Torsion of Ovary
Mehdi Parva
Charles J. Dunton
Causes of acute abdominal pain unique to women include pelvic inflammatory disease, ectopic pregnancy, endometrioma, rupture or hemorrhage of a corpus luteum cyst, and torsion of adnexal structures (1). Although uncommon, adnexal torsion is not rare and comprises approximately 3% of surgical emergencies in women (2). Diagnosis of this condition is challenging. Prompt diagnosis may allow for preservation of the adnexal structures and fertility.
ETIOLOGY
Torsion of the adnexa is caused by rotation of the ovary or the adnexa about the ovarian pedicle, resulting in arterial, venous, or lymphatic obstruction (Fig. 23.1). Initially, the venous and lymphatic obstruction without arterial obstruction produces edema and enlargement of the ovary. If arterial obstruction occurs, the organs may become necrotic and gangrenous. This in turn may lead to peritonitis and intestinal obstruction. In some cases, the twisted adnexa may be absorbed, leading to unilateral absence of the adnexa. Torsion of the fallopian tube alone is rare and has been associated with hydrosalpinx, neoplasms of the tube, and previous tubal ligation (2,3,4,5) (Fig. 23.2). Torsion of the adnexa is increased in ovarian hyperstimulation syndrome (OHSS) caused by menotropin therapy for infertility (6,7,8).
Pregnancy has been associated with an increased risk of adnexal torsion (9,10). If an adnexal mass is associated with a pregnancy, a recent review found that the most frequent complication was torsion (11). This may be due to the repositioning of the ovaries by the enlarging uterus. Torsion is most likely in the first trimester (10,12).
Torsion of the adnexa may involve the ovary, the fallopian tube, or both structures together. In most cases, an ovarian neoplasm is involved (9). Nonetheless, in up to 18% of cases, the torsion may involve normal tubes and ovaries. In keeping with the age of the patient population, the neoplasms are usually benign (Table 23.1). The most common neoplasm is the dermoid cyst. Paraovarian cysts have the highest relative risk of torsion (9,13).
It is unusual for malignant neoplasm to present with symptoms of torsion. A review of 10 years’ experience at the Women’s Hospital, Los Angeles County, showed only two cases of malignant neoplasms undergoing torsion. In comparison, the relative risk for a benign neoplasm to undergo torsion was 12.9% (95% CI, 10.2 to 15.9) (14,15). However, if a postmenopausal woman presents with torsion, clinicians should consider the possibility of malignancy. In series with a high percentage of malignancy reported with torsion, most patients were postmenopausal (13,16). Postmenopausal patients also had a delayed diagnosis compared to younger patients (13).
Torsion of a normal ovary may present as a massive ovarian edema. This tumor-like condition presents with significant ovarian enlargement and pathologically shows only edema of a normal ovary (17).
CLINICAL FEATURES
The clinical diagnosis of adnexal torsion is often difficult. It occurs mainly in young women and less frequently in children and postmenopausal females. Pain,
low-grade temperature, moderate leukocytosis, and nausea and vomiting (70%) are present in most cases. The pain associated with torsion may be unilateral or bilateral (25%) and either intermittent or constant. The pain may be acute, in onset, and may be associated with a vigorous activity or a change in position. The pain may be out of proportion to other findings. Later in the course, if necrosis occurs, high fever and marked leukocytosis may be seen (17,18,19,20) (Table 23.2). Symptoms may be present for a number of days prior to the patient seeking medical attention, and physician delay prior to surgical treatment is not uncommon. Reviews showed that the median onset of pain was 1 day, but the range was 0 to 210 days, with a median of 7 to 8 days (18).
low-grade temperature, moderate leukocytosis, and nausea and vomiting (70%) are present in most cases. The pain associated with torsion may be unilateral or bilateral (25%) and either intermittent or constant. The pain may be acute, in onset, and may be associated with a vigorous activity or a change in position. The pain may be out of proportion to other findings. Later in the course, if necrosis occurs, high fever and marked leukocytosis may be seen (17,18,19,20) (Table 23.2). Symptoms may be present for a number of days prior to the patient seeking medical attention, and physician delay prior to surgical treatment is not uncommon. Reviews showed that the median onset of pain was 1 day, but the range was 0 to 210 days, with a median of 7 to 8 days (18).
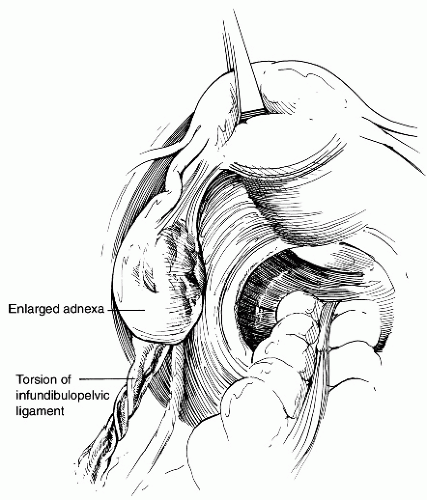 FIGURE 23.1 Torsion of infundibulopelvic ligament. |
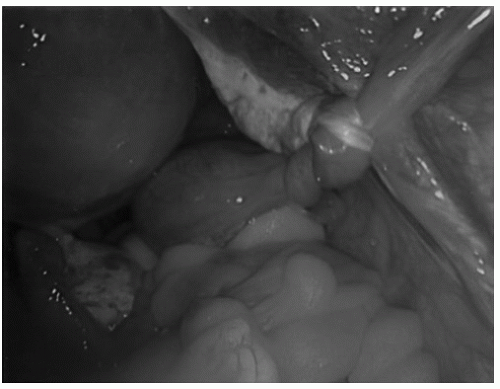 FIGURE 23.2 Torsion of the adnexa. |
TABLE 23.1 Pathology of Torsed Adnexes | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


