End-to-end anastomosis (EEA) sizer—One of a series of metal instruments that are used primarily to evaluate the size of the end-to-end bowel anastomosis. It is also an excellent instrument for distending and manipulating the vaginal apex from below, allowing the abdominal surgeon to easily feel the vagina and dissect against a firm surface (Fig. 39.1).
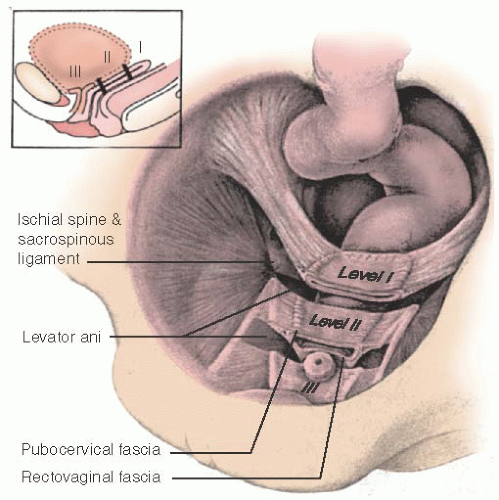
Levels of support defects (according to DeLancey classification)— Level I, apical defects caused by loss of support of the uterosacral ligaments, paracolpium, and parametrium; level II, disruption of the normal lateral attachments of the midvagina; and level III, lower vaginal defects in the perineal body or fusion of the distal urethra to the pubic bone.
Occult urinary stress incontinence—Stress incontinence that becomes apparent after treatment of apical vaginal prolapse. The presumed mechanism is resolution of urinary obstruction with correction of prolapse.
Uterine/cervical prolapse—Descent of the uterus or uterine cervix.
Vaginal vault prolapse—Descent of the vaginal vault (cuff scar after hysterectomy).
As women live longer and healthier lives, pelvic floor disorders continue to become even more prevalent and are an important health and social issue. The prevalence of symptomatic prolapse increases with increasing age. The lifetime risk of surgery for pelvic prolapse has been estimated at 7%. Clark et al. found that 12% of women undergo a second surgery within 6 years of the first procedure due to recurrence, and Denman et al. found the recurrence rate was 17% at 10 years. Thus, prolapse surgery is common, and reoperation is an important concern.
The management of pelvic organ prolapse can be challenging because different support defects often coexist and because of the variable effects on bowel, bladder, and sexual function. The pelvic surgeon must be adept in the thorough evaluation and management of these issues. An understanding of the anatomy and the relationship of the vagina to surrounding structures is imperative.
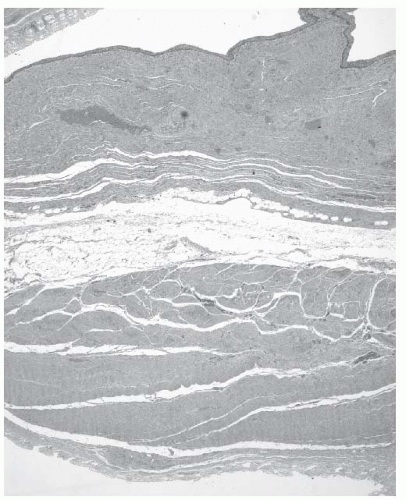
Our understanding of pelvic prolapse and the treatment thereof has changed in recent years. A number of theories have been proposed to explain the development of pelvic prolapse. It was formerly taught that prolapse resulted from attenuation or stretching of endopelvic fascia. Richardson, Lyon, and Williams challenged this theory by introducing the concept of discrete breaks in endopelvic fascia. However, microscopic studies have failed to identify a distinct histologic “fascia” along the anterior and posterior vaginal wall. Currently, it is now generally accepted that the dense tissue under the vaginal epithelium is muscularis rather than fascia. Also, Richardson’s description of an enterocele as a separation of pubocervical fascia from rectovaginal fascia is at odds with microscopic studies of patients with enteroceles, which have failed to identify peritoneum in contact with vaginal epithelium (Fig. 39.2). Work by DeLancey and colleagues has suggested that pelvic muscle weakness may play a critical role in the genesis of prolapse. Specifically, poor function of the levator ani muscle complex or detachment of the levator ani from the pubis may contribute to the development of prolapse for some women. Each of these theories contributes to our overall understanding of vaginal support.
FIGURE 39.1 Instruments useful for the manipulation of the vagina during sacral colpopexy. Shown are a commercially available disposable plastic stent (RUMI handle and Sacrocolpopexy Tip, CooperSurgical, Trumbull CT) and an end-to-end anastomosis (EEA) sizer. (Photo courtesy of Victoria L. Handa.)
FIGURE 39.2 Microscopic hematoxylin and eosin stain of the upper third of the vagina. The vaginal epithelium is at the top, and the rectal mucosa at the bottom.
DeLancey divided the support of the vagina into three levels (Fig. 39.3). This concept is helpful in understanding normal anatomic relationships and appreciating why certain repairs may work in some patients and not in others. Level I support defects are apical defects, which correspond to loss of support of the uterosacral ligaments, paracolpium, and parametrium. Level II support defects may represent loss of normal lateral attachment of the midvagina. Level III support defects correspond to loss in the support of the perineal body or distal urethra.
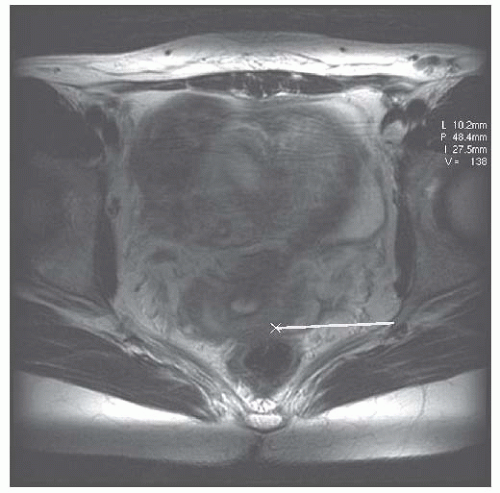
The goals of surgery for pelvic organ prolapse should be to restore anatomy and minimize symptoms. With respect to restoring anatomy, the main goal should be to suspend the vaginal vault as near as possible to its normal anatomic position. Magnetic resonance imaging (Figs. 39.4 and 39.5) demonstrates that the normal position of the vaginal apex is approximately 5 cm inferior to the second sacral vertebral body and approximately 5 cm medial to the ipsilateral ischial spine. Surgeries that recreate this anatomy will also accomplish the goal of suspending the vaginal apex over the levator plate. Distortion of the position of the vaginal apex, whether in an anterior or posterior direction, can contribute to dyspareunia and could contribute to recurrent prolapse opposite the vaginal vault.
It is extremely important to determine preoperatively whether lower urinary tract dysfunction, sexual dysfunction, and defecatory dysfunction exist. Surgery for pelvic organ prolapse may offer an opportunity to address other pelvic floor problems, including stress urinary incontinence and rectal prolapse. Stress urinary incontinence may be masked in patients with advanced pelvic organ prolapse by obstructing or kinking the urethra. Thus, assessment for “occult” stress incontinence (with reduction maneuvers) has been proposed to identify those patients who would benefit from an anti-incontinence procedure in conjunction with their pelvic reconstructive surgery. However, the value of testing for “occult” incontinence remains controversial.
FIGURE 39.4 Sagittal MRI illustrating the relationship between the posterior vaginal fornix and the anterior surface of the middle of the second sacral vertebra.
Another controversy is the value of initiating local estrogen therapy preoperatively in patients who have urogenital atrophy. Cytologic and histologic changes in the vaginal epithelium are seen after as little as 3 weeks of therapy, and therefore, 3 to 6 weeks of preoperative vaginal estrogen may be recommended by some surgeons. However, the benefits of preoperative estrogen therapy have not been demonstrated.
FIGURE 39.5 Axial MRI illustrating the relationship between the left cervical vaginal junction (×) and the left ischial spine.
Many operations have been described for suspending the prolapsed vaginal vault. There is no general consensus on what is the best procedure. The choice of procedure is influenced by many factors, including the comfort and skill of the surgeon; whether the prolapse is primary or recurrent; the patient’s age, state of health, and sexual activity; anticipated outcome; and overall state of the tissues.
PROCEDURES TO SUSPEND THE VAGINAL APEX
McCall Culdoplasty
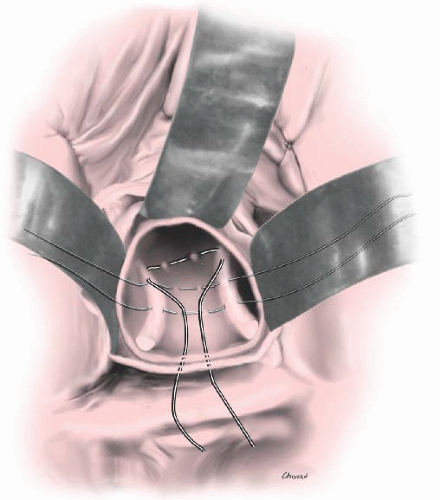
Several operations have been described and used by surgeons for vaginal vault suspension with correction of concurrent enterocele. McCall (in 1957) described his technique of surgical correction of enterocele at the time of vaginal hysterectomy. He used several nonabsorbable sutures to obliterate the enterocele (internal McCall sutures) by approximating both uterosacral ligaments and a running suture through the posterior peritoneum (Fig. 39.6). Delayed absorbable sutures are then inserted through the full thickness of the posterior vagina just lateral to the midline and passed through each uterosacral ligament and back out the posterior vaginal wall. Additional external sutures are placed as required by the amount of prolapse. The internal sutures are then tied, and the external sutures are tied after the vaginal cuff is closed. This simple procedure obliterates the cul-de-sac, supports the vaginal apex, and lengthens the posterior vaginal wall. McCall originally reported on 45 cases and stated there was no incidence of enterocele recurrence.
STEPS IN THE PROCEDURE
McCall Culdoplasty
The patient is positioned in high lithotomy position.
The bladder is drained.
If the procedure is done in the setting of vaginal hysterectomy, the hysterectomy is completed. If a hysterectomy was previously performed, the apex is grasped with Allis clamps and a colpotomy created.
The enterocele is obliterated with nonabsorbable sutures, plicating the uterosacral ligaments and inter-vening peritoneum.
A delayed absorbable suture is inserted through the full thickness of the posterior vagina (just lateral to the midline). The suture is then passed through each uterosacral ligament and back out the posterior vaginal wall.
The permanent sutures are tied, obliterating the cul-de-sac.
The delayed absorbable suture is tied, suspending the apex to the uterosacral ligaments.
Cystoscopy is performed to evaluate ureteral patency and to exclude lower urinary tract injury.
Several modifications of McCall technique have been described, most notably the modified endopelvic fascia repair, also known as a “Mayo culdoplasty.” The enterocele is delineated, and the sac is then dissected free and excised at the neck (Fig. 39.7). A wedge of vaginal mucosa is removed from the anterior and posterior vaginal wall. This narrows the vault when closed. The ureters are identified by palpation bilaterally. One to three internal McCall sutures are placed as described above, using nonabsorbable suture. After these sutures are placed and tagged, modified external McCall sutures are placed by passing delayed absorbable sutures through the posterior vaginal wall and peritoneum, through remnants of uterosacral and cardinal ligaments on the patient’s left. Several bites of peritoneum overlying the rectosigmoid are taken, and then the right perirectal fascia and uterosacral ligament are incorporated into the suture (Fig. 39.8). Last, the suture is passed back out through the posterior vaginal wall. The number of internal and external sutures placed depends on the size of enterocele and redundancy of the upper vagina. After these sutures are tied, the vaginal cuff is closed. There is a risk of ureteral injury or kinking, and therefore, ureteral patency should be confirmed at the conclusion of surgery.
In 1998, Webb reported on 693 women who underwent primary repair of posthysterectomy vaginal vault prolapse at the Mayo Clinic, including 660 who were treated with a Mayo culdoplasty. Among women followed for a mean of 7.4 years, 36/529 (7%) underwent further surgery for prolapse. Of 504 who completed a follow-up questionnaire, 80 (16%) reported symptoms of bulging or protrusion. While these results are encouraging, they are difficult to interpret without information regarding the severity of prolapse before surgery. It is also of note that 42 of 189 sexually active women (22%) reported dyspareunia at the time of follow-up.
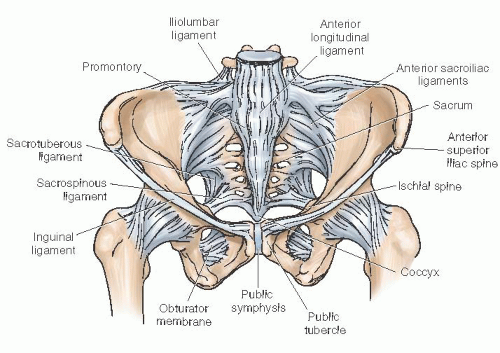
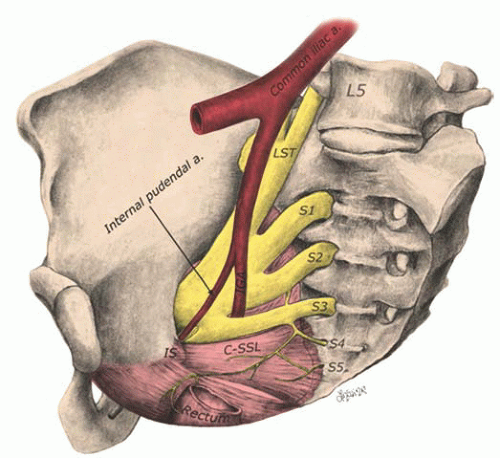
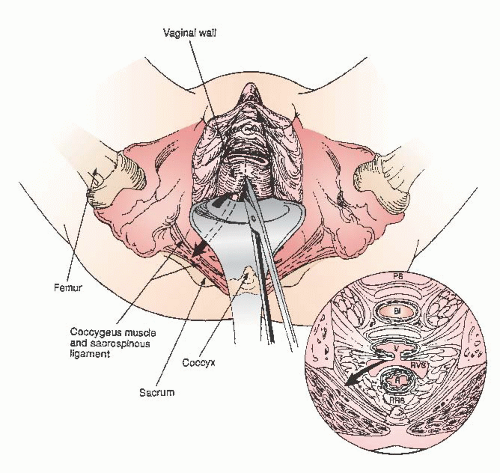
The sacrospinous ligament is a cordlike structure that exists within the body of the coccygeus muscle. The sacrospinous ligament attaches medially to the sacrum and coccyx and attaches laterally to the ischial spine (Fig. 39.9). The complex is collectively called the coccygeus-sacrospinous ligament (CSSL) complex. The CSSL is best identified by palpating the ischial spine and tracing the fingerlike ligamentous structure medially and posteriorly toward the sacrum. To perform sacrospinous ligament fixation, it is imperative that the surgeon be familiar with the anatomy of the sacrospinous ligament complex and of the pararectal space (Fig. 39.10). Obtaining adequate exposure is critical, and vascular complications, when encountered, may be life threatening. Superior to the ligament lie the inferior gluteal vessels and the hypogastric venous plexus. The pudendal nerve and vessels pass directly posterior to the ischial spine. The sciatic nerve, derived from the lumbosacral nerve roots, passes superior and lateral to the sacrospinous ligament. To avoid trauma to these structures, it is important to place the fixation sutures two fingers medial to the ischial spine.
FIGURE 39.9 Ligaments of the bony pelvis. The sacrospinous ligament extends from the ischial spine to the sacrum. The ligament is wider medially and narrows as it inserts on the ischial spine. The ligament lies within the coccygeus muscle (not shown).
The patient is positioned in high lithotomy position.
The bladder is drained.
If the procedure is done in the setting of vaginal hysterectomy, the hysterectomy is completed and the vaginal cuff is closed.
The surgeon identifies the intended vaginal apex.
The posterior vagina is incised longitudinally. The vaginal epithelium is dissected away to expose the rectovaginal space. If present, an enterocele is identi-fied and repaired.
A window is created in the rectal pillar, and the pararectal space is entered.
A pair of Breisky-Navratil retractors is used to expose the CSSL complex.
Using a Miya hook or similar instrument, a permanent suture is passed through the CSSL, two fingers medial to the ischial spine. The loop of the suture is retrieved with a nerve hook, pulled through, and tagged. A second suture is placed, 1 cm medial to the first.
One end of each suspension suture is sewn into the undersurface of the vagina apex and tied by a half hitch.
The upper aspect of the posterior vaginal incision is closed.
Traction on the free end of each suspension suture pulls the vagina directly onto the ligament. The surgeon then ties a square knot to anchor the apex to the ligament.
Cystoscopy is performed to evaluate ureteral patency and to exclude lower urinary tract injury.
The vagina may be packed for up to 24 hours after the procedure.
Most surgeons prefer to use the sacrospinous ligament opposite their dominant hand; that is, the right-handed surgeon uses the right sacrospinous ligament, although some surgeons prefer to perform a bilateral fixation. The first step of the surgery is to identify the intended vaginal apex by elevating the vagina to the ligament using an Allis clamp. It may be necessary to choose a different fixation point than the original vaginal cuff scar. This is best illustrated in a patient with a foreshortened anterior segment and a large enterocele. In this case, the new fixation point would be moved to an area over the enterocele. After identifying the intended vaginal apex, marking sutures are helpful to identify this site throughout the operation.
A posterior vaginal incision is made and extended to the vaginal apex. The rectovaginal space is developed. Almost always an enterocele sac is present. The enterocele sac should be mobilized off the posterior vaginal wall up to its neck; the sac is then opened and the peritoneum excised. The defect is then closed with purse-string sutures.
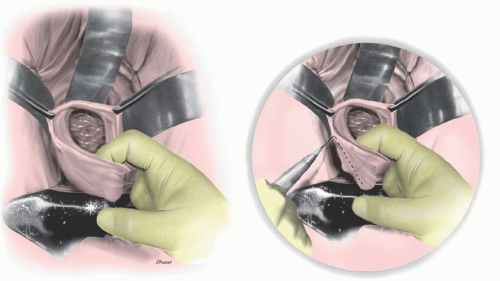
The next step is entry into the perirectal space (Fig. 39.11). The rectal pillar separates the rectovaginal space from the perirectal space. A window must be created through the rectal pillar, which is best accomplished by blunt dissection just lateral to the enterocele sac over the ischial spine. The window can also be created with the tips of scissors, a tonsil clamp, or a hemostat. The window should be gently enlarged to accommodate the vagina. The sacrospinous ligament can then be palpated by palpating the spine and moving the fingers dorsal and medial. It may be necessary to use blunt dissection to remove excess tissue from the CSSL.
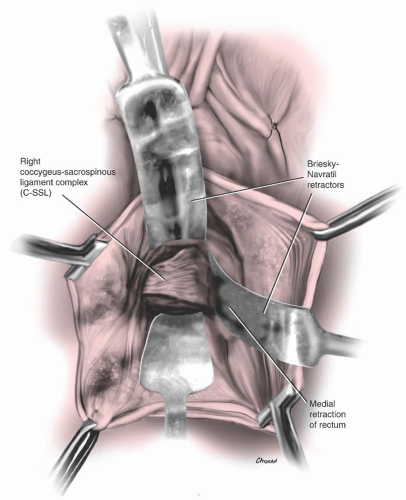
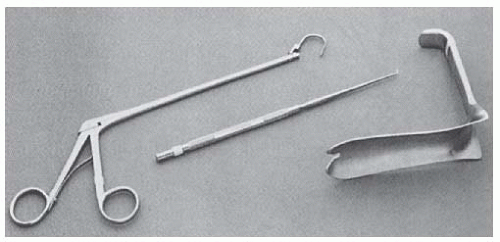
Once the window has been created and the ligament is identified, a Breisky-Navratil retractor is used to displace the rectum medially and to expose the CSSL complex (Fig. 39.12). Great care must be taken to avoid raking the retractor over the anterior surface of the sacrum and causing damage to presacral nerves and vessels. Traditionally, the Deschamps ligature carrier was used to pass the suture through the sacrospinous ligament, but this may be more cumbersome than are other methods. We recommend a Miyazaki hook (Miya hook; Fig. 39.13) for placement of the suspension sutures. The Miya ligature carrier is easy to operate and facilitates penetration of the sacrospinous ligament under direct visualization.
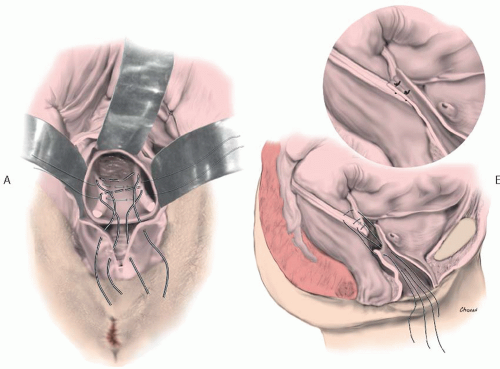
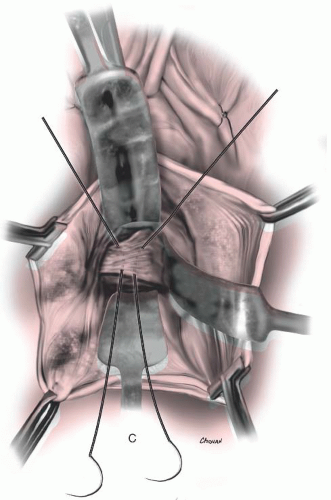
Palpation of the ischial spine identifies the correct location for the placement of the sutures, along the inferior half of the sacrospinous ligament, two fingers medial to the ischial spine. The ligament is exposed using a pair of Breisky-Navratil retractors, and a notched speculum is inserted. The notch can be used to guide placement of the suture. Nonabsorbable suture is used. There should be considerable resistance as the carrier is pushed through the body of the ligament. If no resistance is felt, the surgeon should suspect that the carrier either passed in front of or around the ligament. After the suture has been passed, the loop of the suture is retrieved with a nerve hook, pulled through, and tagged. A second suture is placed in a similar fashion approximately 1 cm medial to the first (Fig. 39.14). If a good purchase of tissue has been taken, the surgeon should be able to gently move the patient with traction of the suture.
Once the surgeon has the two sutures through the sacrospinous ligament, the vaginal vault can be suspended. There are two ways for the surgeon to attach the sutures to the vagina. The first is to use a pulley stitch. Here, one end of the suture is sewn into the full thickness of the fibromuscular layer on the undersurface of the vagina (excluding the epithelium) and then tied by a half hitch. Traction on the free end of the suture will pull the vagina directly onto the ligament. Suture bridging should be avoided, since this could predispose to recurrent prolapse. Once pulled into position, a square knot is used to fix the suture in place. A second technique involves passing each end of the sutures through the full thickness of the vagina. This technique requires the use of absorbable suture, however.
The upper portion of the posterior vaginal wall should be closed with interrupted or running 3-0 absorbable sutures before tying the colpopexy sutures. If the colpopexy sutures are tied before the proximal posterior wall is closed, the visibility of the vault is reduced, and this segment of the posterior vaginal incision is difficult to close.
After the colpopexy sutures are tied, a posterior colporrhaphy and perineorrhaphy are usually performed. If an anterior colporrhaphy is planned, this step is most easily accomplished prior to the sacrospinous suspension. At the conclusion of surgery, the vagina is then packed with moist gauze for 12 to 24 hours.
Injury to the ureter or obstruction due to ureteral kinking has been reported after sacrospinous suspension. Therefore, cystoscopy with assessment of ureteral patency should be performed at the conclusion of surgery.
The overall results from sacrospinous fixation have been good. A 2007 systematic review suggested a low rate of apical prolapse beyond Baden-Walker grade 1 (7.2%, 95% confidence interval: 4.0% to 10.4%). Symptom relief was noted in approximately 90% of women across seven studies. However, recurrent prolapse of the anterior wall remains a long-term challenge after sacrospinous suspension. Specifically, one third of patients may experience recurrent prolapse to or beyond the hymen if all vaginal segments are considered.
Complications can occur, and the more common complications are discussed here. It is important to do a rectal examination during this procedure to make sure that no inadvertent proctotomy has occurred. If there is evidence of suture penetration, the offending suture should be removed and replaced. Lacerations should be closed in a standard two-layer fashion.
Only gold members can continue reading. Log In or Register to continue