
Before proceeding, confirm that both guide wires are in the correct position. Measure the diameter of the quadruple hamstring graft using tendon sizers; these grafts typically range from 6 to 8 mm in diameter. Because a tight fit is essential, use the smallest reamer possible to ream over the guide wires. Chamfer the edge of the femoral hole intra-articularly, and measure the width of the lateral femoral condyle. Choose an EndoButton continuous loop (Acufex, Smith & Nephew, Memphis, TN; 2 to 3 cm) that allows 1.5 to 2 cm of the quadruple hamstring graft to remain within the lateral femoral condyle. Pass the EndoButton continuous loop around the middle of the double tendons, and loop it inside itself to secure the tendons. This will shorten the length of the EndoButton continuous loop substantially. An alternative method is to place the tendons through the continuous loop before suturing the tendons together. This method requires drilling and measuring the length of the femoral hole to determine the appropriate length of the EndoButton continuous loop before the graft is prepared.
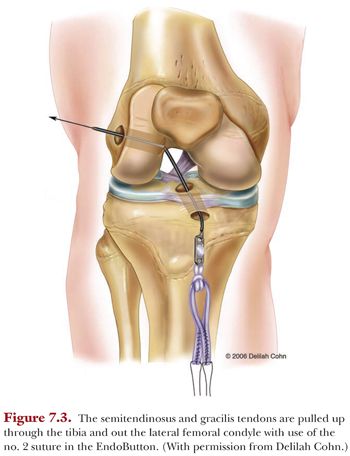
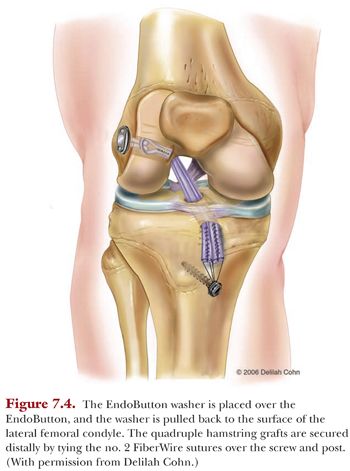
In one end of the EndoButton, place a no. 2 FiberWire suture. Pass the suture from anterior to posterior through the tibia and out the lateral femoral condyle using a suture passer. Then pull the EndoButton and tendons up through the tibia and out the femoral hole using the suture (Fig. 7.3). Place an AO washer that is 3 to 4 mm larger than the femoral hole over the EndoButton. Apply tension to the tendons distally and pull both the EndoButton and the washer to the surface of the lateral femoral condyle. The washer anchors the graft proximally, so the EndoButton does not get pulled through the hole in the lateral femoral condyle. Place the graft under tension and extend the knee to arthroscopically ensure that the graft is not impinging on the intercondylar notch. It is usually unnecessary to perform an anterior notchplasty when performing transepiphyseal ACL reconstruction; however, a small area of the anterior intercondylar notch may be removed if it comes in contact with the graft in terminal extension. Place the knee in 20 degrees of flexion and secure the quadruple hamstring graft distally by tying the no. 2 FiberWire sutures over a 4.5- × 25-mm long cancellous screw and post (Smith & Nephew) located medial to the tibial tubercle apophysis and distal to the proximal tibial physis (Fig. 7.4). Close the subcutaneous tissue and skin using standard technique.
Modified Anderson Technique—All-Epiphyseal Anterior Cruciate Ligament Reconstruction
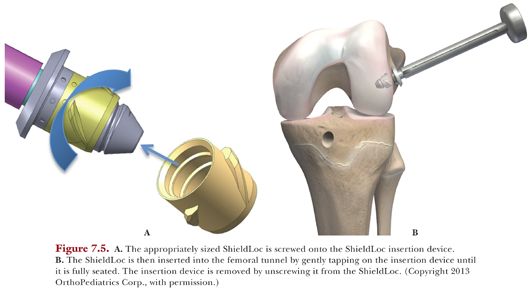
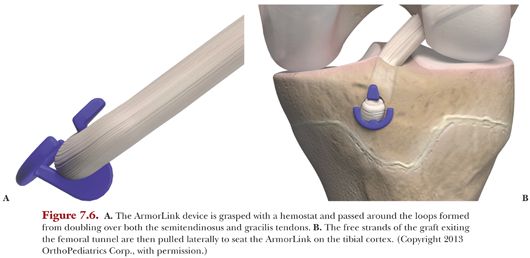
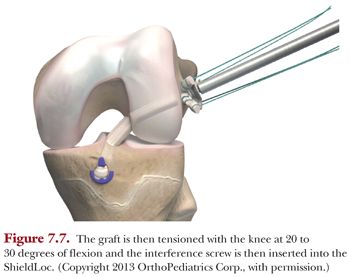
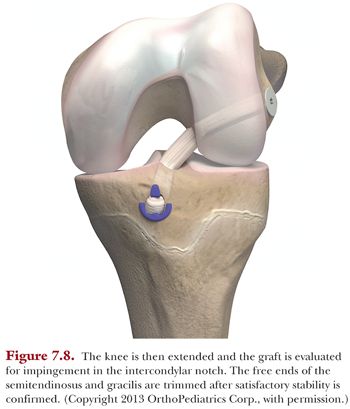
The setup of the room, diagnostic arthroscopy, harvesting and preparing the grafts, insertion of the guide wires, and drilling the holes in the tibial and femoral epiphyses is performed just as described in the transepiphyseal technique. However, the OrthoPediatrics set has all of the necessary instrumentation to perform each step. After drilling the tibial and femoral holes, it is necessary to insert the ShieldLoc sleeve into the femoral hole. Insert the counter bore reamer into the femoral hole until it bottoms out on the lateral femoral cortex. During this step, the counter bore is inserted to a depth of 8 mm and increases the diameter of the femoral hole by 2 mm. The small amount of bone removal occurs rapidly. Retract the iliotibial band and carefully remove the soft tissue immediately around the hole to allow for clear placement of the ShieldLoc. The appropriately sized ShieldLoc sleeve is screwed on to the insertion device (Fig. 7.5A) and then gently tapped into the femoral tunnel (Fig. 7.5B). The fluted fins on the outside of the ShieldLoc sleeve prevent the device from backing out of the femoral tunnel while removing the insertion device. The ShieldLoc sleeve is designed to protect the physis from radial pressure caused by the insertion of the interference screw. After the ShieldLoc sleeve has been inserted, place the Graft Passer from the Disposable Kit through the femoral tunnel and with an arthroscopic grasper; pull the Graft Passer loop out of the tibial tunnel. Place one end of each graft through the Graft Passer loop on the femoral side. Then pull the tibial end of the Graft Passer, bringing the graft through the femoral tunnel into the tibial tunnel. Gently pull 1 to 2 cm of the graft loop outside of the anterior tibial cortex to allow installation of the ArmorLink implant. With the use of hemostat, pass the ArmorLink around the tendons (Fig. 7.6A). Pull on the free strands of the graft coming out of the femoral tunnel in order to seat the ArmorLink on the tibial cortex (Fig. 7.6B). The ArmorLink may be positioned in any orientation. Observe the ShieldLoc when pulling the free strands of the graft to make sure the ShieldLoc sleeve does not catch on the sutures in the free ends of the graft and become displaced. If the ShieldLoc sleeve moves when pulling the tendons through, then stabilize the ShieldLoc sleeve with a hemostat to prevent displacement. With the knee in approximately 20 to 30 degrees of flexion, apply tension with the graft tensioner and insert the screw of the ShieldLoc (Fig. 7.7). Evaluate the graft for intercondylar notch impingement and then close the wound in a standard fashion (Fig. 7.8). The postoperative rehabilitation is the same with this technique as for the transepiphyseal technique.
Postoperative Rehabilitation for Transepiphyseal or All-Epiphyseal Anterior Cruciate Ligament Reconstruction
Postoperative rehabilitation following the transepiphyseal ACL reconstruction procedure has three phases. Phase I begins when the patient awakens from surgery. Encourage the patient to perform straight-leg raises and to contract the quadriceps muscles. Use cryotherapy for 5 to 10 minutes each hour. The day after surgery, the patient performs range-of-motion exercises and hamstring stretches in a prone position. Patients without meniscal repairs may ambulate with crutches and partial weight bearing for 4 weeks. For patients who required meniscal repair, only toe-touch weight bearing is allowed for the first 6 weeks. The 1-week postsurgical goal is to have a range of motion of 0 degrees of extension to 90 degrees of flexion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


