The goal of perinatal care is to improve survival, minimize the occurrence and severity of long-term adverse neurodevelopmental outcomes, and enhance health-related quality of life. Advances in neonatal intensive care have successfully led to dramatic decreases in infant mortality rates. As survival improves, we need to know what the future of these new survivors will be. Without long-term follow-up, negative effects of medical interventions cannot be identified and patient outcomes are unlikely to improve. Significant variations in neonatal practices and short- and long-term morbidities exist (1), which suggests that practices associated with better outcomes can be identified. Unlike survival, the evaluation of long-term outcomes is challenging. In this chapter, the current knowledge on the longterm outcomes of children born premature and of those in other select perinatal risk groups is discussed, in addition to providing an overview of the organization of high-risk infant follow-up programs.
The World Health Organization’s 1980 terminologies for impairment, disability, and handicap have changed. In 2001, the World Health Organization endorsed use of the International Classification of Functioning, Disability, and Health (ICF). The ICF addresses health and disease from the perspective of body structures and functions and individual activities and participation (Table 56.1). It acknowledges the influence of environmental and personal factors and shifts the focus from disease to health (2). The ICF-Children and Youth considers activities and participation, body function and environment by the following age categories: less than 3, 3 to 5, 6 to 12, and 12 to 17 years.
There is a baseline risk of adverse neurodevelopmental outcome in the healthy term infant, which necessitates the need for comparison groups. In normal-birth-weight term controls, 4% had a substantial disability at 2 years of age (3). The definitions of disability vary and are discussed below. In addition to the effect on the child of adverse long-term outcomes, there are significant negative psychosocial and emotional impacts on parents, families, and society.
Sociodemographic factors such as socioeconomic status, social support, ethnicity, and maternal physical and mental health are important determinants of outcome. Several neonatal factors, severity of illness, and disease complications are predictive of longterm outcomes. Tremendous progress has been made in the use of advanced neuroimaging in the prognosis of neurologic outcomes (4). Postdischarge and subsequent illness, as well as early interventions and the home and community environments, may alter developmental trajectories.
▪ RISK OF NEURODEVELOPMENTAL DISABILITY
Preterm Infants
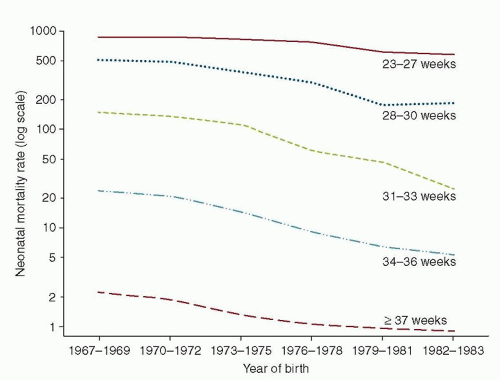
The advent of neonatal intensive care led to a dramatic improvement in survival rates for children born preterm (Fig. 56.1), with subsequent concerns regarding the long-term outcomes of these new survivors. In the last 30 years, there have been multiple publications documenting their long-term neurodevelopmental and health outcomes. The spectrum of complications and morbidity is inversely related to gestational age (GA) (5). The early focus was on low-birthweight (LBW) infants (<2,500 g birth weight), very-low-birth-weight (VLBW) infants (<1,500 g), and extremely low-birth-weight (ELBW) infants (<1,000 g) and as GA assessments improved, on very preterm (<32 weeks’ GA) and extremely preterm (<29 weeks’ GA) infants. Late preterm (34 to 36 weeks’ GA) infants comprise 9% of all live births and 70% of all births less than 37 weeks’ gestation. Though the incidence of neurodevelopmental disability in late preterm infants is less than their more premature counterparts, they are more than 3 times as likely as term babies to be diagnosed with cerebral palsy (CP) and 1.25 times more likely to be diagnosed with developmental delay or a cognitive impairment (6).
The preterm infant is different from the term infant because of the vulnerability of the actively maturing brain, increased risk of brain injury, and the effect of injury on brain maturation. Preterm birth occurs at a time of peak brain growth, synaptogenesis, developmental regulation of specific receptor populations, and central nervous system organization and differentiation (7). The transient fetal subplate neurons that guide cortical neuron wiring and maturation are particularly vulnerable to hypoxia. The periventricular white matter is the zone most vulnerable to watershed injury from hypoxia in the preterm infant. Intraventricular hemorrhage and periventricular hemorrhage are injuries specific to prematurity because of the evolution of the germinal matrix. The risk of neurodevelopmental disability with intraventricular hemorrhage is 5% to 10% for grade 1, 15% to 20% for grade 2, 35% to 55% for grade 3, and over 90% for grade 4 (8). Concomitant ischemic parenchymal injury is likely a significant contributor to the disabilities seen with intraventricular hemorrhage (8). Other susceptible areas include the hippocampus, which is associated with working memory and numeracy problems. Corticostriatothalamic pathway alterations may affect attention and neurobehavior (9), and cerebellar volume reduction is associated with poorer cognitive function (10). Newer studies using diffusion tensor magnetic resonance imaging (MRI) techniques are showing widespread abnormal maturation in white (11) and gray matter (12), independent of destructive brain lesions (13). MRI performed at term equivalent age can provide important information about brain injury and development, is feasible, and is a useful tool to predict neurodevelopmental outcome (4). Routine MRI for preterm babies in neonatal intensive care units (NICUs) has been recommended by some (4). Risk factors during the period of neonatal intensive care may affect the brain in multiple ways.
Factors that affect outcome can be categorized as biologic factors, therapeutic interventions, and environmental factors. Biologic factors include central nervous system insults (periventricular-intraventricular hemorrhage, periventricular leukomalacia, hydrocephalus), degree of prematurity, male sex, multiple birth, chorioamnionitis, necrotizing enterocolitis or sepsis (7), chronic lung disease, severe growth restriction (14), and some congenital abnormalities. Prolonged postnatal steroid therapy is associated with adverse neurologic outcomes in humans (15). In animal models, reductions in cerebral blood flow and hippocampal volume, altered white matter protein metabolism, delayed myelination of the optic axon, altered hypothalamic-pituitary-adrenal axis, and changes in dopamine receptor responses (16) have been associated with steroids. The repeated painful procedures that very premature babies undergo during their neonatal intensive care admission have been associated with abnormal white matter microstructure and intelligence at 7 years of age (17). Opioids do not mitigate this effect. Animal models have shown that general anesthetics can cause neuronal apoptosis in developing brains. Though not conclusive, there is concern that in young children repeated exposures to general anesthetics may be associated with learning disabilities and attention deficit disorder (18). Protective therapeutic interventions include a single course of antenatal corticosteroids, caffeine for apnea of prematurity, and antenatal magnesium sulfate.
The child’s family characteristics are major determinants of neurodevelopmental outcome and increasingly so as the child grows older. Measures of socioeconomic status include family income, parental educational level, and socioeconomic status, which may also interact with biologic factors. Mother-child interaction is a better predictor before 2 years of age (19). Maternal depression, substance use, and crowding in the home have a negative effect on outcome, and early intervention services are protective (14).
TABLE 56.1 International Classification of Functioning, Disability, and Health Definitions
In the context of health
Functioning is an umbrella term for body functions, body structures, activities, and participation. It denotes the positive aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors).
Disability is an umbrella term for impairments, activity limitations, and participation restrictions. It denotes the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors).
Body functions: The physiologic functions of body systems (including psychological functions).
Body structures: Anatomical parts of the body such as organs, limbs, and their components.
Impairments: Problems in body function and structure such as significant deviation or loss.
Activity: The execution of a task or action by an individual.
Participation: Involvement in a life situation.
Activity limitations: Difficulties an individual may have in executing activities.
Participation restrictions: Problems an individual may experience in involvement in life situations.
Environmental factors: The physical, social, and attitudinal environment in which people live and conduct their lives. These are either barriers to or facilitators of the person’s functioning.
From WHO 2001, 212-213—World Health Organization. How to use the ICF: a practical manual for using the International Classification of Functioning, Disability and Health (ICF). Exposure draft for comment. Geneva, Switzerland: WHO, 2013. Publicly available online.
Major Disabilities Detectable in Early Childhood
Moderate-to-severe disabilities can be detected in early childhood, though reported rates are higher than at older ages. Typical disability categories are motor (including CP), cognitive development, hearing, and vision. The presence of one or more major disabilities occurs in 6% to 8% of infants with birth weights 1,501 to 2,500 g, 14% to 17% with birth weight 1,001 to 1,500 g, and 20% to 25% in those weighing less than 1,000 g at birth compared to 5% in full-term infants (7). A meta-analysis of neurodevelopmental impairment and severe neurodevelopmental disability by GA (Table 56.2) for 22 to 25 weeks’ gestation showed a 6.5% reduction in impairment for each week gestation (20).
FIGURE 56.1 Neonatal mortality rate trends. From Moster D, Lie RT, Markestad T. Long-term medical and social consequences of preterm birth. N Engl J Med 2008;359:262-273.
TABLE 56.2 Results of a Meta-analysis of Neurodevelopmental Impairments at 22-25 Weeks’ Gestation