Although knowledge is increasing from randomized trials, the majority of these recommendations are based on observational human and animal data but have not been rigorously tested. It is expected that in the future, some of these recommendations will undergo close scrutiny and possible change.
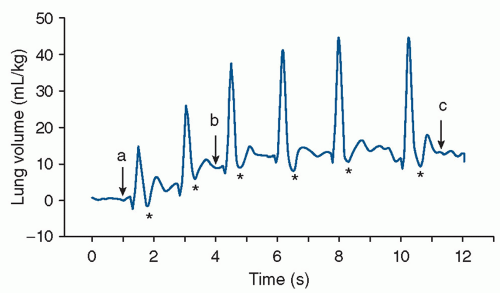 FIGURE 17.1 Plethysmography recording of breathing activity and the increase in end-expiratory lung gas volumes from birth in a spontaneously breathing newborn rabbit pup delivered near term. The recording demonstrates that pups can rapidly generate an end-expiratory lung air volume of approximately 16 mL/kg within 10 to 12 seconds of the onset of breathing. Note that the end-expiratory lung air volume increases with each breath. Phase-contrast x-ray images were acquired at the times indicated by the arrows in the plethysmography recording and demonstrate the increase in lung aeration associated with each breath (a, b, c). Reductions in gas volume immediately following inspiration (asterisk) are recording artifacts. From Hooper SB, Siew M, Kitchen MJ, et al. Imaging lung aeration and lung liquid clearance at birth. FASEB J 2007;21:3329, with permission. |
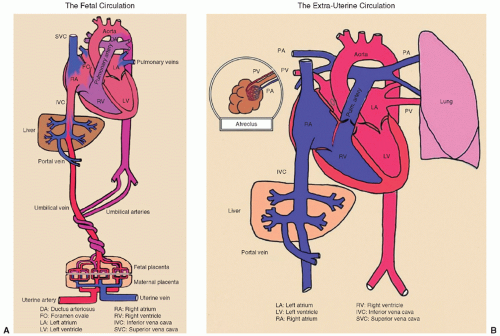 FIGURE 17.2 A and B: Fetal and neonatal circulation. From David Atkinson, MD, David Geffen School of Medicine at UCLA, with permission. |
insufficient or excessive oxygenation can be harmful to the newborn infant (14,15). Percentiles of oxygen saturation as a function of time from birth in uncompromised babies born at term have been recently published (Fig. 17.4) (16). To appropriately compare oxygen saturations to similar published data, the probe should be attached to a preductal location (i.e., the right upper extremity, usually the medial surface of the palm). During respiratory support, a special emphasis should be given to prevent oxygen-induced lung injury by providing the lowest level of oxygen supplementation that maintains adequate delivery of oxygen to tissues (17,18,19). Studies suggest that resuscitation with 100% oxygen may generate oxygen free radicals, which may cause tissue damage, particularly to the brain (15,20,21). Therefore, continuous monitoring of oxygen saturation should start in the DR by using recently published nomograms (Fig. 17.4) to reduce overall oxygen exposures (16). The current resuscitation guidelines recommend to start resuscitation in room air in all term infants (4). Although, for preterm infants, no definitive recommendation has been made (4), there is increasing evidence that DR resuscitation of preterm neonates with an initial oxygen of less than 30% is feasible, decreases oxygen exposure without increasing need for additional resuscitation, and decreases oxidative stress (18,19,22). In the absence of DR studies comparing important clinical outcomes such as bronchopulmonary dysplasia and long-term neurodevelopment, neonatal resuscitation of preterm infants should be initiated with air or a blended oxygen and titrating the oxygen concentration to achieve an oxygen saturation value in the interquartile range of preductal saturations measured by pulse oximetry (Fig. 17.4) (4,16).
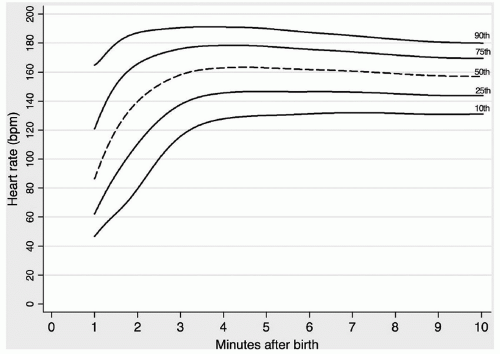 FIGURE 17.3 The 10th, 25th, 50th, 75th, and 90th HR centiles for all infants with no medical intervention after birth. bpm, beats per minute. Dawson J, Kamlin O, Wong C, et al. Changes in heart rate in the first minutes after birth. Arch Dis Child Fetal Neonatal Ed 2010;95:F177. |
TABLE 17.1 Some Factors That Place the Newborn at High Risk for Asphyxia | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 17.2 Fetal Heart Rate Patterns Associated with Fetal and Neonatal Distress | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
of atelectrauma and improve respiratory function in different ways: (a) CPAP reduces upper airway obstruction by decreasing upper airway resistance and increasing the pharyngeal cross-sectional area; (b) both CPAP and PEEP increase FRC; (c) CPAP and PEEP reduce inspiratory resistance by dilating the airways and allow a larger tidal volume for a given pressure with a reduction in the work of breathing; (d) CPAP and PEEP increase the compliance and tidal volume of stiff lungs with a low FRC by stabilizing the chest wall; (e) CPAP and PEEP increase the mean airway pressure and improve ventilation-perfusion mismatch; (f) PEEP conserves surfactant on the alveolar surface; (g) as CPAP and PEEP increase lung volume, oxygenation is also improved (23).
TABLE 17.3 Team Assignment During Neonatal Resuscitation | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
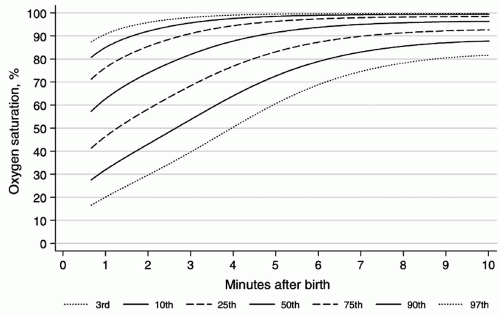 FIGURE 17.4 Third, 10th, 25th, 50th, 75th, 90th, and 97th SpO2 percentiles for all infants with no medical intervention after birth. Dawson J, Vento M, Kamlin O, et al. Defining the reference range for oxygen saturation for infants after birth. Pediatrics 2010;125:e1340. |
negative pressure, produces a fall in inflation pressures but results in a transient increase in tidal volume. Of course, the neonate may demonstrate no response to the inflation attempt, that is, not generating any change in intraesophageal pressure during PPV, and passive inflation subsequently results. It is important to recognize that these physiologic responses to PPV in the DR may cause large variability in the tidal volume and intrapulmonary pressures, despite delivery of constant inflation pressure.
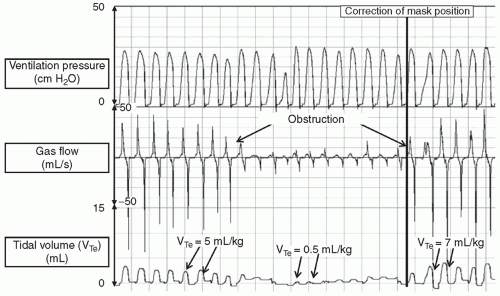 FIGURE 17.5 Airway obstruction during mask PPV in a very preterm infant with a self-inflating bag. Initially, PPV delivered an expired tidal volume (VTe) of 5 mL/kg. Both inflation and expiratory flow waves rapidly reduced in size. This is reflected in the VT curve, which displays a 90% reduction in VTe. By correcting the face mask position, the tidal volume is restored. Throughout PPV, the peak inflation pressure is achieved. From Schmölzer GM, Dawson J, Kamlin O, et al. Airway obstruction and gas leak during mask ventilation of preterm infants in the delivery room. Arch Dis Child Fetal Neonatal Ed 2011;96:F254, with permission. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


