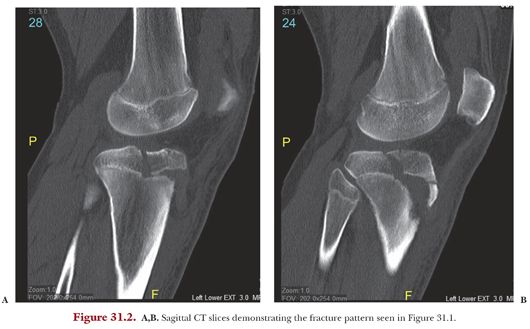
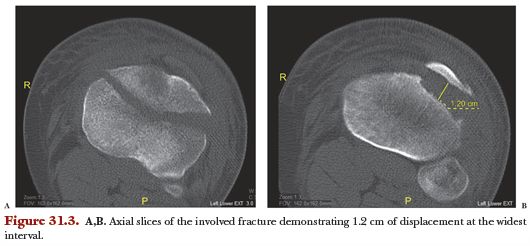
Tibial tubercle avulsion injuries often involve complex fracture patterns, and although standard radiographs may help in the diagnosis of injury, they are insufficient in the characterization of fracture pattern. Computed tomography (CT) is required for a precise understanding of fracture configuration (Fig. 31.2). In some cases, the fracture visualization afforded by CT allows for more accurate classification of the fracture and targeted preoperative planning as compared to what was originally provided in plain radiographs. In particular, CT allows the surgeon to gauge whether there is fracture extension into the joint (Fig. 31.3). Magnetic resonance imaging may be performed if there is a high index of suspicion for meniscal injury, ligamentous injury, or cartilage damage through the physis and epiphysis.
Classification of tibial tubercle avulsion fractures is based primarily on the Watson-Jones classification. Type I fractures involve a small avulsion from part of the tubercle. Type II extend through the physis without entering the joint. Type III, unlike type II, involve fracture extension into the joint. There are modifications to this original classification system. The Ogden classification was derived with types I to III modifiers to describe the injury severity for each various type of fracture.22 Ogden added A and B subtypes in order to indicate displacement and comminution. A type C has been added and this describes associated patellar ligament avulsions.23 Types IV and V classification also have been described.24,25 Type IV injury involves complete tibial epiphysis involvement, whereas type V has been described as a type IIB with an associated type IV, thereby creating a “Y” fracture configuration.
Management of tibial tubercle avulsion fractures is dictated by the fracture type and classification. Types IA and IB fractures can be treated successfully with conservative management: closed reduction and casting with the knee in extension. Type IC fractures, however, are better treated with open reduction internal fixation (ORIF) of the avulsed osseous fragment and patellar ligament.
ORIF is also performed for types IIB, IIC, IIIA, IIIB, IIIC, and any IV and V tibial tuberosity avulsion fractures. In addition to addressing the primary fracture, associated quadriceps or patellar tendon avulsions also are repaired at the time of surgery in order to maintain an intact extensor mechanism. Fixation methods typically comprise tension band wiring or cannulated screw fixation of the avulsed fragment. For fractures involving the joint, arthroscopy or submeniscal arthrotomy may be considered to address internal derangement.
We describe our preferred surgical technique to address a type III fracture involving the knee joint (fracture extension into the tibial plateau). The described technique can be modified and used for less extensive fracture types.
A midline anterior approach to the knee is performed, with an incision made from the midportion of the patella, centered over the patellar tendon, extending distally to the tibial tubercle. Then the skin and subcutaneous tissues are incised, along with the paratenon over the patellar tendon. The patellar tendon, distal portion of the patella, and the fracture site are exposed at this stage. A medial parapatellar arthrotomy is performed extending down to the fractured fragment of the proximal tibial metaphysis. Subsequently, the fracture is visualized fully, proximally to distally, and throughout the entire fracture site. At this point, a prophylactic anterior compartment release can be performed based on the clinical index of suspicion for impending compartment syndrome. In addition, a visual assessment of soft tissue injury and muscle viability are completed.
After these steps, a tourniquet will be inflated typically. Next, dissection is carried proximally to the proximal tibial plateau (lateral or medial depending on the side to which the fracture extends). A submeniscal arthrotomy is performed and two no. 2 FiberWire sutures are placed through the involved meniscus to retract the meniscus and allow for visualization of the joint surface. At this stage, it can be noted whether there is a cartilaginous defect that requires attention. Once the articular fracture site is cleaned of all hematoma and debris, the fracture can be reduced under direct visualization. Cartilaginous flaps with bony attachments should also be reduced at this point. During this critical step, the goal is primarily anatomic fracture reduction with direct apposition of the fracture at the cartilage surface. The proximal fracture fragment then may be fixed provisionally with two 1.6-mm K-wires.
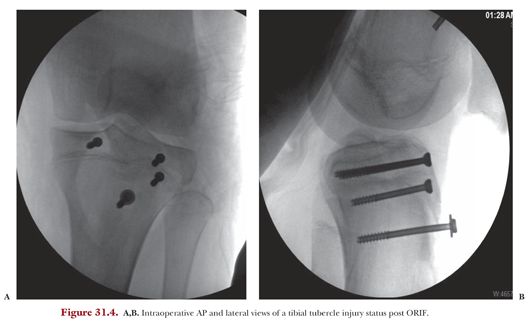
Next, attention can be turned distally to the tibial tubercle fracture fixation. Any remaining alignment and reduction can be performed using a tamp and fluoroscopic guidance. Once appropriate bony alignment is achieved, two 3.5-mm epiphyseal screws are placed under fluoroscopic guidance from anterior to posterior. Both screws should be placed in standard fashion: measured for depth, followed by screw placement. AP and lateral fluoroscopic views then should be used to confirm proper implant position. Next, a third screw of the same size typically is placed more distally through the center of the tibial tubercle, just below the level of the physis. In cases where the patellar tendon is avulsed distally, the distal portion can be secured with suture anchors. Typically, we use DePuy Mitek four-prong suture anchors. These are placed through drill holes in the anterior cortex and tamped into place. Then, the tendon is secured to the bone with the use of four suture strands placed in a simple fashion. At this point, final fluoroscopic views are obtained (Fig. 31.4), and the tourniquet is released in order to identify any active bleeders. The submeniscal arthrotomy is repaired with two no. 2 FiberWire sutures. The median parapatellar arthrotomy is repaired with a 0 vicryl suture. The wound is closed in layers in the usual fashion.