Training the Gynecologic Surgeon: Maintaining and Improving Surgical Skills
Training the Gynecologic Surgeon: Maintaining and Improving Surgical Skills
Tola B. Fashokun
Victoria L. Handa
DEFINITIONS
Assessment—The process of measuring a trainee’s knowledge skills, judgment, or professional behavior against defined standards.
Deliberate practice—A highly structured form of training that consists of focused, repetitive practice in which the subject continuously monitors his or her performance and subsequently corrects, experiments, and reacts to immediate and constant feedback, with the aim of steady and consistent improvement.
Global Rating Index for Technical Skills (GRITS)—A validated assessment tool used for evaluation of intraoperative performance.
Learning style—The process by which a person understands and retains information, thereby gaining knowledge or skill.
Learning theories—Conceptual frameworks and principles that attempt to explain the learning process.
Mental imagery (mental practice)—The cognitive rehearsal of a task with or without physical movement. It can be used to enhance the acquisition of new technical skills.
Objective Structured Assessment of Technical Skills (OSATS)—A valid and reliable examination in which subjects perform standardized surgical procedures while being evaluated by an expert surgeon.
Simulation—The act of reproducing or imitating a real-life event, process, or procedure. It can be utilized both as an effective training technique and assessment tool.
Vaginal Surgical Skills Index (VSSI)—A validated procedure-specific assessment tool used for intraoperative evaluation of vaginal surgical skills.
“It would take me one year to teach a traineehowto do an operation, five years to teach themwhento do the operation, but a lifetime to teach themwhen notto do an operation.”
Lord Smith, past President of The Royal College of Surgeons of England
HISTORY OF SURGICAL EDUCATION
For more than a century, the surgical teaching model introduced to Johns Hopkins Hospital in 1889 by Dr. William Halsted has been the standard approach for training surgeons. Under this apprenticeship model, the surgeon trainee experiences “…the orderly exposure to graduated clinical experience in the operating room during several years of residency under the close tutelage of dedicated senior attending surgeons….” This widely accepted and historically successful model traditional paradigm “to see one, do one, teach one” led to the declaration that “the operating room is the surgeon’s classroom.”
However, there are limitations to this surgical education model. Variability in the number and type of surgical cases and duration of apprenticeship will impact training. Second, this model does not provide for remediation. Even Dr. Halsted recognized this limitation. Halsted observed, “experience can mean doing the same thing wrong over and over again.” Finally, this traditional method of training may not be practical given the current pressures of residency work hour restrictions, increasing numbers and complexity of surgical procedures, and financial and ethical constraints of teaching surgical skills in the operating room.
EDUCATIONAL THEORIES: HOW DO ADULTS LEARN?
A contemporary approach to surgical training requires consideration of not only what the trainee is learning but how they learn. Advances in educational research have identified principles of adult learning, and accumulating evidence suggests that surgical trainees have specific learning styles. The three basic types of learning styles are visual, auditory, and tactile. To learn, we depend on our senses to process the information around us. Most people tend to use one of their senses more than the others; however, it is not unusual to use a different style to learn a particular skill. For example, some novice surgeons may find it difficult to hear and then duplicate instruction on how to correctly apply a clamp; they may learn best by first observing and then performing the illustrated task. The latter method might have a direct impact on the efficiency of intraoperative teaching. This does not imply that one style is better than the other, but one style may be more preferable given the learning environment, and the trainee may need to make adjustments to minimize any obstacles to effective learning.
A better understanding of the factors that impact the process of learning new surgical skills will hopefully lead to a more effective and efficient educational model for surgical educators and novice surgeons. Dr. Reznick et al. have suggested that “adult learning is enhanced by an approach that is self-directed and centers on the learner rather than the teacher. Adult learning is facilitated by focusing on a problem or task. Abstract, subject-centered learning is less effective as a motivator. Adults also come to an educational activity, such as learning operative skills, with a vast amount of past experience that must be recognized and utilized.” Because the development of surgical skills is an active learning process, a surgeon’s optimal surgical education should be based on learning theory.
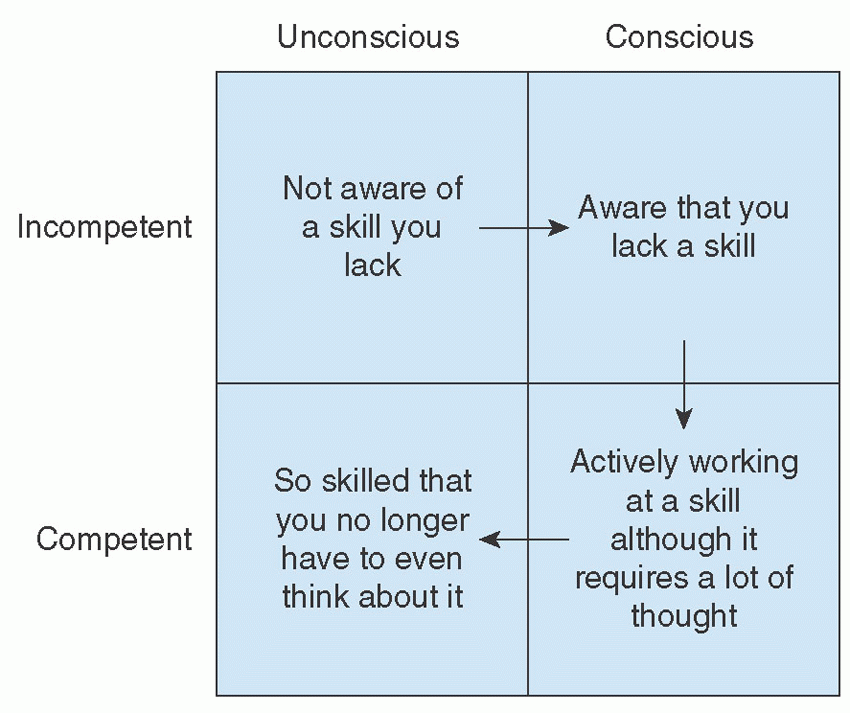
One learning model relates to the psychological states involved in the process of progressing from incompetence to competence in a skill (Table 6.1). This theory outlines four stages. The first stage is “Unconscious Incompetence”: You don’t know that you don’t know something. The second stage is “Conscious Incompetence”: You are now aware that you are incompetent at something. Next is stage 3, “Conscious Competence”: You develop a skill in that area but have to think about it. In the final stage is “Unconscious Competence”: You are now so good at it, and it now comes naturally. Obviously, most surgeons would agree that their goal is to achieve the final stage when a particular surgical skill becomes “second nature”; however, this may have a direct impact on one’s ability to teach this skill or procedure. Surgical educators are most effective when they are able to “break down” a complex procedure to its basic elements, which can be challenging if they are not “conscious” about the process.
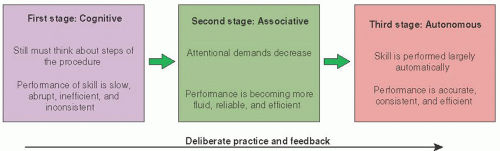
FIGURE 6.1 Fitts and Posner’s three-stage theory of motor skill acquisition.
TABLE 6.1 The Four Stages of Learning
Modern research in surgical education has also examined the specific steps involved in attaining motor skills. Fitts and Posner’s three-stage theory of motor skill acquisition (Fig. 6.1) is widely accepted in both the motor skills and surgical literature. In the first, cognitive stage, the learner is still in the process of obtaining information about how to correctly perform the skill, through reading or direct observation. In this stage, performance is relatively slow, abrupt, inefficient, and inconsistent. The learner must concentrate on the task, and attentional demands are high. In the second associative stage, through deliberate practice and feedback, the movement becomes more fluid with fewer interruptions and attentional demands decrease. After extensive practice, the performer reaches the final, autonomous stage, which is characterized by fluent and seemingly effortless motions. Movements are accurate, consistent, and efficient. The skill is performed largely automatically at this stage, and movement execution requires little or no attention. The understanding of skill acquisition has important implications in surgical training and is best illustrated by an example given by Reznick and MacRae, “….with a surgical skill as simple as tying a knot, in the cognitive stage the learner must understand the mechanics of the skill—how to hold the tie, how to place the throws, and how to move the hands. With practice and feedback, the learner reaches the associative stage, in which knowledge is translated into appropriate motor behavior. The learner is still thinking about how to move the hands and hold the tie, but is able to execute the task more fluidly, with fewer interruptions. In the autonomous stage, practice gradually results in smooth performance. The learner no longer needs to think about how to execute this particular task and can concentrate on other aspects of the procedure….”
Surgical trainees must have a firm understanding of basic skills first before they can progress to more complex and elaborate tasks, and the quality of performance requires assessment at every stage. Therefore, the earlier stages of teaching fundamental technical skills should take place outside the operating room; practice with constructive feedback is the rule until automaticity in basic skills is achieved. The mastery of basic skills allows trainees to focus on more complex tasks in the operating room.
OUT OF OPERATING ROOM LEARNING EXPERIENCES
Simulation
The advent of surgical simulation has resulted in significant and dynamic changes to surgical education. The use of simulation has been adopted from other disciplines, most notably the aviation industry. An obvious advantage of simulation training is that core skills can be learned prior to application in the operating room, theoretically improving safety and efficiency. Also, with a simulation curriculum, training opportunities are not constrained by the available clinical experience. Simulation offers the opportunity for repeated practice in a safe and controlled environment, focusing on trainees and tailored to their needs. Most surgical educators would agree that fundamental surgical principles and technical skills should be taught outside the operating room. Although some training programs include surgical training models in their surgical curricula, no simulation model has gained sufficient acceptance to be considered a gold standard. Simulation practices vary widely across and within residency programs. Several research studies have confirmed the positive impact on surgical skill of practice outside the operating room using surgical simulators. Trainees whose initial learning occurs in a simulated environment make fewer errors and complete the “real” operation faster than those without such training. In essence, better skills translate into better surgery.
TABLE 6.2 Simulation Methods
SIMULATION
DESCRIPTION/COST
PROS
CONS
Bench models
Suture boards and foam models
Low to mid cost
Inexpensive, safe, generally reusable; can perform basic tasks
Decreased realism; not able to perform more complex tasks
Mannequin
May be entire anatomy or pelvis
Mid to high costs
Multiple use; can perform basic or more complex procedures, patient specific
Team training
Limited realism, not “exact” anatomy, limited applications
Computer/virtual reality surgical simulators
Virtual software, computer visual-haptics
Can practice basic laparoscopic skills High cost
Multiple use, data capture, minimal setup time; provide performance feedback, can make patient-specific
Cost, maintenance, and down time; realism varies
Live animals
Primate, sheep, pig, rabbits
High cost
Closer to human anatomy; can perform entire operation or complex procedures
Expensive, differences in anatomy, single use; requires special facilities and personnel, tissue compliance, infection risks, ethical concerns
Cadavers
Entire anatomy, best used for continuing medical education
High cost
Accurate anatomy; can perform the entire operation
Expensive limited availability, single use, compliance of tissue, infection risks, and ethical concerns
There are a variety of types of surgical training models, including bench models, virtual reality trainers (computergenerated models), surgical simulation in live animal models, and surgical simulation in human cadavers (Table 6.2). These various simulators have advantages and disadvantages. All are believed to result in improved trainee performance that is transferable to the operating room.
However, it is unclear which type of trainer is superior. A number of studies have reached differing conclusions. For example, a Cochrane Database Systematic Review of the effectiveness of virtual reality training compared with physical reality simulators concluded that these two training methods result in similar laparoscopic skill acquisition, but that the virtual reality trainers may result in better transferability of skills into the operating room (especially for more complex tasks). In contrast, Denadai et al. demonstrated that the acquisition of suture skills was similar on a low- and high-fidelity bench model. Practice on either model was shown to improve performance compared to training with only didactic materials. However, another systematic review (performed by Sutherland et al.) of 30 randomized controlled trials concluded that simulation training was superior to no training but was not consistently superior to traditional training methods. Most investigators would agree that the effective use of surgical training models requires standardization of instruction, feedback, and evaluation.
Ultimately, the role of simulation in teaching surgical skills is to facilitate practice of technical skills. Ericsson et al. showed that becoming an expert takes about 10,000 hours of deliberate and distributed practice, regardless of whether the goal is to become a competent surgeon, a chess master, or a professional musician. Deliberate practice is defined as a “highly structured activity, the explicit goal of which is to improve performance.” In other words, time spent practicing a new surgical skill is most useful if the learner reflects on or receives feedback on performance (either self-evaluation or through formal assessment) and has numerous sessions distributed over time (e.g., throughout residency or fellowship), rather than the same number of hours compressed into a single training session. This confirms what other educators have suggested that “practice does not make perfect; perfect practice makes perfect.”
Simulation may also facilitate the evaluation of surgical skills. However, for simulation to provide a robust and valid assessment tool, the simulation exercise must be highly standardized, widely available, and focused on the critical aspects of performance. It is important that simulation is incorporated as part of a standard surgical curriculum, with well-defined learning goals and objectives that should be completed at specific time intervals.
MENTAL IMAGERY (MENTAL PRACTICE)
Mental imagery, also called visualization and mental imagery rehearsal, is “the cognitive rehearsal of a task with or without physical movement.” It can be used to enhance the acquisition of new technical skills and increase emotional preparedness to perform in stressful situation, both qualities applicable to the training of novice surgeons.
Educational researchers have examined whether the experience of mental imagery affects the degree of learning. For example, imagining playing a 5-finger piano exercise (mental practice) resulted in a significant improvement in performance over no mental practice—though not as great an improvement as that produced by physical practice. Mental practice alone seems to be sufficient to promote the modulation of neural circuits involved in the early stages of motor skill learning.
So how does this translate to the use of mental practice to teach surgical skills? Several studies support the use of this training tool to teach surgical skills. In a multicenter randomized controlled trial, gynecology residents who had performed three of fewer cystoscopies were randomized to preoperative mental imagery sessions or reading a book chapter describing cystoscopy. The imagery group’s surgical performance assessment was 15.9% significantly higher than controls (p = 0.03). In addition, residents considered mental imagery to be a more useful preoperative preparation. Two additional studies using mental imagery to teach medical students demonstrated similar results. Medical students who used mental imagery techniques had at least equivalent and sometimes superior results when compared to traditional methods of learning new skills.
Despite evidence to support its usefulness, the exact role of mental imagery in surgical training has yet to be clearly defined, and there is no ideal way to use this technique. Based on prior research, mental practice is most effective when the leaner is familiar with the task and the actual performance immediately follows the imagery session. Novice surgeons could use this technique in preparation for an “actual” surgery by reviewing details of an entire surgical procedure with the appropriate hand movements for the operation. Thus, this approach may offer a less expensive, efficient, and ethical way for a surgeon to acquire a new skill before operating on a “live” patient.
WEB-BASED LEARNING
In recent years, Web-based learning has become an emerging technology for learning and teaching surgical skills. This online learning environment includes access to videos as well as live surgeries viewed remotely. These resources support the learner-centered teaching approach, facilitating interactions with experts and with other learners. The availability of online surgical videos provides a useful resource that complements the more traditional options, including textbooks and case observation. However, the quality of materials available on the Internet is variable, and the materials available are typically not subject to peer review. Despite these limitations, Webbased learning may be a valuable resource for more seasoned surgeons interested in obtaining knowledge about a newer procedure or technique. In fact, most webcasts are created for surgeons already familiar with certain aspects of a surgical procedure or basic technical skills; surgical webinars provide an opportunity for these surgeons to interact live with an expert surgeon and may be the catalyst for a surgeon to seek more formal training.
TEACHING IN THE OPERATING ROOM
Simulation training and other surgical educational opportunities only complement traditional surgical educational experience (in operating room learning) but cannot replace it. The operating room is obviously a unique educational setting for several key reasons; first it can be a very high-stress environment for surgical educators and learners alike given the concern for providing an optimal surgical outcome in a safe, controlled, and efficient manner. In addition, it provides the teacher and learner with uninterrupted time together, and this time can and should be used for clinical teaching and learning. Operating room teaching should be similar to other structured learning activities in which key learning objectives and goals for the learner are reviewed prior to case. It is not acceptable or ethical for novice surgeon to learn a “new” technical skill without supervision. Dr. Roberts et al. emphasized the importance of deliberate and guided instruction in the operating room. The authors refer to this teaching method as “briefing, intraoperative teaching, and debriefing” or BID. The educational framework for this teaching begins with the “briefing” component before the surgery at the scrub sink; with a short interaction between the surgical educator and the learner assessing the needs of the learner and identifying mutual learning objectives. It is important that the learner is active in this process because it encourages the learner to reflect on areas that may need improvement (from previous surgeries) and formulate needs to be addressed in the current surgery. The “intraoperative teaching” should involve coaching and guiding the learner through the surgery, but the didactics or “teaching script” used during the operation should focus on the preestablished learning objectives. This more tailored approach is to avoid overloading the learner with too much information, which then becomes difficult to apply to future practice. The “debriefing” should occur at the end of the procedure and concentrate on four areas of discussion: reflection, rules, reinforcement, and correction. Details about this process are discussed later in the chapter.
Surgical educational researchers have consistently identified certain principles of effective intraoperative teaching: They include explaining reasons behind decisions, providing clear answers to questions, involving learners (letting them “actually operate”) with direct supervision, and providing feedback without belittling.
SURGICAL SKILLS ASSESSMENTS
Assessment is the process of measuring a trainee’s knowledge, skills, judgment, or professional behavior against defined standards. Ideally, the assessment tool should be objective, reliable, and reproducible. Assessment can have different and multiple purposes, including aiding learning through constructive feedback, measuring progress over time, and/or determining a level of competence.
Only gold members can continue reading. Log In or Register to continue