The Changing Environment in Which We Practice Gynecologic Surgery
The Changing Environment in Which We Practice Gynecologic Surgery
Eric J. Bieber
DEFINITIONS
Accountable Care Organization (ACO)—An organization of health care providers (hospitals, providers, and others) that agrees to be accountable for the quality, cost, and overall care of the beneficiaries.
Hospitalist/laborist—Physician/providers who dedicate all or part of their practices to providing care specifically to patients within the hospital.
Institute for Healthcare Improvement (IHI)—A not-for-profit organization founded in 1991 and dedicated to improving health care throughout the globe. Initiated the 100,000 lives campaign (www.ihi.com).
Institute of Medicine (IOM)—Not-for-profit organization chartered in 1970 as part of the National Academy of Sciences to provide unbiased, evidence-based guidance to improve health in the United States (www.iom.com).
Patient Protection and Affordable Care Act (PPACA)—A federal statute approved in 2010 by President Obama and upheld by the Supreme Court in June 2012. The act aims to increase the health insurance coverage for Americans via mandates, subsidies, and tax credits.
Pay for performance (P4P)—A broad construct that attempts to pay providers or health care organizations for achieving predetermined quality thresholds.
Value-based purchasing—Authorized by PPACA, this is a payment method for rewarding quality of care through financial incentives.
As gynecologic surgeons and care providers of women, we have witnessed major changes in our practices over the years. When we think back to our days as medical students and residents, even the youngest of us is able to appreciate the palpable differences that exist today: from how we manage our offices to how we approach diagnostic testing and treatment. Most recently, the passage of the PPACA, the advent of Accountable Care Organizations, and the focus on value and value-based purchasing have begun to rapidly change our external environment.
The cornerstone of the modern practice of medicine continues to be the resounding theme of evidence-based medicine. Quality initiatives from the IHI recommendations, National Committee for Quality Assurance (NCQA), and more recently the efforts of many organizations with the Partnership for Patients as well as many other initiatives have made attempts to promote the safest, most effective care of our patients. Pay for performance and adherence to quality metrics and benchmarks are becoming commonplace. Hospitals have their patient satisfaction scores transparently available for patients to evaluate, and we expect doctor scores to similarly be available in the coming years. We are also being challenged to move from a time when surgical and other treatments were the mainstay of our practice to a new time of screening, prevention, wellness, and the ultimate promise of genomics.
Few of us appreciated how profound a role the computer would play in our daily practice or how this tool might empower us to provide the best possible care in each encounter. The electronic health record (EHR), its implementation and daily use, and its significant benefits and pitfalls will be reviewed in part. We also review the changes that are occurring in medical education from residency to postgraduate training.
We discuss one of the latest trends: a move for at least some physicians, including obstetrician-gynecologists, to choose to function as hospital-based providers or hospitalists. Finally, we review the importance of evaluating evidence-based methodologies for rating our literature.
HEALTH CARE REFORM
The PPACA has profoundly changed the landscape of medicine in the United States. Signed into law in 2010 and upheld by the Supreme Court in 2012, this large body of legislation will continue to impact all care providers for decades to come. Undoubtedly, there will be alteration to the original, but the main tenets of the law are likely to be enacted over the next few years.
Accountable Care Organizations or ACOs had been proposed and piloted in the late 2000s. They are called out specifically within the PPACA, and by law, pilots had to be started. The Centers for Medicare & Medicaid Services (CMS) is the responsible party for overseeing the Medicare Shared Savings Program (MSSP). The Center for Medicare & Medicaid Innovation (CMMI) launched the initial Pioneer ACO program composed of 32 initial ACOs. Since this time, there has been a proliferation of both Medicare ACOs and more recently of commercial ACOs. The main tenet of an ACO is patient-centered care with a view to optimizing care over the continuum including wellness and preventative care. Don Berwick’s triple aims of improving the health of the population, enhancing patient experience, and decreasing cost or improving efficiency are core to ACOs mission. In addition, the MSSP calls out 33 key quality metrics that must be met to share in savings. These metrics are in the four core areas of patient/caregiver experience, care coordination/patient safety, preventative health, and care of at-risk populations. A different variation on patientcentric care is the advent of the patient-centered medical home (PCMH). NCQA has defined the PCMH as a “health care setting that facilitates partnerships between individual patients, and their personal physicians, and when appropriate, the patient’s family. Care is facilitated by registries, information technology, health information exchange (HIE), and other means to assure that patients get the indicated care when and where they need and want it in a culturally and linguistically appropriate manner.”
Additional changes brought about through PPACA include the introduction of “value-based purchasing” where providers are either rewarded or penalized for their efforts relative to quality and efficiency. Discussed in more detail later, this is a true pay-for-performance program. Bundled payment demonstrations are also called out in the legislation and aim to better align providers, hospitals, and others to work together to optimize care over the continuum by providing a single payment for an entire episode of care. The issue of readmissions has also been brought to the forefront with penalties now beginning for many hospitals. Also, key to the PPACA is the expansion of Medicaid by many states and the formation of health care exchanges with the goal of providing health care coverage to the majority of the citizens of the United States. The details of many of these issues remain to be worked out as of the time of this writing and are outside the scope of this chapter. Indeed, many states have chosen to opt out of Medicaid expansion in 2015, and health exchanges have largely only been attempted in Utah and Massachusetts. The true impact on health care at an individual level as well as a population level remains to be seen. Other issues such as the physician and nursing workforce required to care for the additional millions of individuals who will now have health care coverage continue to be hotly debated topics.
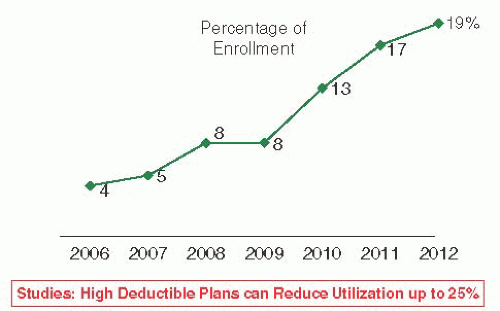
FIGURE 5.1 Increasing enrollment in high-deductible health plans. Data from Towers Watson. 2012 health care changes ahead survey report. http://www.towerswatson.com/DownloadMedia. aspx?media={24F68B2F-90F6-48C9-ADF3-CA61A378300A}. Published on October 2012.
Another evolving area is the increase in high-deductible or consumer-driven health plans (Fig. 5.1 and Table 5.1). Because of the ever-increasing cost of health care premiums, many companies and employees have chosen to accept the potential of greater out-of-pocket expense for the concomitant reduction in health insurance premiums. The outcome of patients having to pay these “first dollar amounts” to providers is more and more patients asking about the cost of visits, surgeries, and radiologic studies. Given the complexities of charges and billings, this may be challenging for many organizations. This advent of consumerism in health care is consistent with the government’s desire to increase transparency of both quality and pricing in an effort to increase the value for patients. With the significant increase in the number of these plans across the country, the issues of cost, access, and transparency of information are likely to become of even greater interest for patients.
TABLE 5.1 High-Deductible Health Plan: National Enrollment
2012 DATA BY STATE
TOTAL ENROLLMENT IN HIGH-DEDUCTIBLE HEALTH PLANS
California
1,002,000
Texas
755,000
Illinois
717,000
Ohio
663,000
Florida
540,000
New York
495,000
Minnesota
487,000
Pennsylvania
406,000
Source: Buck K. Health savings accounts and account-based health plans: research highlights. America’s Health Insurance Plans (AHIP) Center for Policy and Research. http://www.ahip. org/HSAHighlightsReport072012/. Published on July 2012.
QUALITY INITIATIVES
In 2010, Daniel Levinson of the Office of the Inspector General of the Department of Health and Human Services released a report on safety issues for Medicare beneficiaries. After evaluation of numerous patient records, including review by multiple physicians, the report concluded that 13.5% of hospitalized Medicare patients experience at least one adverse event during a hospitalization. An additional 13.5% of all patients experienced an event that led to temporary harm. In the subsequent review by physicians, they noted that 44% of these events were preventable. The total yearly cost estimate appeared to be close to $4.4 billion.
Few clinicians would argue that quality is the most important parameter in health care today. Yet, it is becoming ever more evident that many patients do not receive state-of-theart health care. In a landmark article published in 2006, Asch et al. from the Rand Health group evaluated 30 chronic and acute conditions and used 439 indicators of quality to access if patients had received appropriate care. Unfortunately, overall, only 54.9% of patients received what would be considered recommended care. Some sociodemographic differences existed: Women received 56.6% of care versus men at 52.3%, and those with annual household income greater than $50,000 received 56.6% versus those less than $15,000 at 53.1%. However, what is striking is the low level of achieving recommended care for all the groups studied regardless of the sociodemographic differences.
In 1999, the IOM released a report suggesting that 98,000 patients per year die secondary to inadequate care being rendered. Many subsequent debates ensued regarding the methodologies used to attain these numbers. However, this report created a call to arms, challenging those individuals and organizations who provide care to improve the quality of care delivered to all patients. Furthermore, it has caused a number of initiatives from a broad base of organizations. In December 2004, the IHI, at its 16th Annual National Forum on Quality Improvement in Health Care, announced a goal to save 100,000 lives by June 2006. The campaign invited all US hospitals to join in implementing six broad initiatives that have demonstrated efficacy in well-performed clinical trials. These include
Prevention of surgical site infections
Prevention of ventilator-associated pneumonia
Prevention of central line infections
Prevention of adverse drug events (ADEs) through medication reconciliation
Deployment of rapid response teams
Delivery of evidence-based care for acute myocardial infarction
What is particularly impressive about the IHI campaign is the extent of support across a broad range of disparate federal, state, political, and private organizations, including—but not limited to—the CMS, Veterans Health Administration, American Medical Association, American Nurses Association, Centers for Disease Control and Prevention, Joint Commission on Accreditation of Healthcare Organizations, the Leapfrog Group, and multiple others.
Ultimately, the IHI released information suggesting that these initiatives were able to save 122,300 patients. This was good news and suggested that progress was indeed being made. Unfortunately, a more recent publication reviewed hospital admissions from 2002 to 2007 in North Carolina hospitals. The authors found a rate of 25.1 harms per 100 admissions with no statistical change over the 5 years of the study. The challenge to implement the IHI recommendations as well as multiple other quality initiatives has caused a number of hospitals and large organizations to create chief quality officer positions that are largely responsible for implementing and monitoring compliance to these programs. In essence, this may be the confluence of patient safety, performance improvement, utilization review, and other previous orphan committees.
Consistent with the IHI initiatives, other initiatives have come from CMS, including recommendations for optimization of diabetic patients. These include bundles of care much like the IHI central line bundle, in which appropriate care consists of all elements being appropriately performed or delivered within the correct time frame. Unfortunately, as the bundles become more complicated, it becomes more and more difficult for the provider to remember what has or has not been done. This may be yet another opportunity for the EHR to allow both the clinician and the patient to know what tests or interventions need to be performed, thus optimizing the encounter. The Joint Commission has also continued to evolve its recommendations, including core measure sets for venous thromboembolism, the surgical care improvement project, and most recently a core measure set for perinatal care. In addition, there continue to be updates and new releases of National Patient Safety Goals (Table 5.2). We expect that with increasing evidence-based knowledge, many additional quality-driven initiatives will come forward.
Another key safety initiative is the Partnership for Patients, a public-private partnership that aims to improve quality, safety, and affordability. An amazing 3,700 hospitals have signed on to portions of this program whose two primary goals are the reduction of hospital-acquired infections by 40% by the end of 2013 (as compared to 2010) and reducing complications using care transitions to effect a 20% reduction in hospital readmissions. Twenty-six hospital engagement networks were awarded $218 million to lead these efforts. The patient safety areas of focus include (but are not limited to) the following (many of which an obstetrician-gynecologist may encounter):
Adverse drug events
Catheter-associated urinary tract infections
Central line-associated bloodstream infections
Injuries from falls and immobility
Obstetrical adverse events
Pressure ulcers
Surgical site infections
Venous thromboembolism
Ventilator-associated pneumonia
Readmissions
TABLE 5.2 2013 Hospital National Patient Safety Goals
Identify patients correctly
NPSG.01.01.01
Use at least two ways to identify patients. For example, use the patient’s name and date of birth. This is done to make sure that each patient gets the correct medicine and treatment.
NPSG.01.03.01
Make sure that the correct patient gets the correct blood when they get a blood transfusion.
Improve staff communication
NPSG.02.03.01
Get important test results to the right staff person on time.
Use medicines safely
NPSG.03.04.01
Before a procedure, label medicines that are not labeled, for example, medicines in syringes, cups, and basins. Do this in the area where medicines and supplies are set up.
NPSG.03.05.01
Take extra care with patients who take medicines to thin their blood.
NPSG.03.06.01
Record and pass along correct information about a patient’s medicines. Find out what medicines the patient is taking. Compare those medicines to new medicines given to the patient. Make sure the patient knows which medicines to take when they are at home. Tell the patient it is important to bring their up-to-date list of medicines every time they visit a doctor.
Prevent infection
NPSG.07.01.01
Use the hand cleaning guidelines from the Centers for Disease Control and Prevention or the World Health Organization. Set goals for improving hand cleaning. Use the goals to improve hand cleaning.
NPSG.07.03.01
Use proven guidelines to prevent infections that are difficult to treat.
NPSG.07.04.01
Use proven guidelines to prevent infection of the blood from central lines.
NPSG.07.05.01
Use proven guidelines to prevent infection after surgery.
NPSG.07.06.01
Use proven guidelines to prevent infections of the urinary tract that are caused by catheters.
Identify patient safety risks
NPSG.15.01.01
Find out which patients are most likely to try to commit suicide.
Prevent mistakes in surgery
UP.01.01.01
Make sure that the correct surgery is done on the correct patient and at the correct place on the patient’s body.
UP.01.02.01
Mark the correct place on the patient’s body where the surgery is to be done.
UP.01.03.01
Pause before the surgery to make sure that a mistake is not being made.
The purpose of the National Patient Safety Goals is to improve patient safety. The goals focus on problems in health care safety and how to solve them.
Because of the breadth of the Partnership for Patients effort and the collaborative nature of the learning, there is real hope that sustainable change may be able to be accomplished.
It was previously believed that organizations with higher caseloads of a particular disease might be better positioned to deliver recommended care. Lindenauer et al. studied this tenet as it relates to pneumonia in the acute care setting. Surprisingly, they found both hospitals and physicians who had a higher caseload of pneumonia patients actually had reduced adherence to recommended guidelines—such as influenza and pneumococcal vaccine administration or early antibiotic administration—and had no better outcomes.
Quality initiatives are currently being led by a number of organizations, including some physician groups. For example, in Washington State, a physician-led group has brought all hospitals to the table to evaluate discrete performance measures regarding cardiac revascularization. Similarly, the California Perinatal Quality Care Collaborative in 1998 targeted improving antenatal steroid use as an initiative. They accumulated baseline data, developed educational materials, and broadly disseminated this information. They concluded that regional collaboration allowed an improvement from a baseline rate of administration of 76% to 86% post implementation. Callcut and Breslin discuss how private groups, such as the Leapfrog Group, are playing an important role in moving the private regulatory movement forward and suggest that surgeons need to become more active participants in this process of reshaping and redefining our future.
How to best implement quality improvement programs in a given setting is also continuing to be investigated. A recent evaluation of hospital quality improvement implementation and subsequent impact on discrete patient-safety metrics suggested that involvement by multiple units within a hospital might have a negative impact on results. Alternatively, having a higher percentage of physicians involved was associated with better scores on at least two of the four safety indicators. Interestingly, having a higher percentage of hospital staff or senior management involved had no impact on any of the indicators.
TABLE 5.3 Key Steps for Initiating, Improving, Evaluating, and Sustaining a Quality Improvement Program
Initiating or improving a quality improvement program
1.
Do background work: Identify motivation, support teamwork, and develop strong leadership.
2.
Prioritize potential projects and choose the projects to begin.
3.
Prepare for the project by operationalizing the measures, building support for the project, and developing a business plan.
4.
Do an environmental scan to understand the current situation (structure, process, or outcome), the potential barriers, opportunities, and resources for the project.
5.
Create a data collection system to provide accurate baseline data and document improvement.
6.
Create a data reporting system that will allow clinicians and other stakeholders to see and understand the problem and the improvement.
7.
Introduce strategies to change clinician behavior and create the change that will produce improvement.
Evaluating and sustaining a quality improvement program
1.
Determine whether the target is changing with ongoing observation, periodic data collection, and interpretation.
2.
Modify behavior change strategies to improve, regain, or sustain improvements.
3.
Focus on sustaining interdisciplinary leadership and collaboration for the quality improvement program.
4.
Develop and sustain support from the hospital leadership.
Most clinicians have not been trained in how to develop and implement quality improvement programs. Curtis et al. have published a how-to paper that came out of an outcomes task force of the Society of Critical Care Medicine but has wide applicability to many areas of medicine (Table 5.3). The generalized lack of education and training in quality may explain some of the lethargy that Leape and Berwick allude to in their article “Five Years after To Err Is Human: What Have We Learned?.” They suggest that extraordinary quality improvements have been achieved by implementing discrete strategies in specific environments. If each of our organizations could fractionally achieve similar success, the impact on patient care might be quite remarkable.
PAY FOR PERFORMANCE
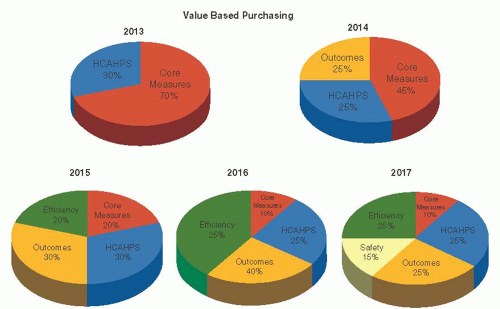
In many settings, multiple quality measures are being subjected to pay for performance, with groups achieving higher levels of patient compliance being awarded higher levels of reimbursement. This is a marked change from being paid for delivery of units of health care or procedures in which disease states are being managed. As of 2013, 100s of pay-forperformance initiatives have been started by a wide variety of sponsors, ranging from employers to the federal government. The most important current pay-for-performance effort is the value-based purchasing program sponsored by CMS. In this program, up to 2.0% of a hospital’s base-operating diagnosis related group (DRG) payments will be at risk (Table 5.4). CMS calculates the incentive adjustment based on a total performance score achieved by the hospital. The program is structured to allow a continual evolution with measures and weighting changing each year. Because almost $1 billion dollars is at risk, many organizations have highly focused efforts around the measures. As can be seen, CMS is moving from a time when surrogate measures, such as core measures, were the key drivers to outcomes and efficiency metrics (Fig. 5.2 and Table 5.5). The PPACA also required a Hospital-Acquired Condition (HAC) Reduction Program with another potential 1% payment reduction if performance thresholds are not met. Currently, there are eight measures in two domains, but these will likely increase over time (Table 5.6). In addition, many of these measures have applicability for obstetrician-gynecologists. The final major pay-forperformance program is aimed at reducing readmissions. In this program, payments are again reduced (1% in 2013, 2% in 2013, and 3% in 2015 and beyond) if readmission rates exceed the expected level. While the initial disease states being evaluated are acute myocardial infarction, pneumonia, and heart failure, all Medicare discharges are penalized. Reviewing Figure 5.3 demonstrates the significant potential for hospital revenue reductions as all of these programs are phased in.
TABLE 5.4 Amount Available Each Year Controlled by Statute
2013
1.00% of base-operating DRG payments
2014
1.25%
2015
1.50%
2016
1.75%
2017
2.00%
In an early article on the subject of paying for high-quality care, Epstein et al. called for several significant changes to facilitate adoption of pay-for-performance initiatives. These recommendations included an expansion in the scope of the efforts, as well as the amount of incentive available to the clinician or group; the importance of large groups such as CMS becoming involved; an expansion from the current small cadre of clinical indicators; an improvement in our ability to establish reliable metrics for evaluation of quality; and, finally, a call for investment in electronic infrastructure to facilitate all of the above.
A Cochrane systematic review of the subject of targeted payments to affect outcomes in primary care was unable to reach a conclusion because of limitations in prior study quality and power. Kouides et al. evaluated the use of financial incentives to increase rates of influenza vaccine administration and found that modest incentive increased an already high baseline administration rate. In another study on immunizations, Fairbrother et al. evaluated use of cash bonus, enhanced fee for service, and feedback for improving baseline vaccination rates. They found only the bonus group statistically improved (increased by 25.3%), although they believed much of this effect was due to better documentation versus actual increased administration of vaccine. Roski et al. noted that in incentivized groups, documentation of tobacco use was markedly increased, as was accession to counseling programs. Unfortunately, other important clinical end points showed no difference.
FIGURE 5.2 Evolution of value based purchasing from 2013 to 2017.
Only gold members can continue reading. Log In or Register to continue