Ultrasound-Assisted Suprapubic Bladder Aspiration
John M. Loiselle
Introduction
Suprapubic bladder aspiration of urine is a means of obtaining urine in a sterile fashion by passing a needle through the abdominal wall directly into the urinary bladder. This technique is most commonly used to collect urine from incontinent children as part of a sepsis evaluation when isolating an organism from the urinary tract may be of paramount importance. A urine culture obtained by a suprapubic aspiration is considered the gold standard for detecting bacteruria (1). The suprapubic approach avoids potential contamination from organisms present on the perineum or in the distal urethra. Numerous studies have demonstrated the superiority of suprapubic bladder aspiration compared with other techniques of collecting urine for culture in infants and toddlers (2,3,4,5,6,7,8). Although the technique is inherently invasive, few serious complications have been reported with suprapubic bladder aspiration (9,10,11).
Reported rates of successfully obtaining urine by suprapubic bladder aspiration vary from 23% to 90% (1,2,5,7,8,12,13,14,15). Despite the straightforward nature of the technique, suprapubic bladder aspiration performed in an emergency department (ED) setting is often unsuccessful. Experience with the technique improves the success rate (13,15), but a primary factor for failure to obtain urine is the lack of urine in the bladder at the time of the attempt.
Ultrasound was first described as a useful adjunct to suprapubic aspirations in infants in the early 1970s (16). The advent of relatively low cost, portable ultrasound devices has expanded the availability of this noninvasive diagnostic technique to a variety of clinical settings. Ultrasound can be used to determine the presence of urine within the bladder before suprapubic bladder aspiration or to guide the needle during the procedure. Several studies demonstrate that ultrasound can accurately predict the volume of urine in the infant bladder (17,18) and improve the success rate in obtaining urine specimens when compared with blind aspiration (12,13,15,19,20). In addition to the ED setting, this technique may prove valuable in neonatal intensive care units and other areas where suprapubic bladder aspiration is performed regularly.
Suprapubic bladder aspiration is usually performed by a physician and can be done in most inpatient and outpatient settings. Physicians with no formal training in ultrasonography have been able to assess bladder volume accurately (12,18). The relative ease of learning and performing the ultrasound procedure allows trained physician assistants, nurse practitioners, and nurses to use it as well.
Anatomy and Physiology
The urinary bladder is an intra-abdominal organ in infants and children under 2 years of age, making it easily accessible by suprapubic bladder aspiration. As a child grows, the bladder recedes into the pelvis and, in older children, enters the abdomen only when full. When suprapubic bladder aspiration is performed in the midline along the suprapubic crease, the needle passes through skin, rectus muscle, and the anterior wall of the bladder. When viewed by ultrasound, these tissues create a lighter background than the full bladder, which appears as a black ovoid structure (Fig. 133.1).
Indications
Suprapubic bladder aspiration may be indicated in incontinent children less than 2 years of age when the collection
of sterile urine is necessary and urethral contamination must be avoided. A common clinical situation that may necessitate suprapubic bladder aspiration is the sepsis evaluation in a febrile infant. A urinary tract infection is a common source of bacterial infection in these infants, and obtaining uncontaminated urine that allows identification of a true pathogen is imperative. Aspiration of the bladder may also be used when uncontaminated urine must be obtained from the incontinent child who has gastroenteritis and frequent diarrheal stools.
of sterile urine is necessary and urethral contamination must be avoided. A common clinical situation that may necessitate suprapubic bladder aspiration is the sepsis evaluation in a febrile infant. A urinary tract infection is a common source of bacterial infection in these infants, and obtaining uncontaminated urine that allows identification of a true pathogen is imperative. Aspiration of the bladder may also be used when uncontaminated urine must be obtained from the incontinent child who has gastroenteritis and frequent diarrheal stools.
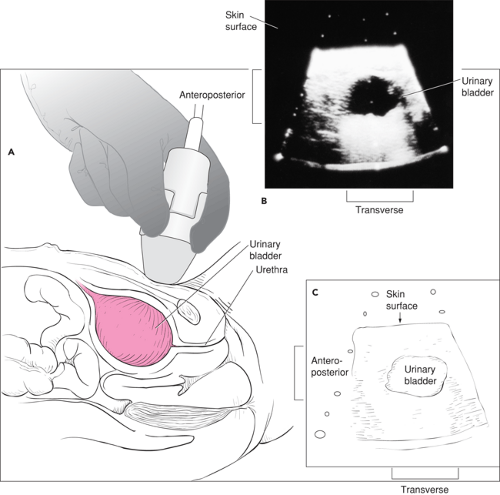 Figure 133.1 A. Position of the patient and ultrasound probe for scanning the bladder. B. Ultrasound image of a full urinary bladder in an infant. C. Schematic depiction of an ultrasound image. |
Urethral catheterization is widely used in lieu of suprapubic bladder aspiration, and it is the procedure of choice in most facilities. Urethral catheterization is more often successful in obtaining an adequate volume of urine for culture than suprapubic aspiration (21) and is less painful for the infant (22). However, the incidence of contamination is higher in cultures obtained by urethral catheterization than in those obtained by suprapubic aspiration (1). At times, anatomic considerations limit the opportunities for urethral catheterization. It is
occasionally difficult to find the urethral orifice in the infant female. A suprapubic aspiration may be the preferred method of urine collection in the young female infant with labial adhesions or the male infant with a minimally retractable foreskin (1).
occasionally difficult to find the urethral orifice in the infant female. A suprapubic aspiration may be the preferred method of urine collection in the young female infant with labial adhesions or the male infant with a minimally retractable foreskin (1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


