● INTRODUCTION
The sonographic assessment of the fetal venous system has seen significant advances over the past 20 years, since the pioneering work on the ductus venosus (DV) by Kiserud et al. (1). The development of high-resolution ultrasound transducers, the common use of color Doppler, and the advent of power Doppler (see Chapter 12) were important steps, which facilitated the comprehensive study of the venous system in the fetus. Normal and abnormal anatomy of the fetal venous system were described and reported in 2D and 3D ultrasonography (2–9). We hereby provide a comprehensive description of the fetal venous system and report a simplified systematic approach for the evaluation of the course and connection of the veins in and around the fetal heart (7). An overview of the pulsed Doppler patterns of the fetal venous system is presented in Chapter 13.
● ANATOMY OF THE VENOUS SYSTEM
From an embryologic point of view, the central systemic venous system evolves from a symmetrical system with bilateral vitelline, umbilical and cardinal veins, to an asymmetrical, mainly right-sided system, where the left-sided veins bridge to drain into the large right-sided veins that connect to the heart (5) (see also Chapter 3). In the upper body, above the diaphragm, the left jugular vein connects via the brachiocephalic (or innominate) vein to the right superior vena cava (SVC) (5) (see Fig. 5.19); and in the lower body, below the diaphragm, the portal system, hepatic veins, and DV join the inferior vena cava (IVC) (5). The SVC and IVC drain into the right atrium. In this chapter, we present a detailed review of the fetal systemic and pulmonary venous systems, including the umbilical vein (UV), the DV, the portal veins, the hepatic veins, the IVC and SVC, the azygos vein, the pulmonary veins, the coronary sinus (CS), and the left brachiocephalic vein (Fig. 10.1).
● PROPOSED PLANES FOR THE EVALUATION OF THE FETAL VENOUS SYSTEM
Standardized ultrasound planes, such as the axial view of the fetal abdomen, the four-chamber view, and views of the great vessels, are used in fetal, infant, and adult echocardiography (see Chapters 5–8) and are primarily dedicated to the evaluation of the anatomy of the heart and great vessels. We have recently proposed a systematic approach for the comprehensive evaluation of the fetal venous system (7). This approach includes six planes (axial, oblique, and parasagittal) of the fetal abdomen and chest, which allows for the demonstration of the fetal central venous system in a step-by-step fashion (7). Color Doppler enhances visualization, and the occasional use of 3D ultrasound allows for better demonstration of the spatial anatomic course of the veins (3, 4). The six standardized planes are described in more detail in the following sections of this chapter.
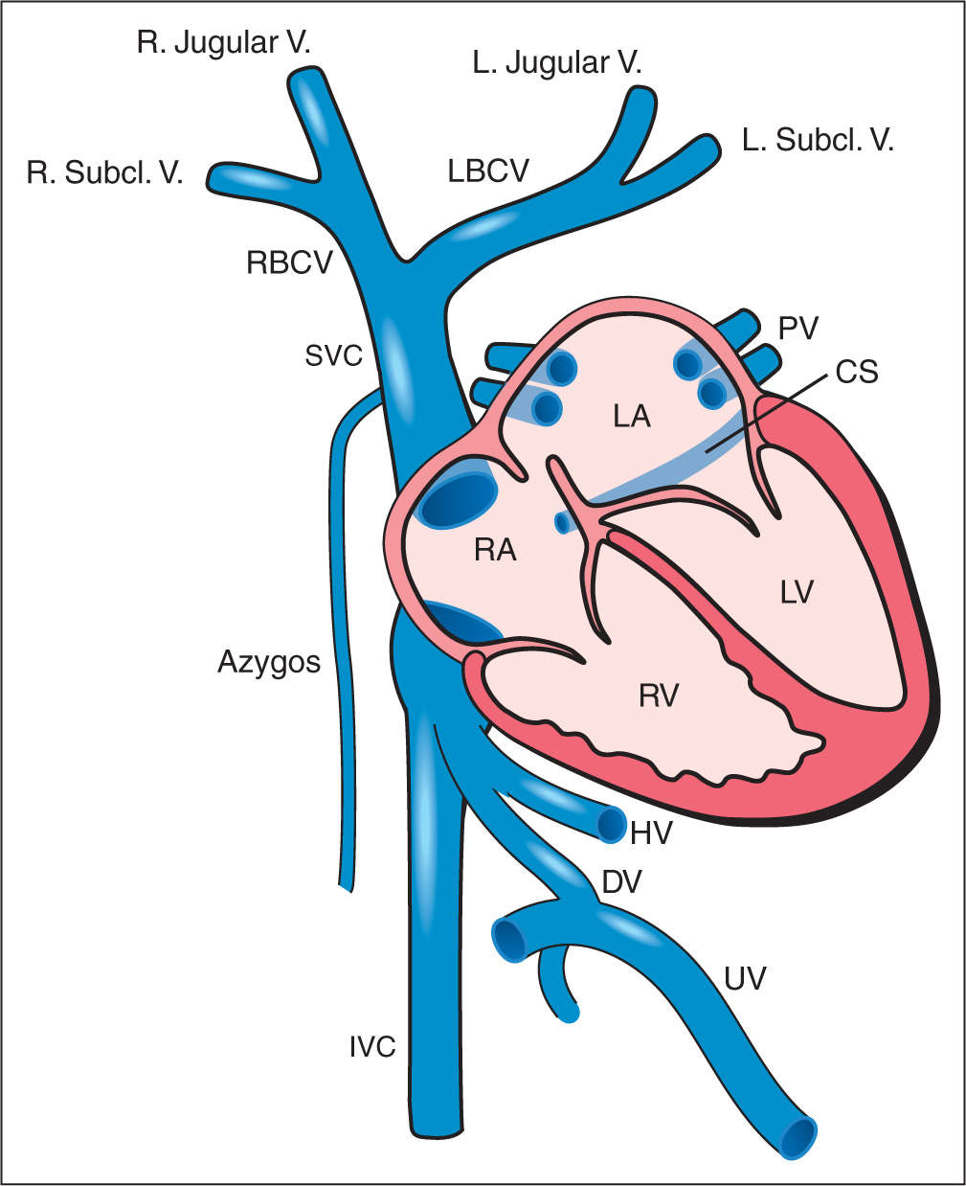
Figure 10.1: Schematic drawing of the fetal central venous system at the level of the heart. Note that the superior (SVC) and inferior (IVC) venae cavae, the pulmonary veins (PV), and the coronary sinus (CS) drain directly into the heart. The SVC is formed by the fusion of the right (RBCV) and left (LBCV) brachiocephalic veins and the azygos vein. The RBCV and LBCV are formed by the fusion of the corresponding right (R. Jugular V.) and left (L. Jugular V.) jugular veins and by the right (R. Subcl. V.) and left (L. Subcl. V.) subclavian veins. The IVC receives venous drainage from the hepatic and portal systems. See text for details. RA, right atrium; LA, left atrium; DV, ductus venosus; HV, left hepatic vein; UV, umbilical vein; RV, right ventricle; LV, left ventricle.
Plane 1: The Axial Abdominal View
The first of the six planes is an axial plane that is obtained at the level of the abdominal circumference. This plane, with slight tilting and angulation, allows for the evaluation of the abdominal venous vasculature, including the IVC, the hepatic veins, the DV, and the umbilical–portal system. The ultrasonographic plane of the upper abdomen, at the level of the abdominal circumference, was described in Chapter 6. In this chapter, we expand on the anatomy of the venous system as it relates to the six standardized planes.
The Inferior Vena Cava
Anatomy. The right and left common iliac veins join in the pelvis to form the IVC, which continues in the abdomen in a course that is right and anterior to the spine and aorta. The IVC receives the right and left renal veins at the level of the kidneys. As the IVC reaches the liver, its course changes slightly to a more ventral position along the posterior surface of the liver. The IVC then enters the right atrium along its posterior wall.
Visualization. The course and the position of the IVC can be assessed by a series of axial parallel planes of the pelvis and abdomen, demonstrating the side-by-side anatomic location of the IVC and aorta in the pelvis (Fig. 10.2) and an IVC that is anterior and to the right of the aorta in the upper abdomen (Fig. 10.3). An axial view of the fetal abdomen, just below the diaphragm can identify the infracardiac portion of the IVC, with its confluence with the DV and three main hepatic veins into a vascular space called the subdiaphragmatic vestibulum (10) (Fig. 10.4A,B). At the level of the diaphragm, the entry of the vestibulum into the right atrium is visualized. This axial approach in the evaluation of the IVC is optimal for the assessment of vessel diameter and relationship with neighboring veins. For color and pulsed Doppler evaluation of the IVC, a parasagittal view is preferred (Fig. 10.5).
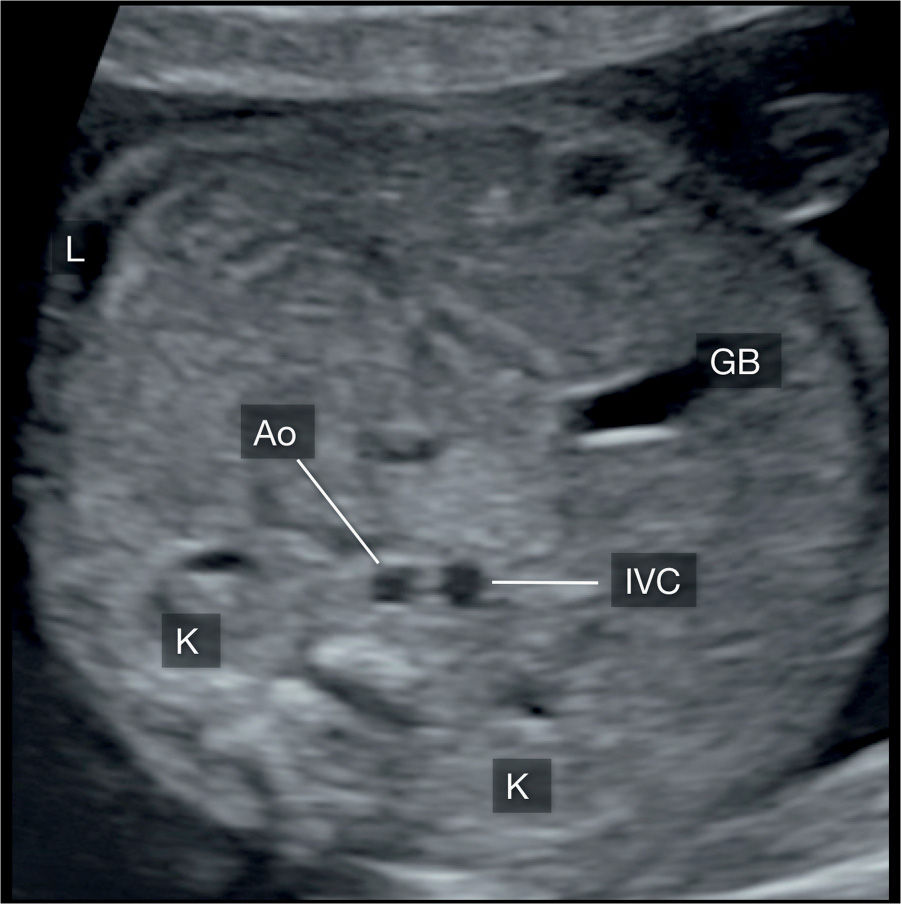
Figure 10.2: Axial view of the fetal lower abdomen, showing the anatomic location of the inferior vena cava (IVC) and its relationship to the descending aorta (Ao). At this level, the IVC is located in the posterior abdomen, in a side-by-side and slightly anterior, anatomic relationship to the Ao. K, kidney; GB, gallbladder; L, left.
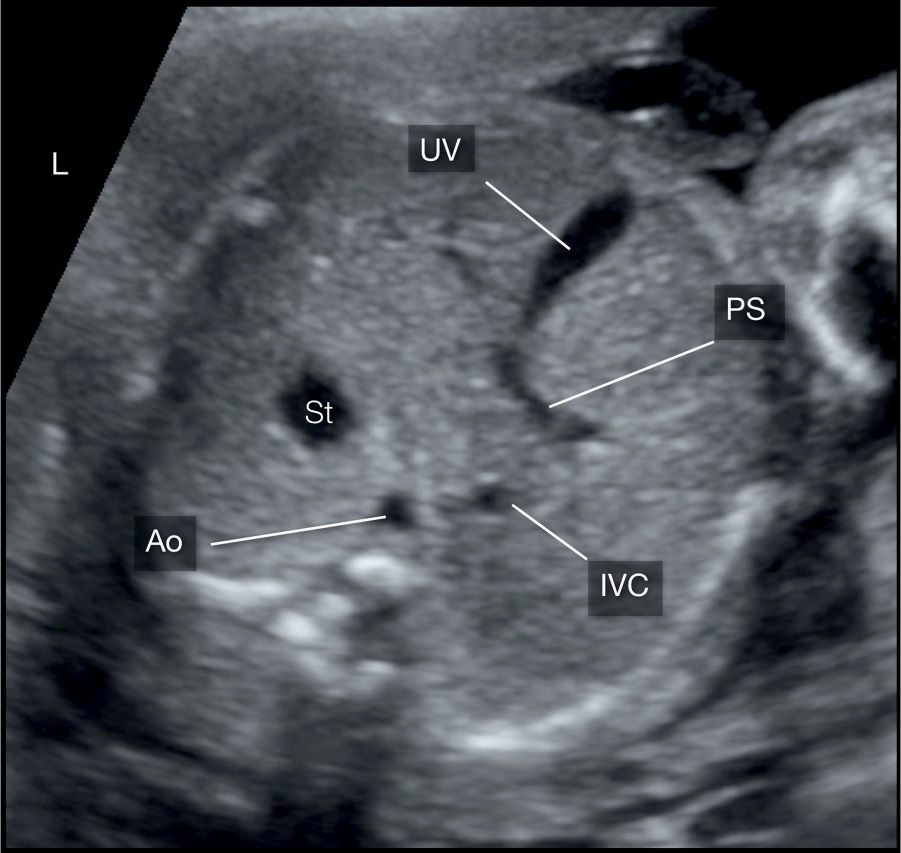
Figure 10.3: Axial view of the fetal upper abdomen, showing the anatomic location of the inferior vena cava (IVC) and its relationship to the descending aorta (Ao). At this level, the IVC is located anterior and to the right of the aorta. The umbilical vein (UV) can be recognized draining into the portal sinus (PS). St, stomach; L, left.
The Hepatic Veins
Anatomy. The hepatic veins are the intrinsic veins of the liver and drain blood from the liver parenchyma to the heart. Veins from the left and right fetal hepatic lobes converge into three main hepatic veins: left, medial, and right hepatic veins (11). These three veins converge into the vascular space of the subdiaphragmatic vestibulum (Fig. 10.4) where the DV empties as well.
Visualization. A slightly oblique plane of the abdomen at the level of the liver, pointing toward the left shoulder, is best for the visualization of the three hepatic veins. All three hepatic veins are visualized in a trident as they merge toward the IVC (Fig. 10.4). In this plane, the DV is often visualized joining the vestibulum in a course between the left and the middle hepatic veins. The demonstration of the hepatic veins on ultrasound is facilitated by color Doppler, with a low-velocity scale, lower than that is typically needed for imaging the IVC or DV.
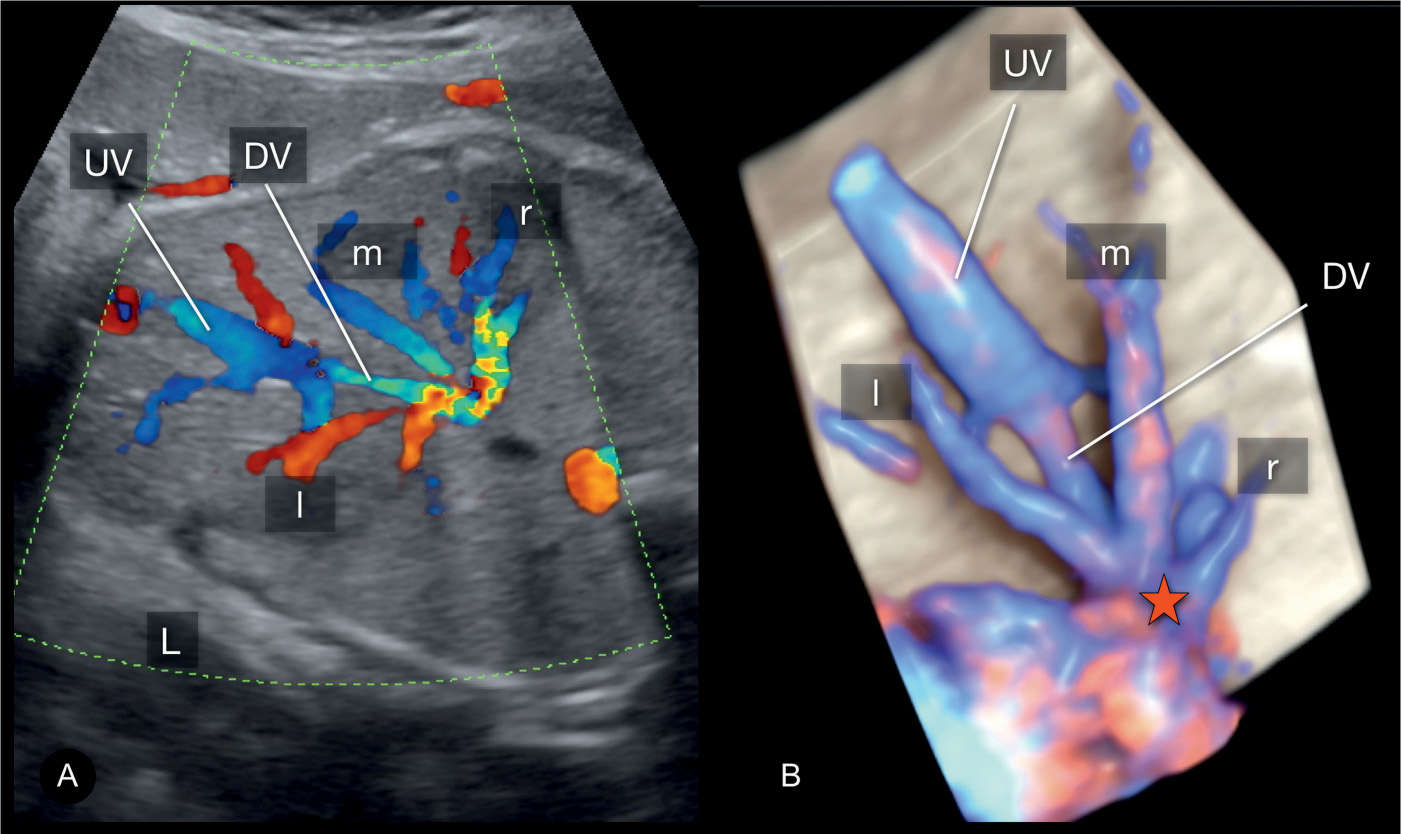
Figure 10.4: Oblique view of the fetal abdomen in color Doppler (A) and in 3D high-definition color (B), showing the course of the umbilical vein (UV) across the liver with its junction with the ductus venosus (DV). The DV along with the left (l), middle (m), and right (r) hepatic veins join the inferior vena cava (IVC) into the subdiaphragmatic vestibulum (star) and then into the right atrium (compare with Fig. 10.1). L, left.
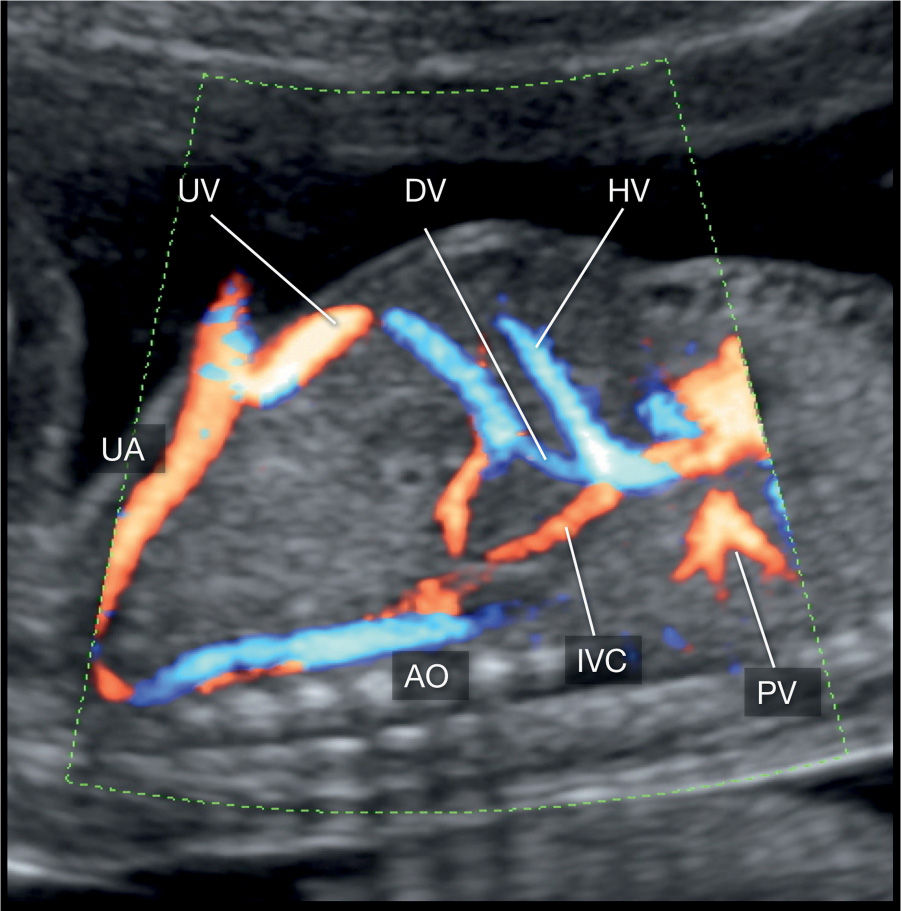
Figure 10.5: A parasagittal view of the chest and abdomen, showing the inferior vena cava (IVC) in a longitudinal view. This view is helpful for color and pulsed Doppler evaluation of the IVC. DV, ductus venosus; HV, hepatic vein; PV, pulmonary veins; UV, umbilical vein; UA, umbilical artery; AO, descending aorta.
The Ductus Venosus
Anatomy. The DV is a thin hourglass-shaped fetal vessel that connects the UV to the heart (1). It arises from the portal sinus at the site of the termination of the UV, ascends in a groove between the left and caudate lobes of the liver, and joins with the IVC subdiaphragmatic vestibulum. The DV, in contrast to previous assumption, does not mix blood with the IVC. Its anatomic size and orientation is such that the oxygen-rich blood within the DV is accelerated and directed straight across the foramen ovale and into the left atrium (12). Highly oxygenated blood from the placenta and UV is thus directed into the left atrium, ventricle, and ascending aorta, bringing high oxygen content to the coronary and cerebral circulations.
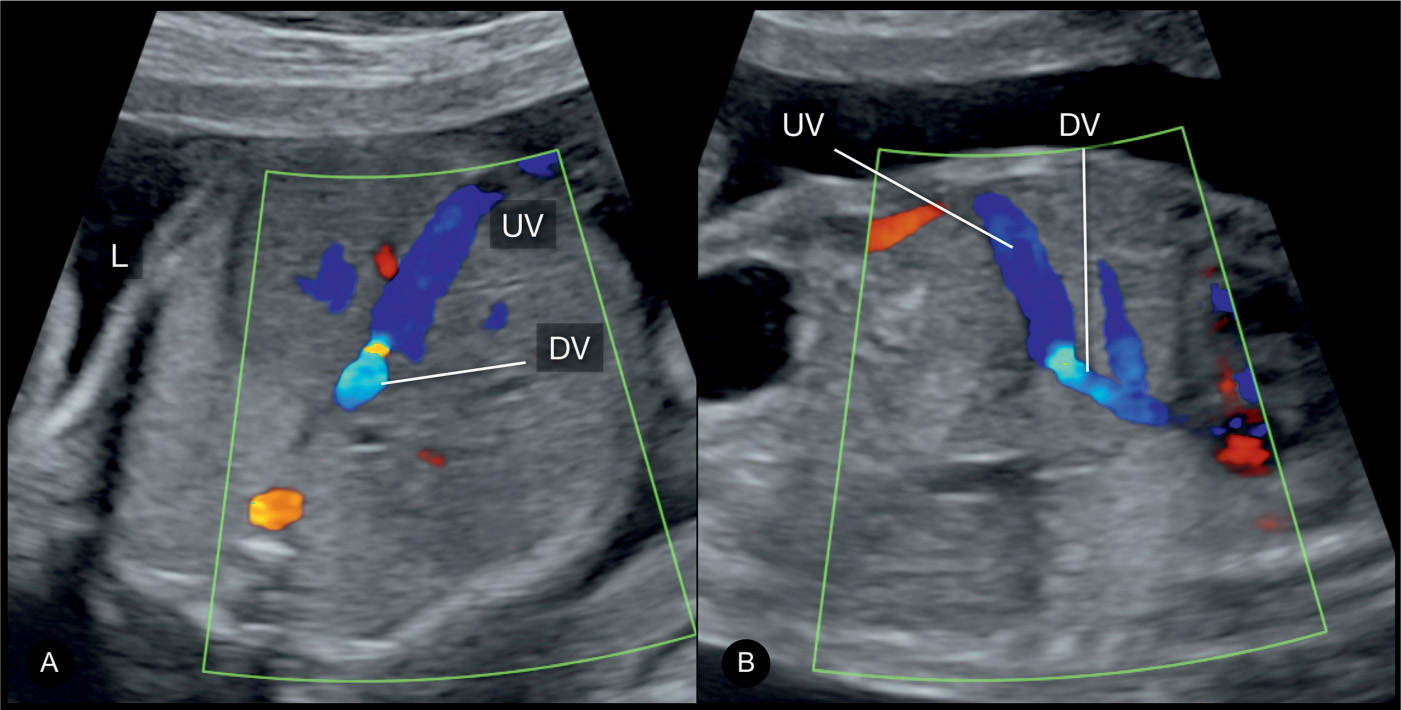
Figure 10.6: Axial/oblique (A) and parasagittal (B) planes of the fetal abdomen in color Doppler, showing the umbilical vein (UV) and the ductus venosus (DV). Note the narrow size of the DV in A and B, and the presence of aliasing on color Doppler, an important feature that helps in its recognition. In B, the parasagittal plane shows the DV in longitudinal view and is preferred in early gestation. See text for details. L, left.
Visualization. The DV can be visualized in an axial plane of the upper abdomen (Figs. 10.4A and 10.6A). From the axial plane at the level of the abdominal circumference, slight inclination toward the upper chest, shows the DV as a narrow vessel arising from the UV (Fig. 10.6A). The DV can also be seen in a midsagittal longitudinal view of the abdomen (Figs. 10.5 and 10.6B). In this approach, which is preferred in early gestation, the junction between the DV and the UV is seen and the narrow size of the DV is appreciated (Fig. 10.6B). Due to its narrow and short size, visualization of the DV is facilitated by the use of color Doppler, which reveals the presence of color aliasing, an important feature that helps in the identification of DV (Fig. 10.6A,B).
The Umbilical–Portal System
Anatomy. The vascular anatomy of the umbilical and portal venous systems in the fetus is difficult to understand, especially due to small vasculature, the presence of normal anatomic variations, and the close spatial relationship of the vessels to each other. The UV enters the fetal abdomen in the midline and has a short extrahepatic course before entering the liver with a slight right tilt. The UV enters the liver at the porta hepatis and drains into a confluence called the portal sinus. The portal sinus is a vascular space at the confluence of the following vessels: UV, DV, extrahepatic portal vein, and left and right intrahepatic portal veins. The extrahepatic portal vein (also called the main portal vein) is formed by the fusion of both the superior mesenteric and splenic veins and enters the portal sinus slightly inferior to and to the right of the origin of DV. In the liver, it forms the intrahepatic portal vein, which bifurcates into the left and right intrahepatic portal veins. The left intrahepatic portal vein divides into three main branches—the inferior, superior and medial, whereas the right intrahepatic portal vein bifurcates into the anterior and posterior branches (7, 11).
Visualization. The umbilical–portal system in the fetus can be demonstrated on ultrasound on a transverse plane of the upper abdomen (Fig. 10.7). In this plane, the UV appears to enter the abdomen and ends blindly as it forms an L-shaped structure pointing to the right with a 90-degree angle (Figs. 10.3 and 10.7). The right-sided structure is the portal sinus, which gives rise to both the left and right intrahepatic portal veins. Color Doppler facilitates visualization of the umbilical and portal venous systems (Fig. 10.7). By slightly angling the transducer downward, the main portal vein, coming from the left side, can be seen connecting into the portal sinus (Fig. 10.7). An insonation from the right and anterior side of the fetus will show the antegrade flow in the main and right portal veins, whereas the flow is noted downward in the left portal vein (Fig. 10.8). In this plane, the connection of the main portal vein and the portal sinus can also be identified.
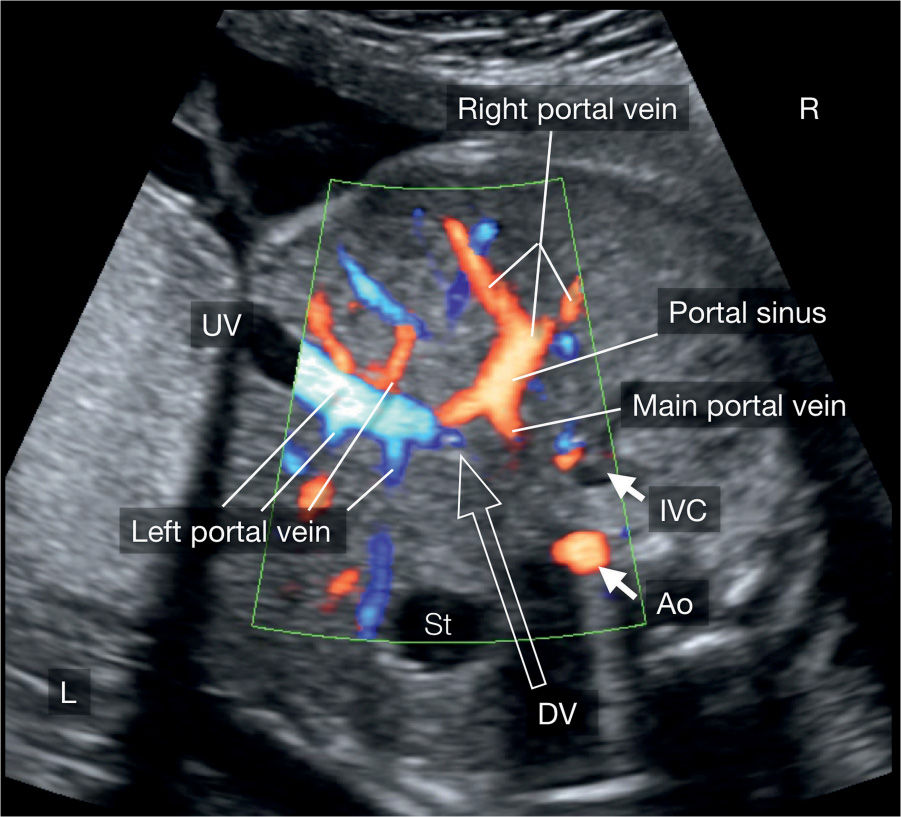
Figure 10.7: Axial plane in color Doppler of the liver, imaged from the fetal right side, showing the umbilical and portal venous system. See text for details. UV, umbilical vein; DV, ductus venosus; IVC, inferior vena cava; Ao, descending aorta; St, stomach; L, left; R, right.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


