Regarding: “The limited utility of currently available venous thromboembolism risk assessment tools in gynecologic oncology patients” by Drs Barber and Clarke-Pearson. The authors used the American College of Surgeons National Surgical Quality Improvement Program database (ACS-NSQIP) to attempt a validation of the 2005 Caprini Risk Assessment Model among gynecology-oncology patients and concluded that the Caprini score lacks validity in this high-risk patient population. However, consideration of their source data and how it impacts their ability to examine their question deserves merit.
The 2005 Caprini Risk Assessment Model weights individual risk factors to create an aggregate risk score that correlates with postoperative venous thromboembolism (VTE) risk. The Caprini score contains 38 individual risk factors and 3 additional factors for women. These include 16 one-point factors, 8 two-point factors, 10 three-point factors, and 5 five-point factors. ACS-NSQIP lacks data for 5 one-point risk factors (swollen legs, varicose veins, history of abortions, use of oral contraceptives, and inflammatory bowel disease), 3 two-point risk factors (central venous access, patient confined to bed >72 hours, and immobilizing plaster cast), and 9 three-point risk factors (personal history of VTE, family history of VTE, and 7 acquired thrombophilias). Stated differently, ACS-NSQIP lacks data for 17 of 41 risk factors (42% of all risk factors) or 38 of 87 potential points (44% of all points). This profound absence of data makes the authors’ conclusions difficult to accept. Any individualized risk stratification tool must be completed correctly to be useful.
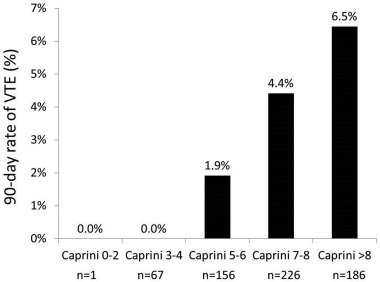
Published validation studies of the Caprini score that include studies in plastic and reconstructive surgery, otolaryngology head and neck, surgical intensive care unit, and general, vascular, and urology surgery patients have identified risk factors rigorously using retrospective chart review or the electronic medical record. Stroud et al studied the 2005 Caprini score in gynecology-oncology patients using scores that were derived from chart review. In that study, 636 patients received no chemoprophylaxis and were risk stratified into accepted strata (Caprini scores. 0–2, 3–4, 5–6, 7–8, and >8) for this letter. Most patients fell into higher risk Caprini strata, and risk for VTE increased as Caprini score increased ( Figure ).