● COMPLETE TRANSPOSITION OF THE GREAT ARTERIES
Definition, Spectrum of Disease, and Incidence
Complete transposition of the great arteries (TGA) is a common cardiac malformation with atrioventricular concordance and ventriculoarterial discordance. This implies a normal connection between the atria and ventricles; the right atrium is connected to the right ventricle through the tricuspid valve and the left atrium is connected to the left ventricle through the mitral valve, but there is a switched connection of the great vessels, the pulmonary artery arising from the left ventricle, and the aorta arising from the right ventricle. Both great arteries display a parallel course, with the aorta anterior and to the right of the pulmonary artery (Fig. 28.1), hence the term D-TGA (D = “dexter”). D-TGA is a relatively frequent cardiac anomaly occurring in 5% to 7% of all congenital cardiac malformations, with an incidence of 0.315 cases per 1,000 live births and a 2:1 male preponderance (1). D-TGA can be an isolated cardiac malformation, termed simple D-TGA, or complex, when associated with other cardiac anomalies. Figure 28.2 shows an anatomic fetal specimen of a heart with a simple D-TGA. Ventricular septal defects (VSDs) and pulmonary stenosis (left ventricular tract outflow obstruction) are common associations with D-TGA and may be present either alone or in combination in up to 30% to 40% of cases (2). Associated extracardiac malformations are rare.
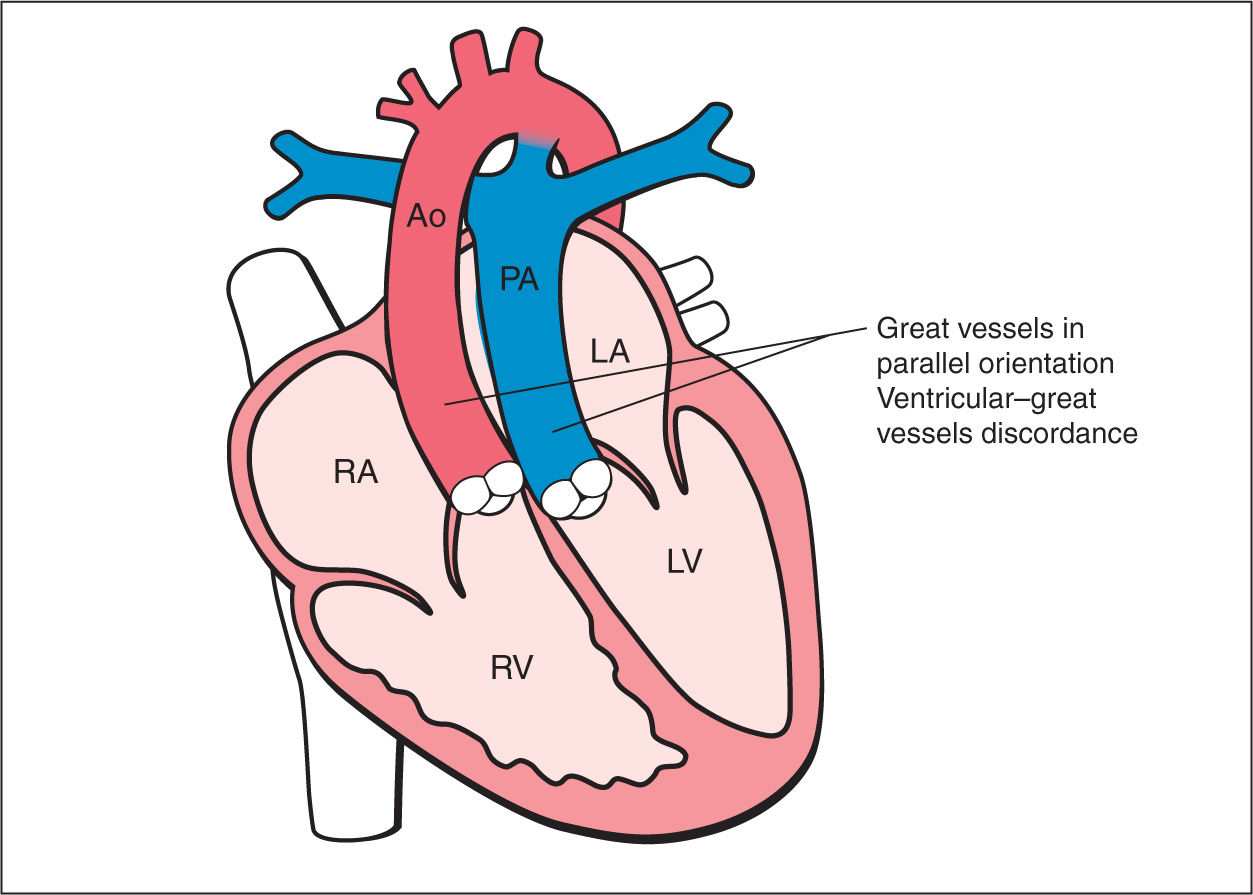
Figure 28.1: Schematic drawing of complete transposition of the great arteries (D-TGA). Note the following features: (1) normal four-chamber anatomy with normal atrioventricular connections, (2) ventriculoarterial discordance, with aorta (Ao) arising from the right ventricle (RV) and the pulmonary artery (PA) arising from the left ventricle (LV), and (3) parallel course of great vessels, with aorta anteriorly and to the right of the pulmonary artery. RA, right atrium; LA, left atrium.
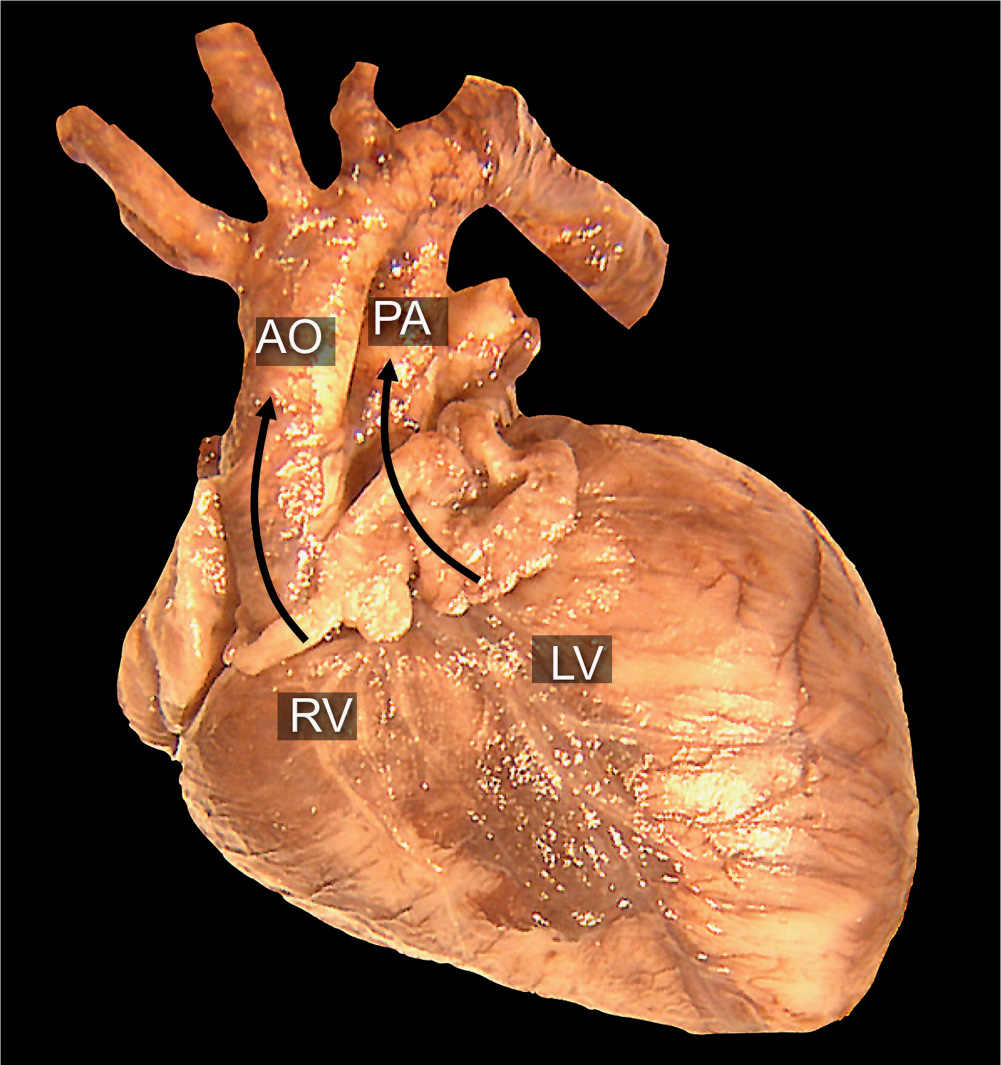
Figure 28.2: Anatomic specimen of a fetal heart with D-transposition of the great arteries. Note that the aorta (AO) is arising from the right ventricle (RV), anterior and parallel to the pulmonary artery (PA), which arises from the left ventricle (LV). Compare with an anatomic specimen of a normal heart in Figure 5.3.
Prenatal diagnosis of D-TGA is still a challenge. Prenatal screening policy for congenital heart disease, which primarily focuses on the four-chamber view alone, will undoubtedly fail in detecting TGA. Prenatal screening for congenital heart disease at a population level reports detection rates of 3% to 17% for simple TGA (3–5). The detection rate of TGA increased from 12.5% to 72.5% during a period of rapid progress and increased access to prenatal diagnosis in a population-based study (6). Given an associated decrease in neonatal morbidity and mortality in prenatally detected TGA (6–8), the assessment of the great vessels as part of the routine cardiac examination of the fetus is thus recommended, and, indeed, the inclusion of the outflow tracts was recently added to the national and international fetal cardiac screening guidelines (9, 10) (see also Chapter 2). Evidence also suggests that inclusion of the outflow tracts in screening guidelines has improved detection of TGA (8).
Ultrasound Findings
Gray Scale
The four-chamber view is typically normal in fetuses with D-TGA (Fig. 28.3A), except for an associated VSD. Visualization of the five-chamber view will show the pulmonary artery arising from the left ventricle and bifurcating, shortly after its origin, into two branches: right and left pulmonary arteries (Fig. 28.4A). The authors believe that the presence of bifurcation of the great vessel arising from the left ventricle is an important ultrasound clue to the presence of TGA. This clue may play a role in increasing prenatal detection of TGA given that the five-chamber view is now part of fetal cardiac screening (9, 10). In TGA, the aorta is noted to arise from the right ventricle in an anterior and parallel course to the pulmonary artery (Figs. 28.3 and 28.4). This parallel orientation of the great arteries in D-TGA is best obtained in an oblique plane of the heart, spatially oriented from the right shoulder to the left hip of the fetus (Figs. 28.3 and 28.5). A transverse view in the upper thorax will show in most cases, instead of the three-vessel-trachea view, a single large vessel (the transverse aortic arch) with a superior vena cava to its right (Figs. 28.4B and 28.6 to 28.8). The large vessel noted in the three-vessel-trachea view is the aorta, which is positioned anteriorly and superiorly to the pulmonary artery. It has also been described that the aorta assumes a right convex shape, also termed the I-sign, in cases of TGA at the three-vessel-trachea view (11, 12). The short-axis view at the level of the great vessels shows both the aorta and pulmonary artery as circular structures adjacent to each other instead of their normal orientation (longitudinal pulmonary artery wrapping around a circular aorta) (compare Fig. 28.6A with Fig. 8.8). On longitudinal views, the aortic arch is seen arising from the anterior right ventricle, giving rise to head and neck vessels and assuming a “hockey stick” orientation as it curves posteriorly. The pulmonary artery assumes the “candy cane” orientation in longitudinal views.
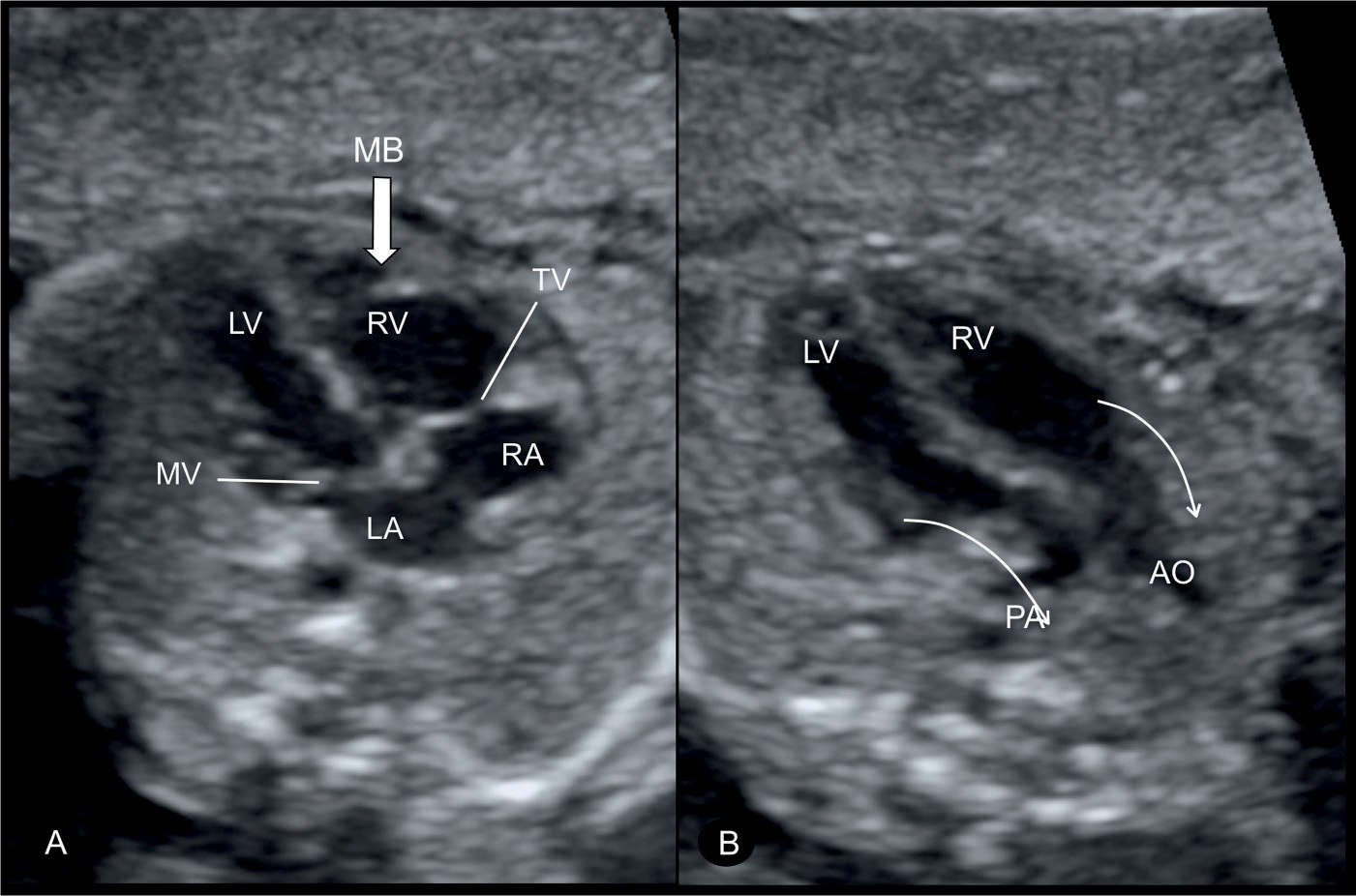
Figure 28.3: Four-chamber (A) and oblique (B) views of a fetus with complete transposition of the great arteries at 22 weeks’ gestation. Note in A, the normal appearing four-chamber view with atrioventricular concordance, normal insertion of the tricuspid (TV) and mitral (MV) valves, and the anatomic location of the moderator band (MB) (large arrow) at the apex of the right ventricle (RV) (compare with Fig. 28.17). In B, the pulmonary artery (PA) is seen to arise from the left ventricle (LV) and the aorta (AO) from the RV (arrows). LA, left atrium; RA, right atrium.
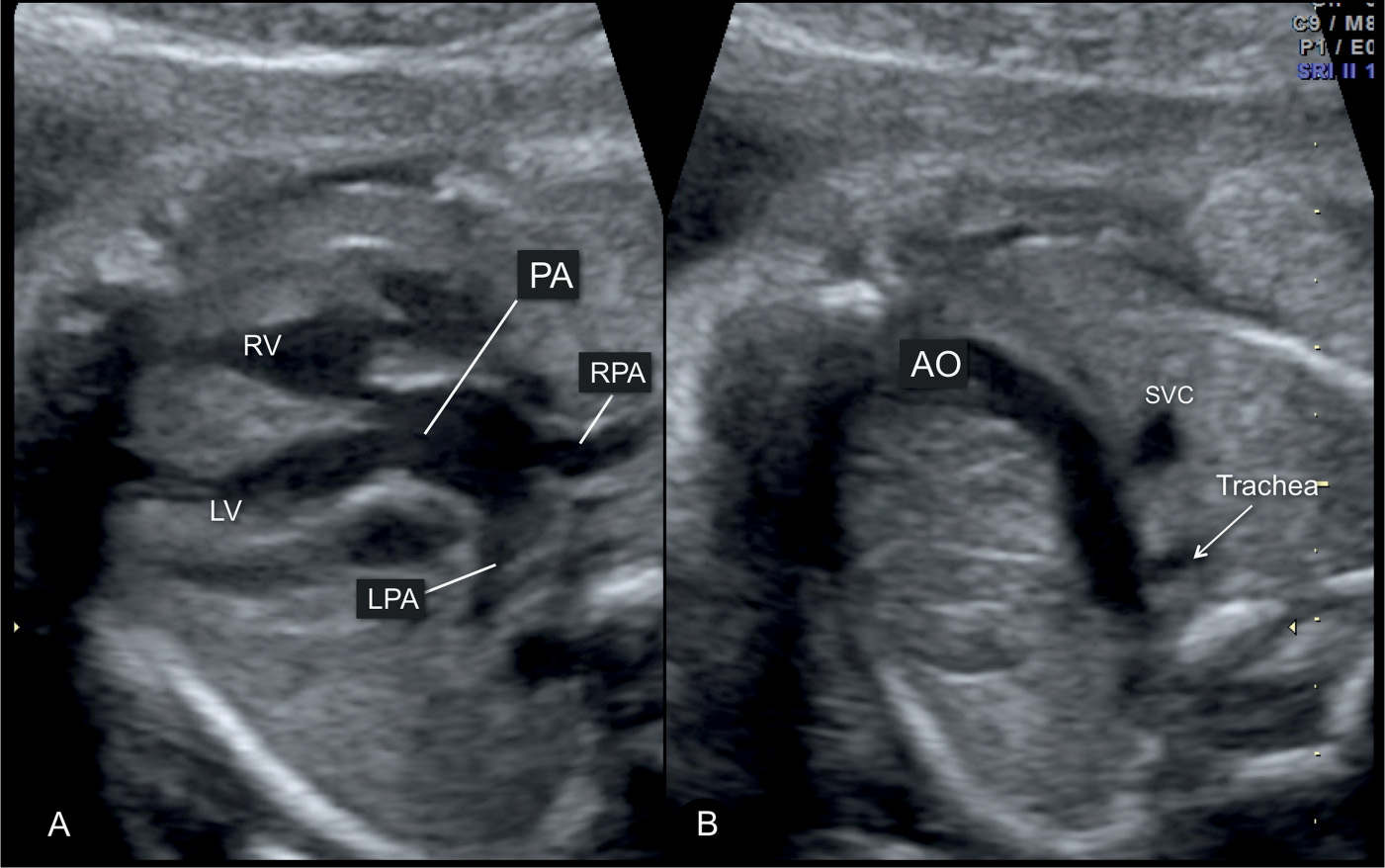
Figure 28.4: Five-chamber (A) and three-vessel-trachea (B) views of a fetus with complete transposition of the great arteries. In A, a slightly dilated pulmonary artery (PA) is seen to arise from the left ventricle (LV). Note in A, the bifurcation of the PA into the left (LPA) and right (RPA) pulmonary arteries. In B, two vessels are seen: the aorta (AO) and the superior vena cava (SVC) instead of the three vessels normally seen (AO, PA, and SVC). The pulmonary artery is not seen in B as it is posterior to the aortic isthmus at this level (see Fig. 28.6). Note that the aortic isthmus is not dilated and is slightly bent to the right. RV, right ventricle.
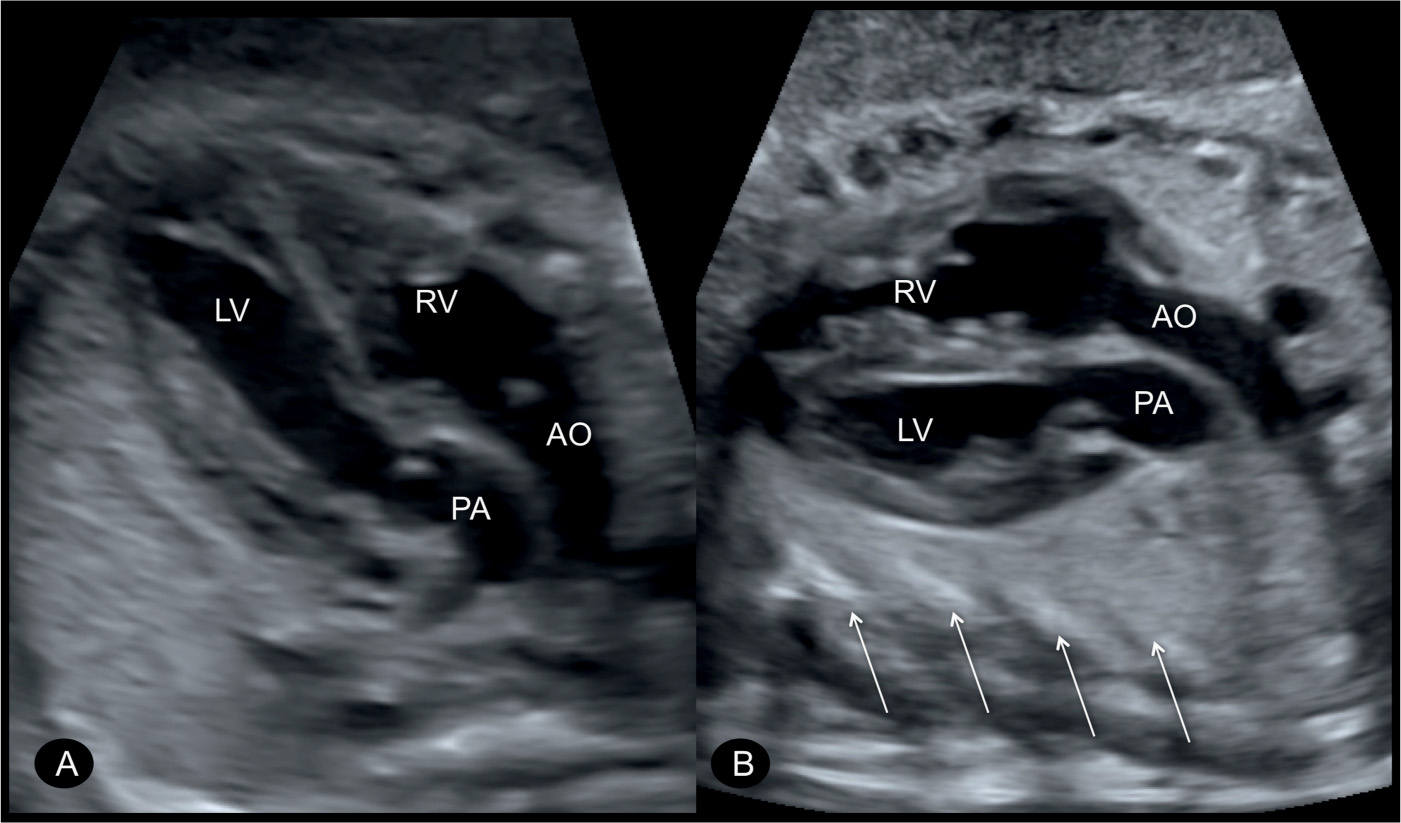
Figure 28.5: Parallel origin of the great vessels in two fetuses (A and B) with transposition of the great arteries shown in an oblique plane of the heart, spatially oriented from the right shoulder to the left hip of the fetus. The aorta (AO) arises more anteriorly from the right ventricle (RV) and is to the right of the pulmonary artery (PA), which arises from the left ventricle (LV). The oblique orientation of these planes is demonstrated by the cross section of ribs (arrows in B) in the outer perimeter of the chest.
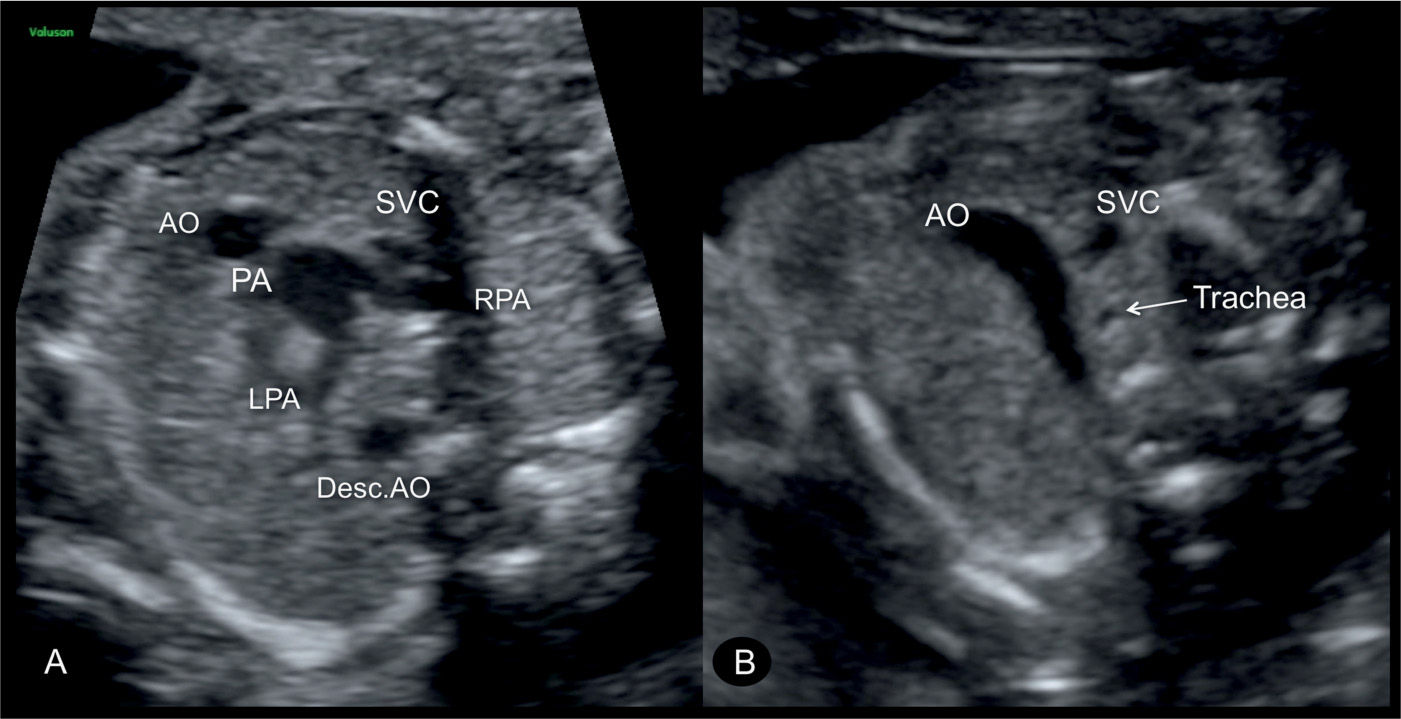
Figure 28.6: Inferior (A) and superior (B) short-axis views in a fetus with complete transposition of the great arteries. Note the presence of both great vessels in A in a cross-sectional orientation with the aorta (AO) anterior to the pulmonary artery (PA). The PA bifurcates into a right (RPA) and a left (LPA) pulmonary artery. In B, the anatomic location of the three-vessel-trachea view, the AO is seen as a single large, bent vessel. Desc.AO, descending aorta; SVC, superior vena cava.
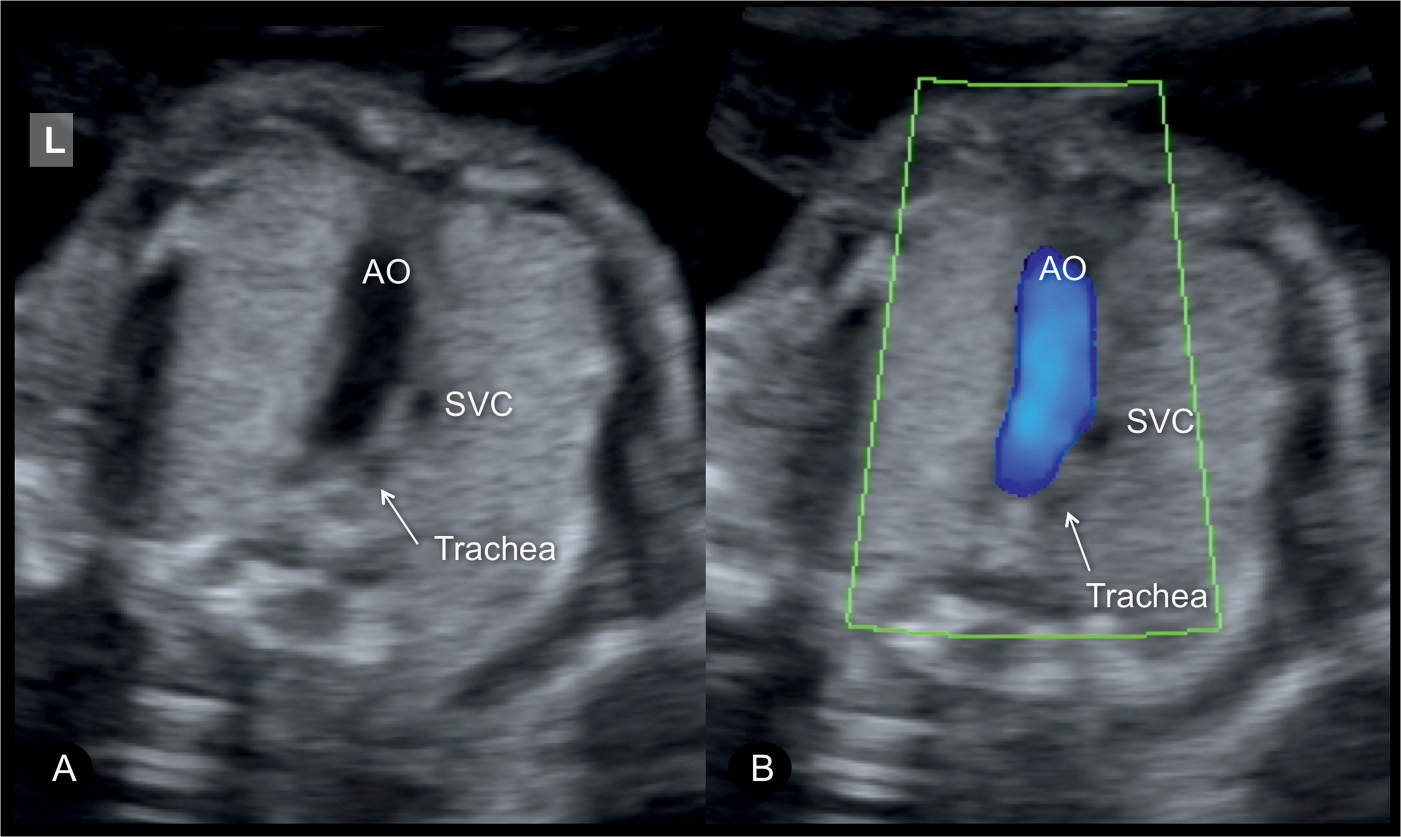
Figure 28.7: The three-vessel-trachea view in gray scale (A) and color Doppler (B) in a fetus with transposition of the great arteries demonstrating the aorta (AO) as a single large vessel with the superior vena cava (SVC) to its right. Color Doppler in B confirms antegrade flow in the AO. The pulmonary artery is generally located in an inferior position to the AO and thus is not visible in the three-vessel-trachea view. L, left.
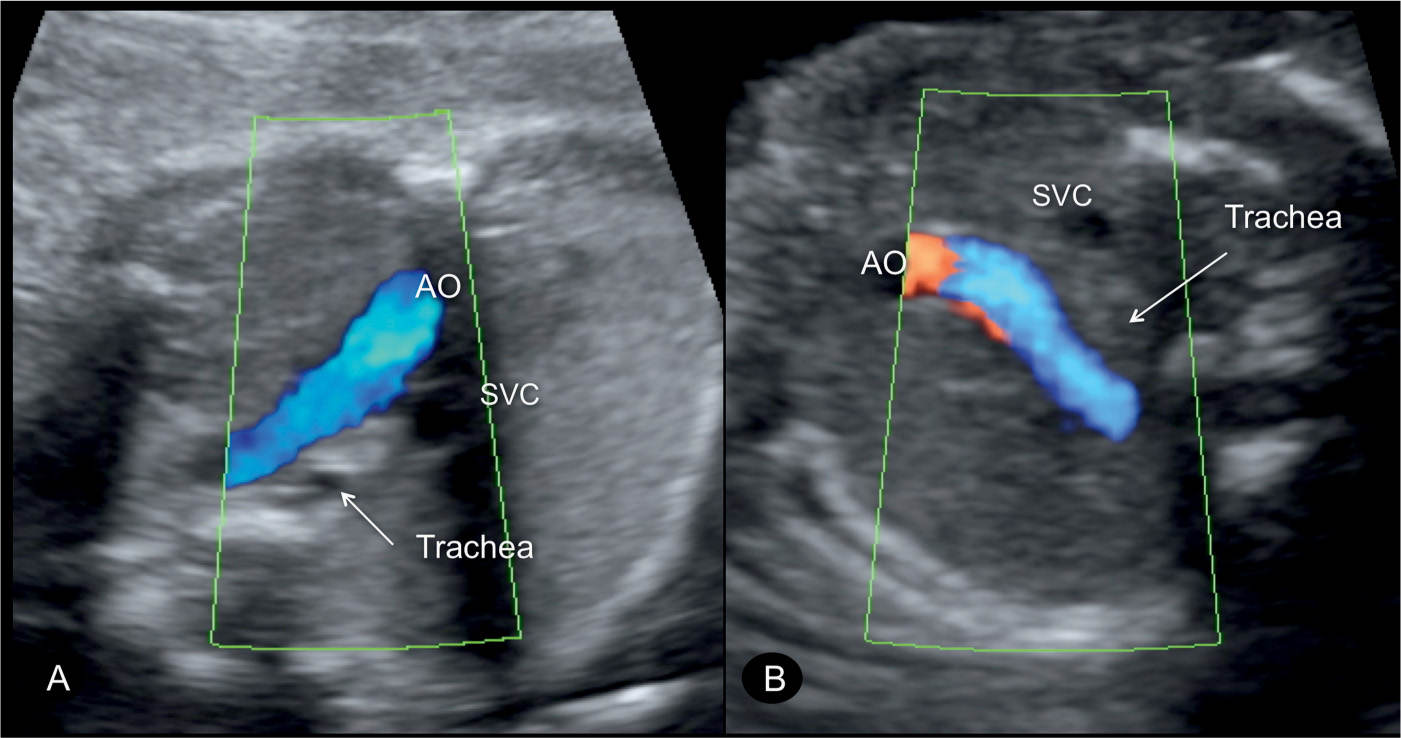
Figure 28.8: Three-vessel-trachea views in color Doppler in two fetuses (A and B) with transposition of the great arteries (TGA). Note the presence of the aortic arch (AO) as a single great vessel adjacent to the superior vena cava (SVC). The presence of the AO as a single great vessel in the three-vessel-trachea view is not specific for TGA, but can be present in other cardiac anomalies, such as in double outlet right ventricle.
Color Doppler
Color Doppler can be helpful in diagnosing D-TGA but is not necessary (13). Color Doppler helps in demonstrating the parallel course of the great vessels (Fig. 28.9). Visualization of an associated VSD (Figs. 28.9B and 28.10), confirming patency of the foramen ovale and assessing left ventricular outflow (pulmonary artery), can be enhanced by color Doppler. In early gestation, color Doppler is essential in demonstrating the crossing of the great vessels in normal conditions or their parallel course in D-TGA.
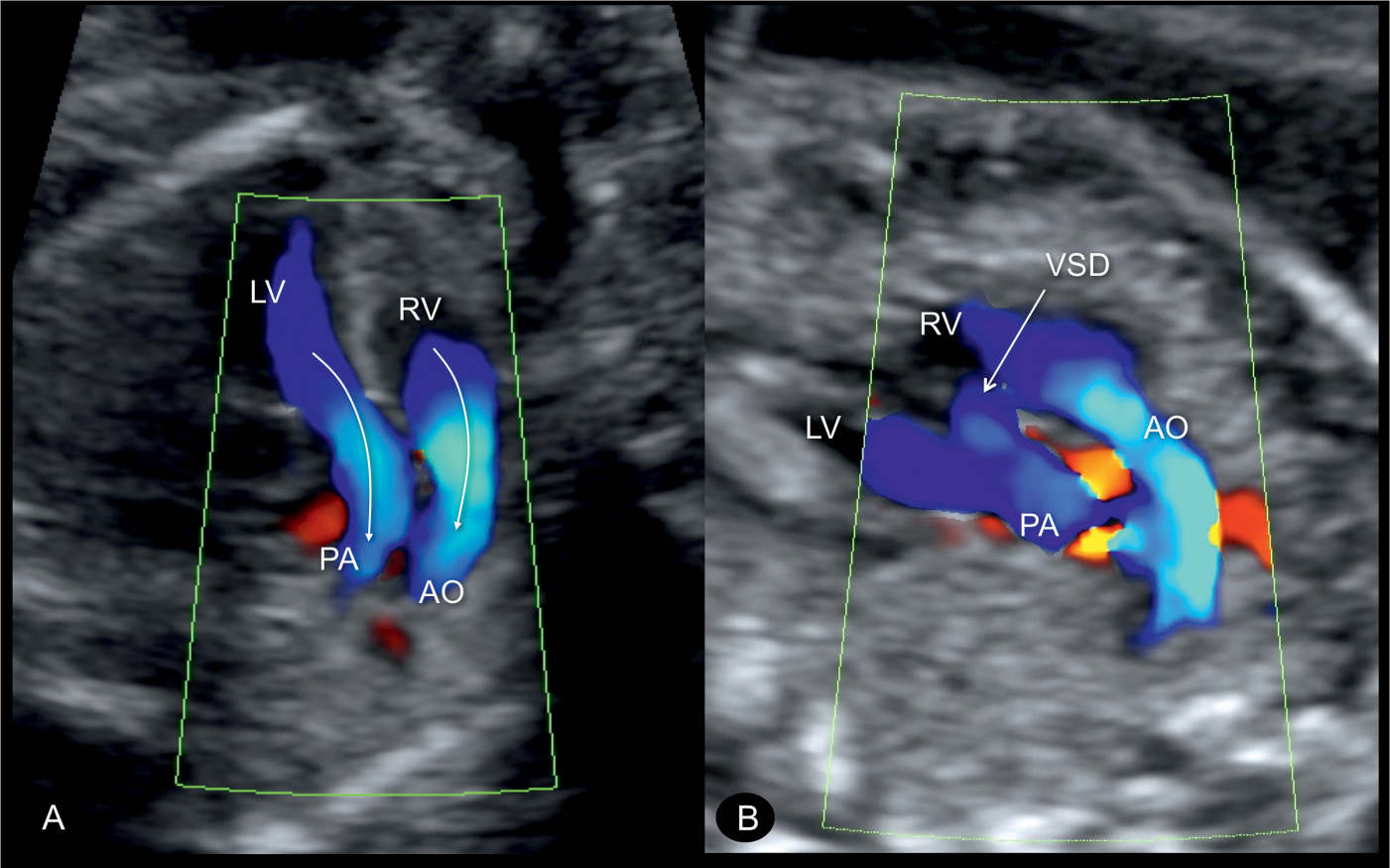
Figure 28.9: Oblique planes of the chest in color Doppler in two fetuses (A and B) with transposition of the great arteries demonstrating the parallel course of the great vessels with the aorta (AO) arising from the right ventricle (RV), anterior and parallel to the pulmonary artery (PA), which is arising from the left ventricle (LV) (arrows in A). In B, color Doppler confirms the presence of a ventricular septal defect (VSD).
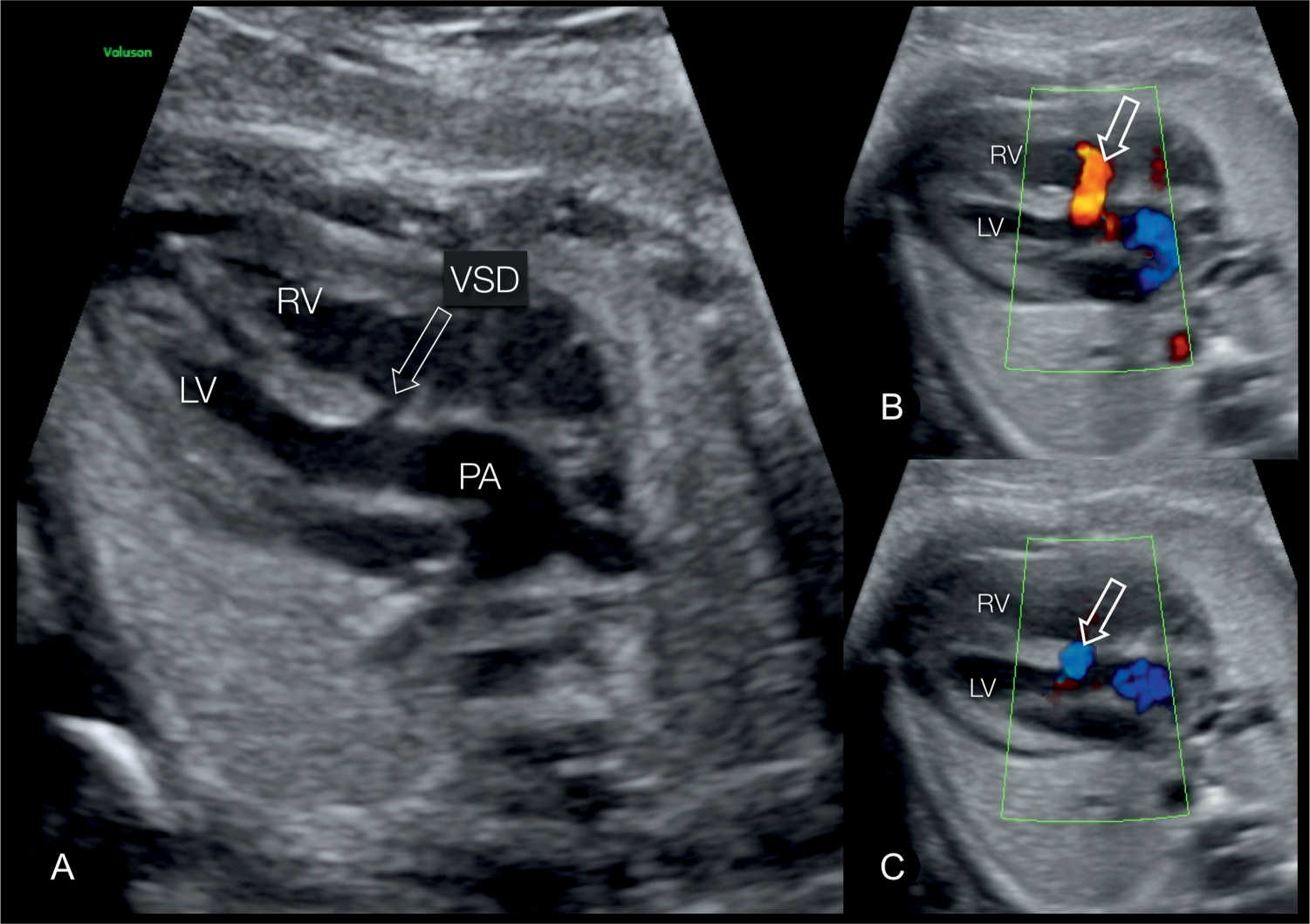
Figure 28.10: Five-chamber views in gray scale (A) and color Doppler (B and C) in a fetus with complete transposition of the great arteries and a ventricular septal defect (VSD) (open arrow). In A, the pulmonary artery (PA) is seen arising from the left ventricle (LV) and the VSD is seen. In B and C, color Doppler demonstrates the bidirectional shunting across the VSD. RV, right ventricle.
Early Gestation
D-TGA can be diagnosed at the 11- to 14-week ultrasound (Fig. 28.11), but its recognition is more difficult than in the second trimester, as reported in one series of targeted fetal echocardiography at 11 to 14 weeks where D-TGA was missed in most cases (14). An enlarged nuchal translucency in the setting of normal fetal chromosomes can be a marker for the presence of D-TGA (15). Recently, we reported on the strong association of abnormal cardiac axis and conotruncal anomalies, including TGA, in early gestation (16). The three-vessel-trachea view, with its finding of a single great vessel, may be helpful in early gestation as well (Fig. 28.11A). By rotating the transducer to view an oblique plane of the chest, the parallel course of the vessels can be demonstrated (Fig. 28.11B).
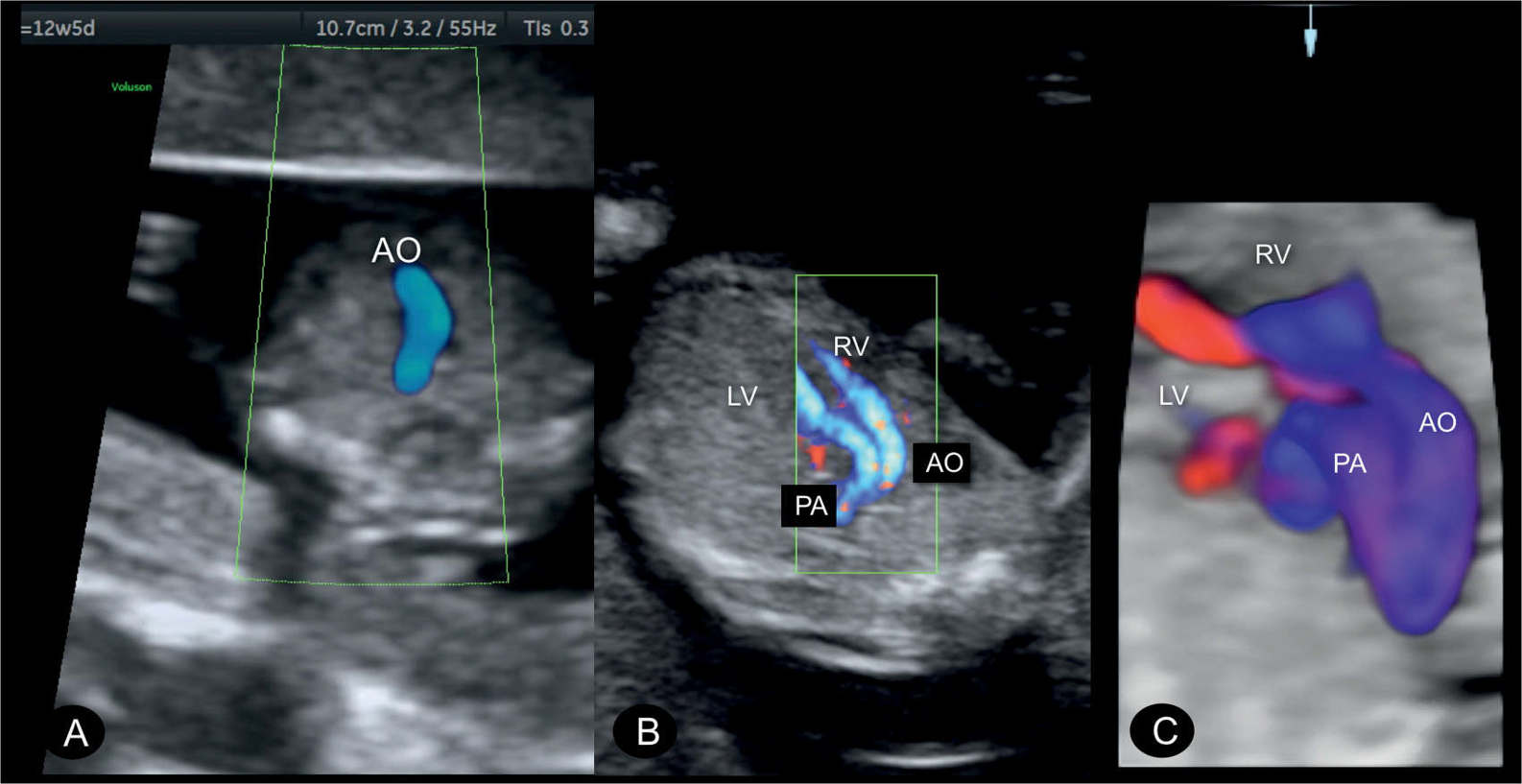
Figure 28.11: Transposition of the great arteries (D-TGA) in a fetus at 12 weeks’ gestation demonstrated in color Doppler at the three-vessel-trachea view (A) and an oblique view of the chest (B) and in 3D color Doppler with glass-body mode (C). Note in A the presence of a single great artery, the aorta (AO), as described in Figures 28.7 and 28.8. The parallel course of the great vessels arising in discordance from the right (RV) and left (LV) ventricles is demonstrated in B. C shows the spatial relationship of the great vessels, with the AO anterior and to the right of the pulmonary artery (PA).
Three-Dimensional Ultrasound
Various reports, focusing on rotations along different axes and color display of rendered volumes, emphasize the role of three-dimensional (3D) ultrasound in the diagnosis of D-TGA (17–20). Tomographic ultrasound imaging (Fig. 28.12), glass-body mode (Fig. 28.13), inversion mode (Fig. 28.14A), B-flow (Fig. 28.14B), and other 3D rendered displays have the ability to enhance visualization of the spatial relationship of the great vessels as they arise from their respective cardiac chambers. The use of the reconstructed en face view with color Doppler imaging of the four cardiac valves in 3D volumes of fetuses with TGA can demonstrate the different types of spatial relationships of the arterial trunks (Fig. 28.15), which may predict the likelihood of abnormal coronary arterial distribution (21). Evaluation of 3D automated software on volumes of fetuses with TGA demonstrated the abnormality in ventriculoarterial connections in all fetuses (22).
Associated Cardiac and Extracardiac Findings
VSDs and pulmonary stenosis (left ventricular outflow obstruction) are the two most common associated cardiac findings in D-TGA. VSDs are common and occur in about 40% of cases and are typically perimembranous but can be located anywhere in the septum (1). Pulmonary stenosis coexists with a VSD in D-TGA patients in about 30% of cases, and the stenosis is usually more severe and complex than in D-TGA with intact ventricular septum (1). Abnormal course and bifurcation of coronary arteries are found in patients with D-TGA, and its prevalence is more than 50% when the great vessels are side by side or when the aorta is posterior and to the right of the pulmonary artery (23, 24). Other associated cardiac anomalies are rare and can involve the atrioventricular valves, the aortic arch, and great vessels.
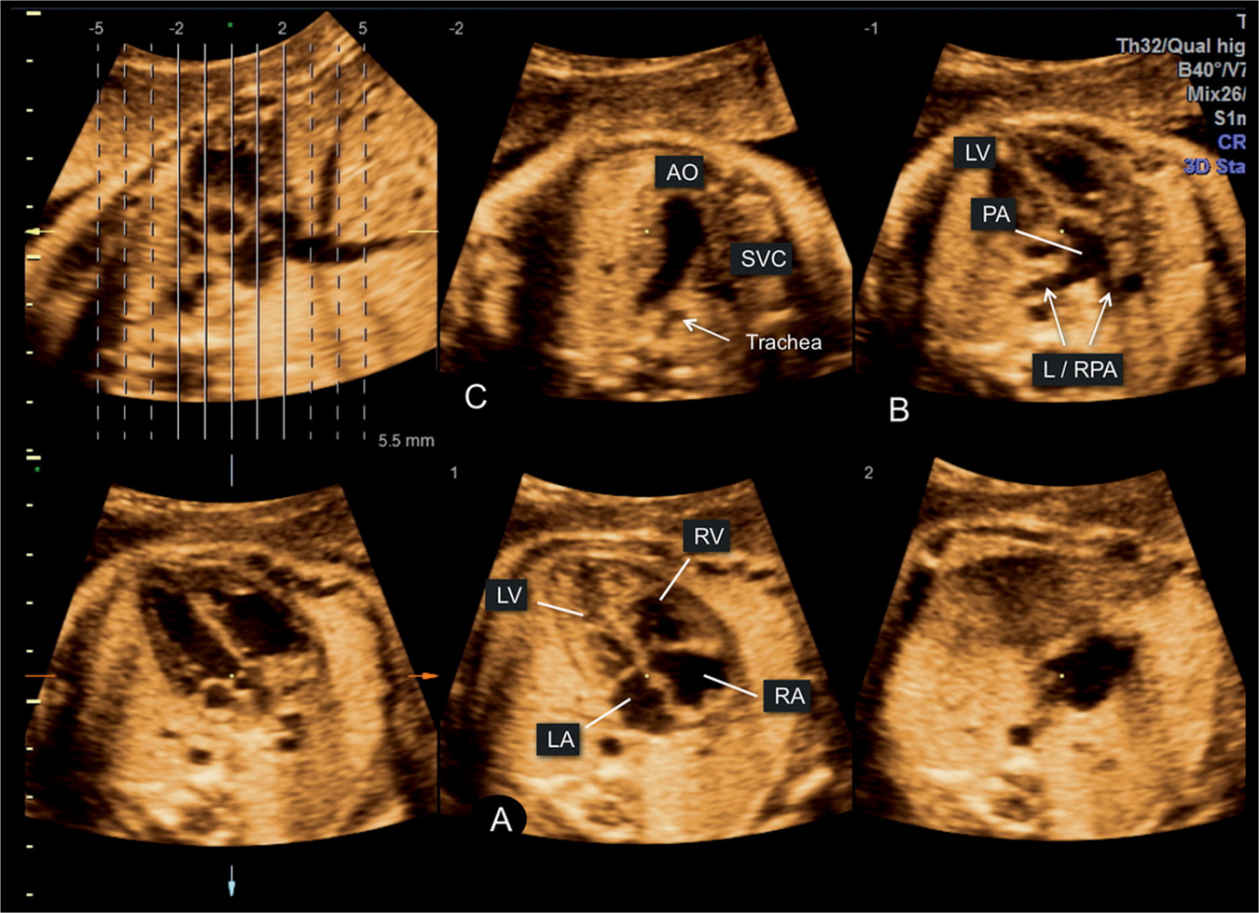
Figure 28.12: Tomographic mode display of a 3D spatiotemporal image correlation (STIC) volume in a fetus with complete transposition of the great arteries. This tomographic display demonstrates several findings, such as (1) normal four-chamber view in A, (2) pulmonary artery (PA) arising from the left ventricle (LV) with its bifurcation into left and right pulmonary arteries (L/RPA) in B, and (3) aortic arch (AO) as a single large great vessel in the upper mediastinum in C. See Figures 28.3, 28.4, and 28.7 for comparison. LA, left atrium; RA, right atrium; RV, right ventricle; SVC, superior vena cava.
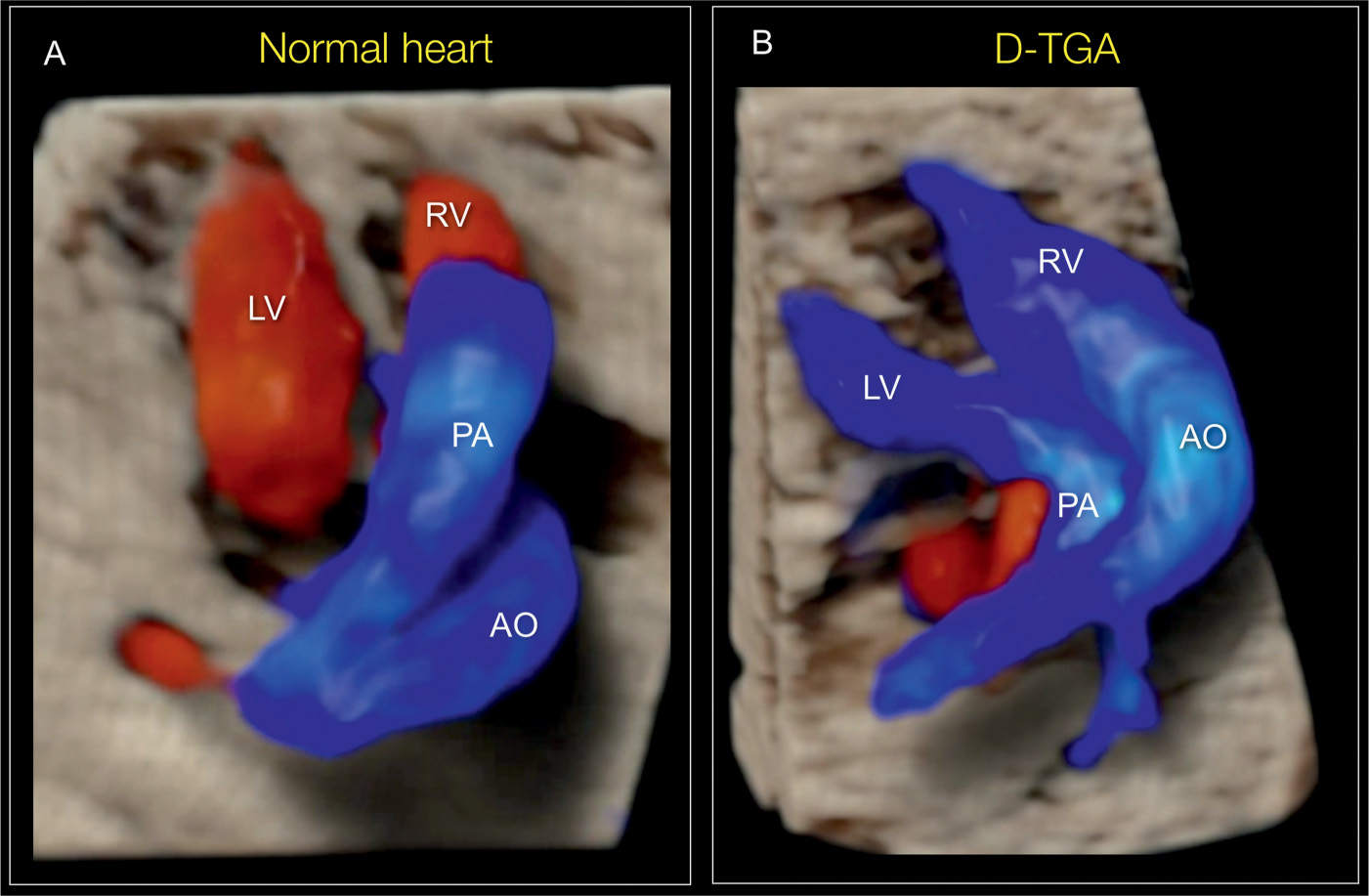
Figure 28.13: Glass-body mode rendering of a cranial view of the great vessels in a normal fetus (A) and in a fetus with transposition of the great arteries (B). The normal great vessel crossing in A and their parallel course in B are clearly demonstrated. AO, aorta; PA, pulmonary artery; LV, left ventricle; RV, right ventricle.
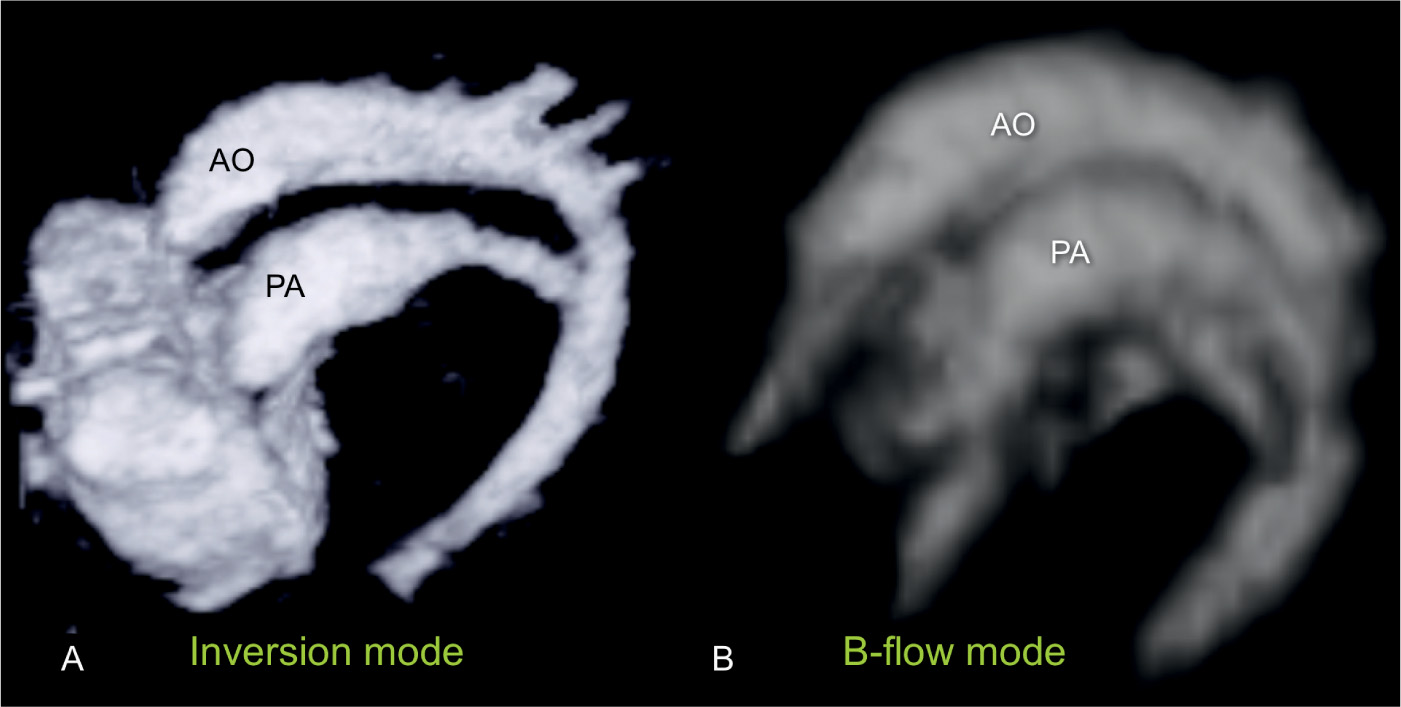
Figure 28.14: 3D volumes showing longitudinal views of the great vessels from the left side in two fetuses with complete transposition of the great vessels. A is obtained from a 3D static volume rendered in inversion mode, and B is obtained from a B-flow spatiotemporal image correlation (STIC) volume. Both planes (A and B) clearly demonstrate the parallel course of the great vessels. PA, pulmonary artery; AO, aorta.
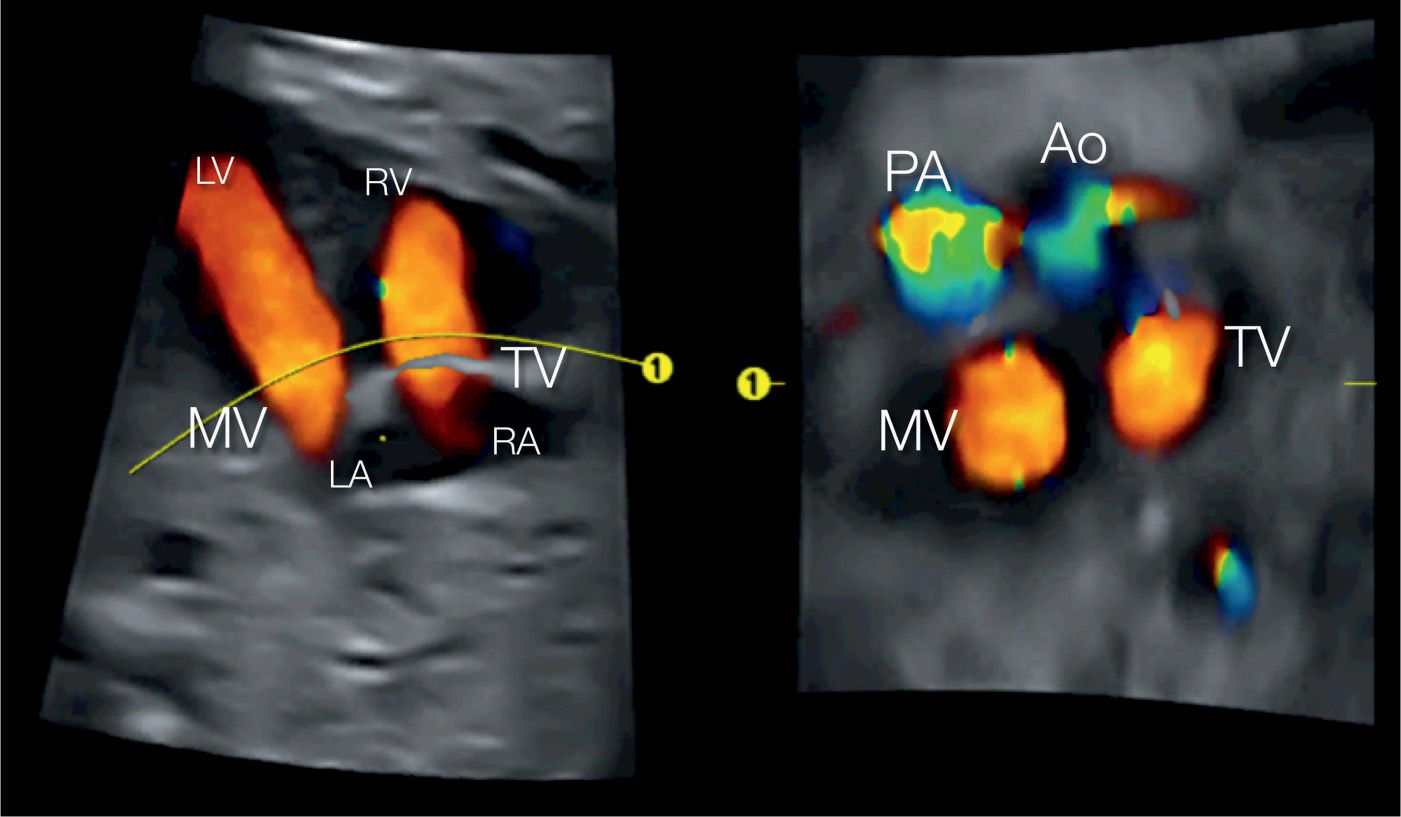
Figure 28.15: 3D volume in color Doppler from a spatiotemporal image correlation (STIC) acquisition obtained at the level of the four-chamber view (A). B is retrieved from the 3D volume at the base of the heart showing in color Doppler the atrioventricular and semilunar valves. Perfusion across the mitral (MV) and tricuspid (TV) valves is seen in red (B). Also, note in B, the side-by-side arrangements of the great arteries in a D-transposition orientation. Ao, aorta; LA, left atrium; LV, left ventricle; PA, pulmonary artery; RA, right atrium; RV, right ventricle.
Extracardiac anomalies may be present but rare, and numerical chromosomal aberrations are practically absent in D-TGA. Microdeletion of 22q11 could be present and should be ruled out, especially when extracardiac malformations or a complex D-TGA is present. Situs abnormalities can be present, such as abdominal situs inversus, and depending on the venoatrial connection, a balanced circulation may be found. Among the few associated extracardiac anomalies in D-TGA, the authors report one ear anomaly, one cleft lip, and one wide cleft lip and palate.
Differential Diagnosis
Double outlet right ventricle and corrected TGA are the two most common cardiac anomalies in the differential diagnosis of D-TGA as they all share the absence of “crossover” of the great vessels (25). Differentiating D-TGA from congenitally corrected TGA (cc-TGA) is explained in the next section.
False-positive diagnosis of TGA may occur at the level of the three-vessel-trachea view if the novice examiner assumes a parallel course of the vessels as they are imaged side by side at this level. The display of a parallel course of the great vessels in the diagnosis of TGA should include the ventricles, the semilunar valves, and the ventricular septum separating the great vessels.
Prognosis and Outcome
D-TGA is well tolerated in utero. Prenatal follow-up examination with color Doppler should focus on the presence or absence of a VSD and on the subsequent development of pulmonary stenosis, which is not commonly detected in the second trimester. Furthermore, flow assessment with color and spectral Doppler, at the level of the foramen ovale and ductus arteriosus, should be given close attention closer to term. Premature closure or narrowing of the foramen ovale and/or the ductus arteriosus is associated with worsening neonatal outcome and may require emergency postnatal procedures (26, 27).
Prognosis of a neonate with D-TGA is excellent provided the child is born at a tertiary institution with pediatric cardiology intensive services (3, 7). Prenatal detection of D-TGA and/or neonatal treatment before cyanosis appears to improve outcome (3, 7). In a study of 144 cases of TGA with a one-year follow-up, first-year mortality and presurgical mortality were significantly lower in cases with prenatal diagnosis (8). Closure of the duct before treatment, renal dysfunction and hypoxia occurred significantly more often in the group without prenatal diagnosis (8).
Prostaglandin infusion to maintain patency of the ductus arteriosus and a balloon atrial septostomy is usually required in order to enhance oxygenation and preparation for corrective surgery. An emergency balloon septostomy may be required within hours after birth in some cases of obstructed foramen flow, hence the importance of delivery at a center equipped to perform these procedures (7, 26, 27). Corrective surgery currently involves an arterial switch operation, where the aorta and pulmonary artery are transacted above the semilunar valves and switched with reimplantation of the coronary circulation.
KEY POINTS  Complete Transposition of the Great Arteries
Complete Transposition of the Great Arteries
 There is atrioventricular concordance and ventriculoarterial discordance in D-TGA.
There is atrioventricular concordance and ventriculoarterial discordance in D-TGA.
 In D-TGA, both great arteries display a parallel course, with the aorta more commonly anterior and to the right of the pulmonary artery.
In D-TGA, both great arteries display a parallel course, with the aorta more commonly anterior and to the right of the pulmonary artery.
 The four-chamber view is typically normal in fetuses with D-TGA, except for an associated VSD.
The four-chamber view is typically normal in fetuses with D-TGA, except for an associated VSD.
 Visualization of the five-chamber view in D-TGA will show the pulmonary artery arising from the left ventricle and bifurcating, shortly after its origin, into two branches: right and left pulmonary arteries.
Visualization of the five-chamber view in D-TGA will show the pulmonary artery arising from the left ventricle and bifurcating, shortly after its origin, into two branches: right and left pulmonary arteries.
 In D-TGA, the three-vessel-trachea view will demonstrate, in most cases, a single large vessel (aorta) with a superior vena cava to its right.
In D-TGA, the three-vessel-trachea view will demonstrate, in most cases, a single large vessel (aorta) with a superior vena cava to its right.
 The short-axis view at the level of the great vessels in D-TGA shows both the aorta and pulmonary artery as circular structures adjacent to each other.
The short-axis view at the level of the great vessels in D-TGA shows both the aorta and pulmonary artery as circular structures adjacent to each other.
 VSDs and pulmonary stenosis are the two most common associated cardiac findings with D-TGA.
VSDs and pulmonary stenosis are the two most common associated cardiac findings with D-TGA.
 VSDs occur in about 40% of D-TGA cases and are typically perimembranous.
VSDs occur in about 40% of D-TGA cases and are typically perimembranous.
 Pulmonary stenosis coexists with a VSD in about 30% of D-TGA cases.
Pulmonary stenosis coexists with a VSD in about 30% of D-TGA cases.
 Extracardiac anomalies may be present in D-TGA but rare, and numerical chromosomal aberrations are practically absent.
Extracardiac anomalies may be present in D-TGA but rare, and numerical chromosomal aberrations are practically absent.
 Premature closure or narrowing of the foramen ovale and/or the ductus arteriosus in D-TGA is associated with worsening neonatal outcome and may require emergency postnatal procedures.
Premature closure or narrowing of the foramen ovale and/or the ductus arteriosus in D-TGA is associated with worsening neonatal outcome and may require emergency postnatal procedures.
 Prognosis of D-TGA is excellent when detected prenatally and the child is born at a tertiary center.
Prognosis of D-TGA is excellent when detected prenatally and the child is born at a tertiary center.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


