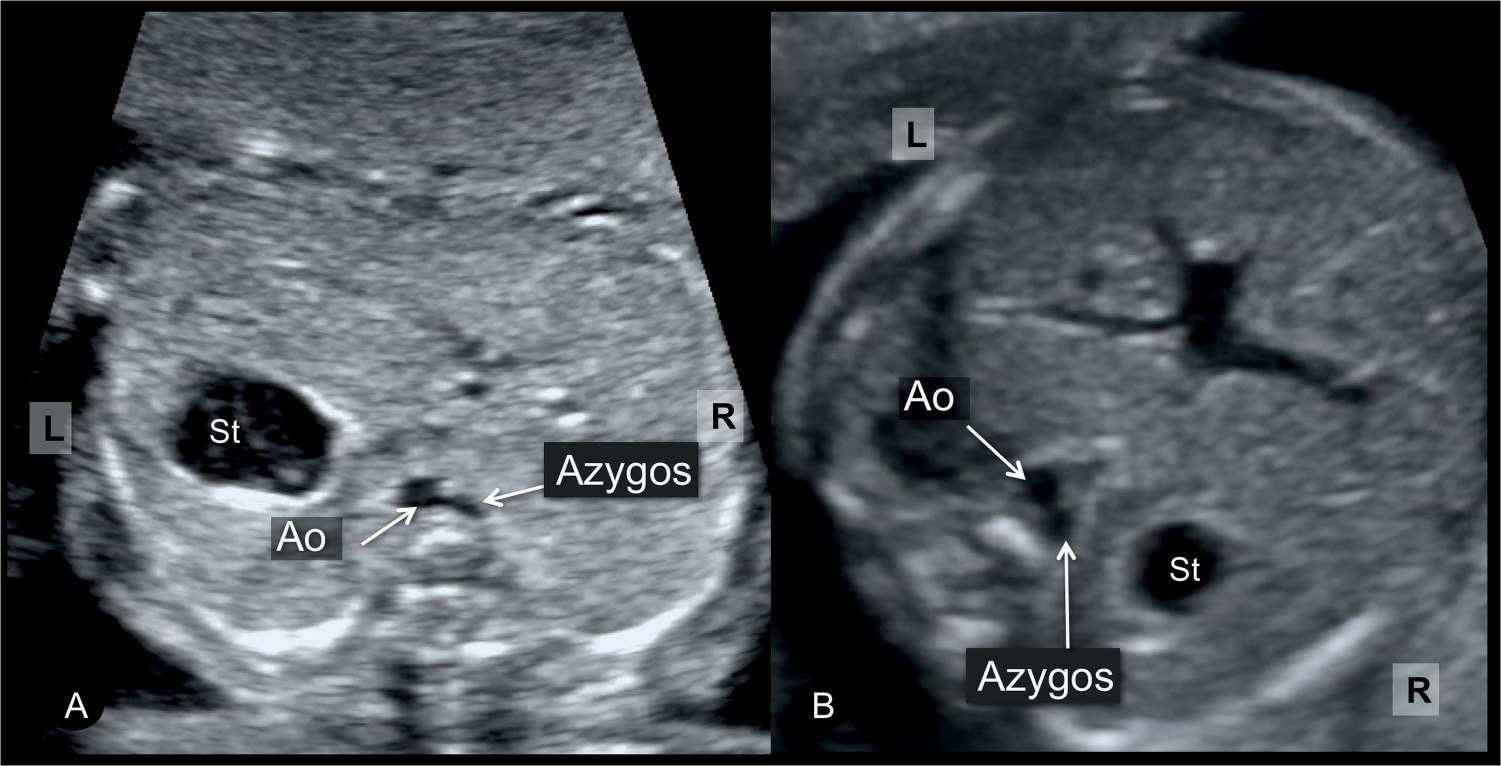
Figure 30.9: Axial views of the fetal abdomen in two fetuses (A and B) with left atrial isomerism showing various positions of the stomach (St) in the abdomen. Note that the stomach (St) is left-sided in A and right-sided in B. The position of the stomach in the abdomen is not of diagnostic importance in heterotaxy syndrome. The presence of a dilated azygos vein (double vessels in front of the spine) in both fetuses suggests the diagnosis of left atrial isomerism. Ao, descending aorta; L, left; R, right.
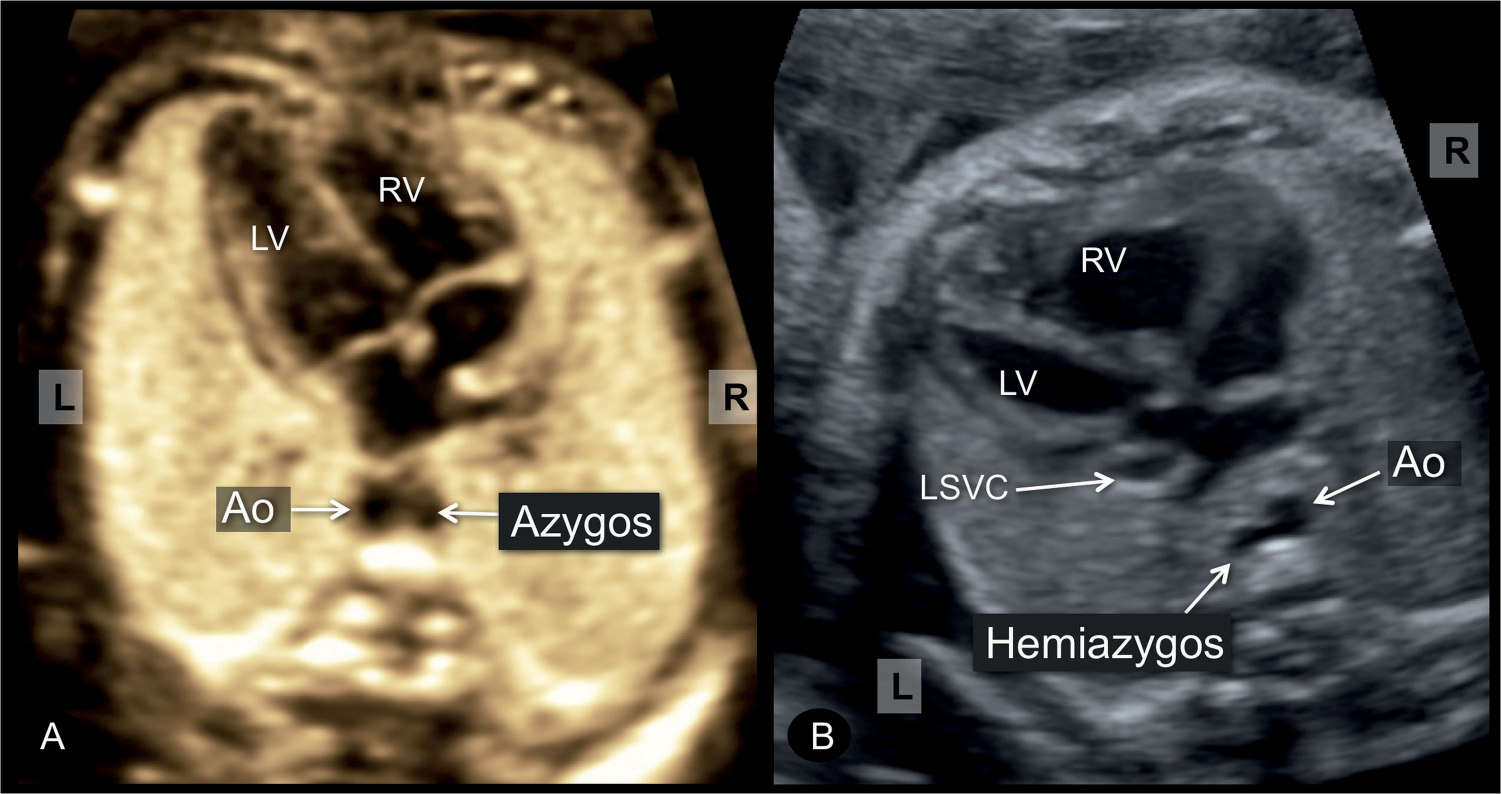
Figure 30.10: Axial views of the fetal chest at the level of the four-chamber view in a fetus with normal cardiac anatomy (A) and another fetus with a cardiac malformation (B). Note the presence of a dilated vessel next to the descending aorta (Ao) (double vessels sign) in front of the spine in both fetuses with the azygos vein in A and the hemiazygos vein in B. This suggests the presence of an interrupted inferior vena cava and left isomerism in both fetuses. In A, the dilated azygos vein drains into the superior vena cava, while in B the presence of a persistent left superior vena cava (LSVC) suggests that the hemiazygos vein drains into the LSVC in the upper mediastinum. L, left; R, right; RV, right ventricle; LV, left ventricle.
Another feature of left isomerism is the absence of the morphologic right atrium with its sinus node. This can lead in many conditions to bradyarrhythmia, commonly presenting as complete heart block (Fig. 30.8) and seen in 40% to 70% of cases (2, 4, 18). The combination of complete heart block with a complex cardiac anomaly, especially in an interrupted vena cava with azygos continuation, is typical for the presence of left atrial isomerism (3). The presence of complete heart block with a complex cardiac malformation may often lead to cardiac failure and fetal hydrops (Figs. 30.8 and 30.12B) in more than 30% of cases (2, 18) and is responsible for the high rate of in utero demise in these fetuses.
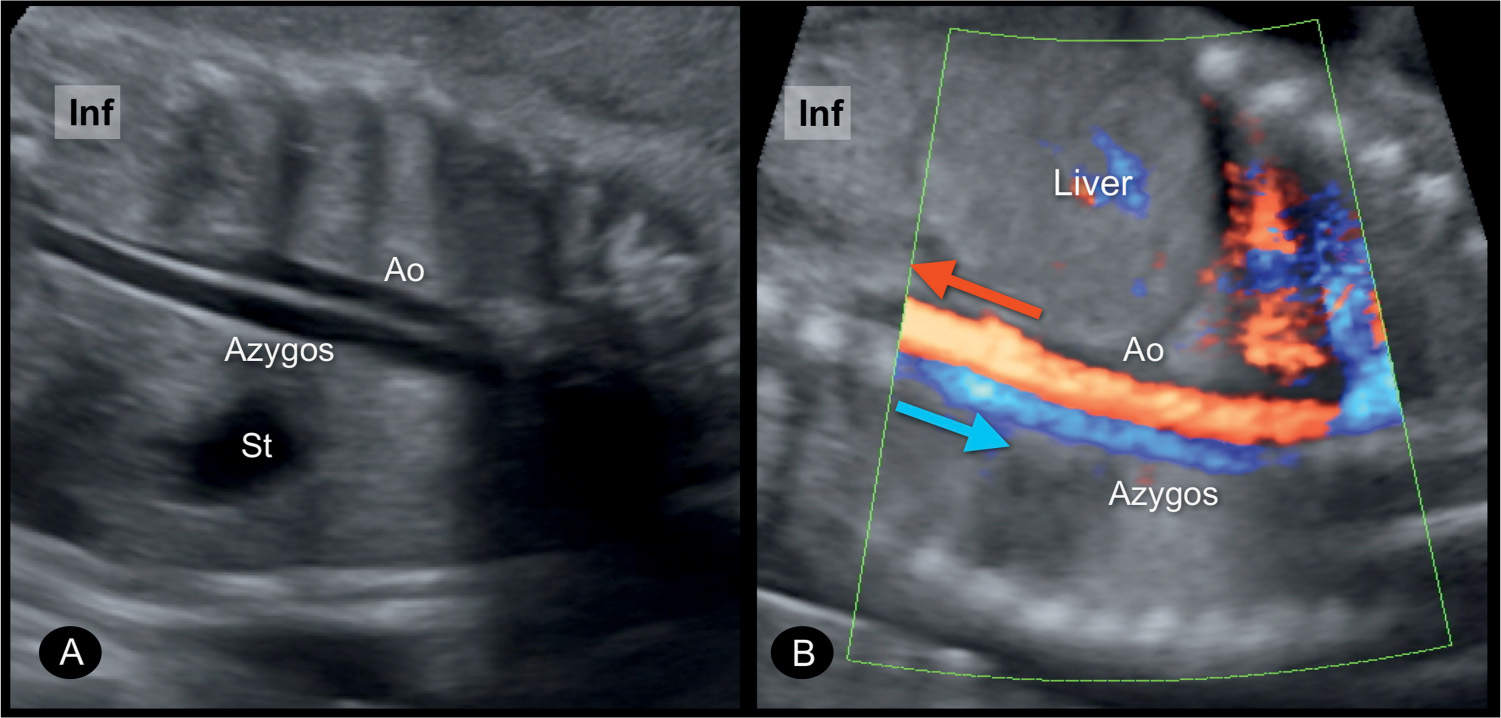
Figure 30.11: Coronal planes of the chest and abdomen in two fetuses (A and B) with left atrial isomerism and interrupted inferior vena cava, showing the azygos vein running parallel and posterior to the descending aorta (Ao). Color Doppler in B shows reverse direction of blood flow in the azygos vein (toward the heart) (blue arrow) to that in the aorta (away from the heart) (red arrow). St, stomach; Inf, inferior.
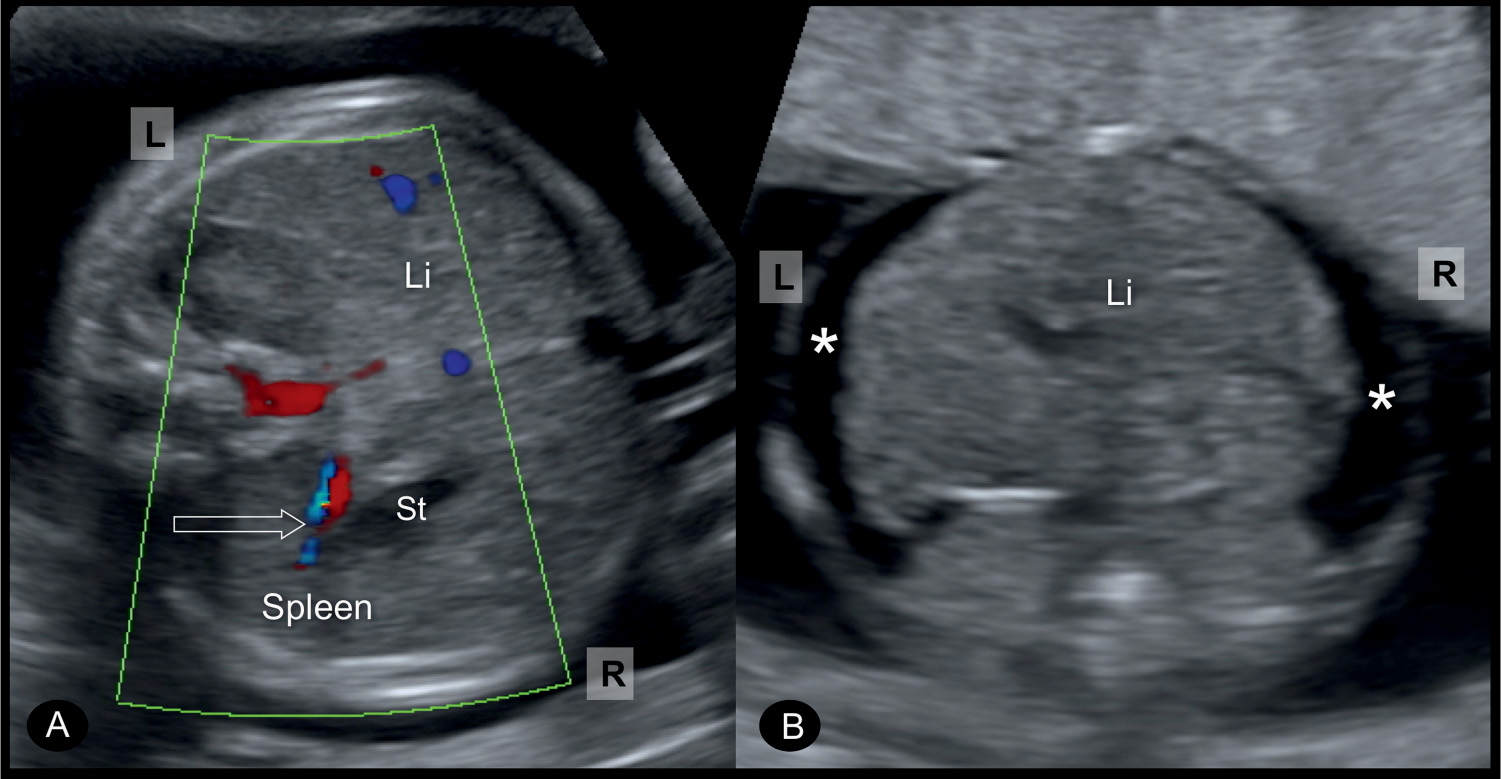
Figure 30.12: Axial views at the level of the fetal abdomen in two fetuses with left atrial isomerism. Note in A, the presence of a right-sided stomach (St) with color Doppler showing the splenic artery and vein (open arrow), which confirms the presence of one or multiple spleens and thus rules out asplenia. The fetus in B has left isomerism with heart block and fetal hydrops. Note the location of the liver (Li) in B in the midline of the abdomen and the presence of ascites (asterisks), which suggests poor prognosis. L, left; R, right.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


