pediatric spine and the vertebral subluxation complex (VSC; i.e., positional dyskinesia).
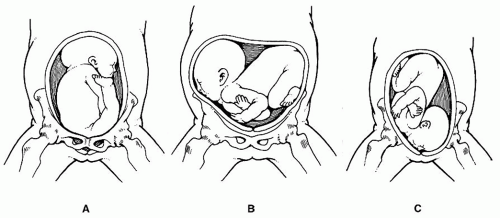 FIGURE 5-1 A: Breech presentation. Notice the position of the legs. Modified from Graham JM. Smith’s recognizable patterns of human deformation (2nd ed). Philadelphia, PA: W.B. Saunders Co., 1988; p. 86. B: Transverse lie presentation. Modified from Graham JM. Smith’s recognizable patterns of human deformation (2nd ed). Philadelphia, PA: W.B. Saunders Co., 1988; p. 95. C: Face presentation. Modified from Graham JM. Smith’s recognizable patterns of human deformation (2nd ed). Philadelphia, PA: W.B. Saunders Co., 1988; p. 96. |
result in extension or flexion trauma to the occiput and cervical and upper thoracic regions.
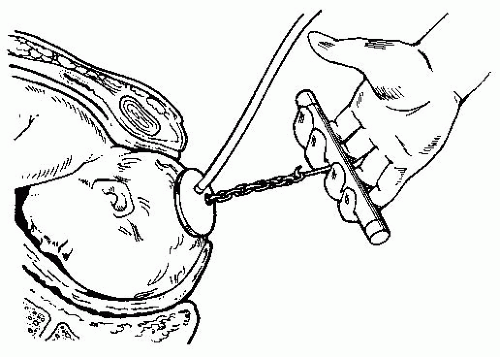 FIGURE 5-2 Bird’s modification of Malmstrom’s vacuum extractor method. Modified from Pernoll ML, Benson RC. Current obstetric and gynecologic diagnosis and treatment. 6th ed. Norwalk, CT: Appleton & Lange, 1987; p. 496. |
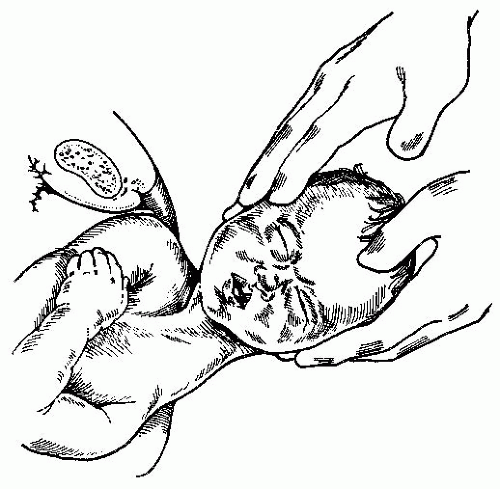 FIGURE 5-3 Delivery with upward traction applied to the head to deliver a posterior shoulder over the perineum. Modified from Wilson JR, Beecham CT, Forman I, Carrington ER (eds). Obstetrics and Gynecology. St. Louis, MO: CV Mosby, 1958; p. 336. |
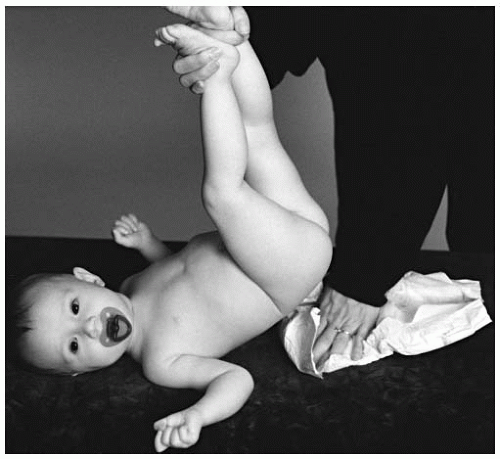 FIGURE 5-4 Certain diapering techniques may place unnecessary stress on the spine. |
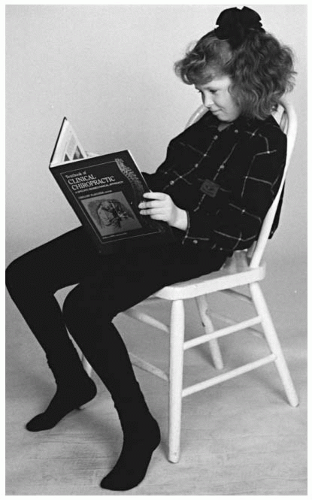 FIGURE 5-5 Poor design and use of school chairs places repetitive stress on the developing spine. |
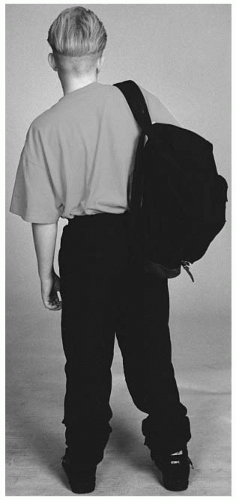 FIGURE 5-6 Asymmetrical usage of the backpack places repetitive stress on the musculoskeletal system. |
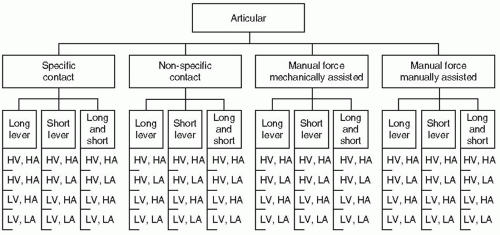 FIGURE 5-7 Articular procedure descriptions. H, high; L, low; V, velocity; A, amplitude. Modified from Bartol KM. A model for the categorization of chiropractic treatment procedures. Chiropr Tech 1991;3:79. |
tenderness. Introducing forces into a hypermobile or normally functioning joint is contraindicated.
is susceptible to the introduction of rotation by poor upper torso stabilization (Fig. 5-13A,B) and excessive leaning or “kicking down” on the superior bent leg. Several general mobilization techniques are dangling or holding infants in the air either by their feet, under the axilla, or with hands wrapped around the thoracic spine, followed by a random snap, shake, or whip to the spine (Fig. 5-14).
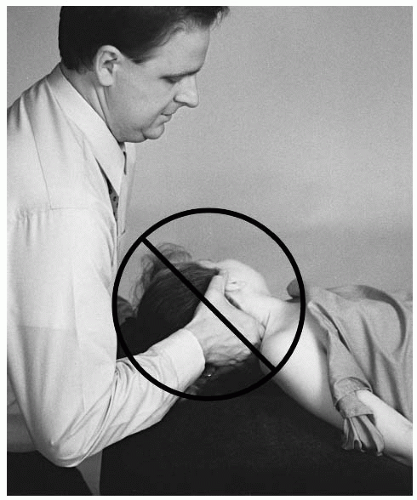 FIGURE 5-8 To pre-load the joint for the supine rotary break, it is necessary to position the cervical spine in extension and Y-axis rotation. |
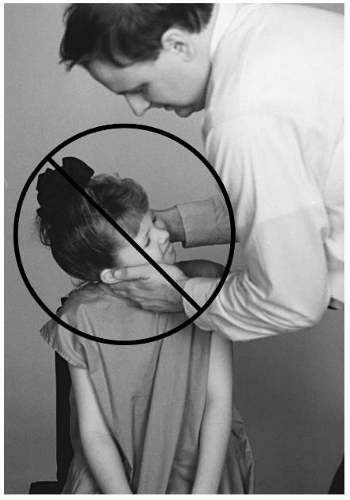 FIGURE 5-9 Long lever techniques are contraindicated for the pediatric spine. |
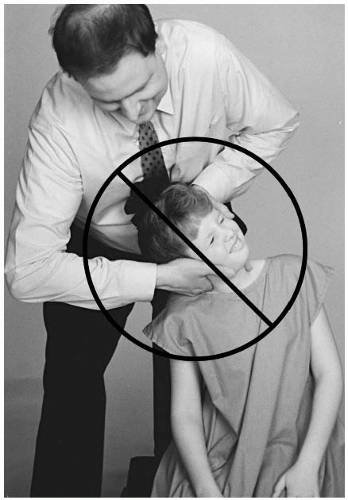 FIGURE 5-10 Lateral flexion with rotation places undue stress on the spinal elements. |
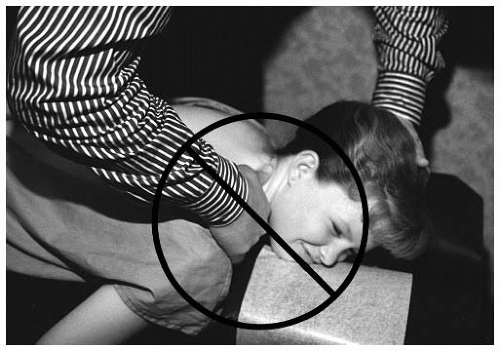 FIGURE 5-11 The diversified thumb move introduces unnecessary Y-axis rotation. |
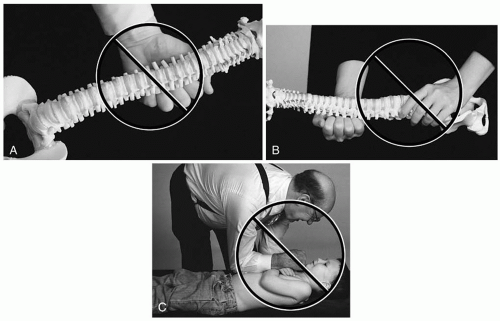 FIGURE 5-12 A-C: The anterior thoracic adjustment is a non-specific manipulation for the developing spine. The doctor overcontacts the spine and ribs. |
hand positions (e.g., pisiform, thenar eminence, the length of the digit) may be too large and contraindicated for the smaller pediatric spine. The possibility of overlapping several spinal segments, or on to the ribs in the case of a thoracic contact, is likely with traditional contact hand set-ups (Fig. 5-15).
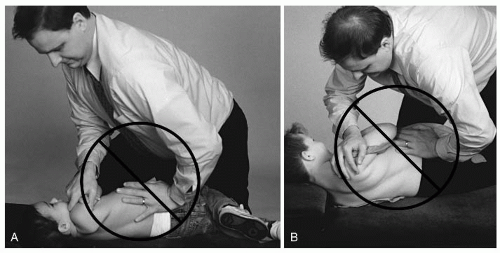 FIGURE 5-13 A,B: Torso rotation introduces unnecessary forces into multiple spinal units. |
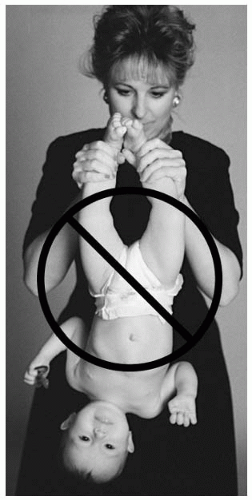 FIGURE 5-14 Dangling the infant by the ankles to perform a whipping movement of the spine is contraindicated. |
by the deceleration, which results in the actual adjustive force produced by the doctor-patient impact.
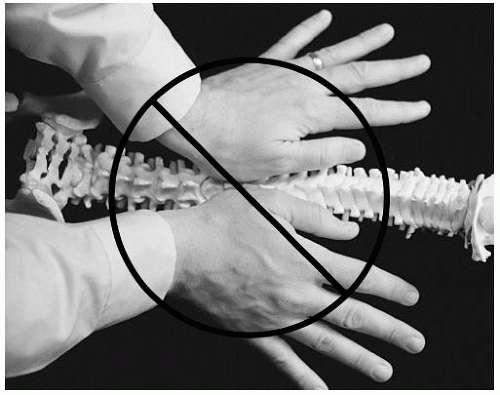 FIGURE 5-15 Overlapping several spinal segments may occur with a traditional hand contact. |
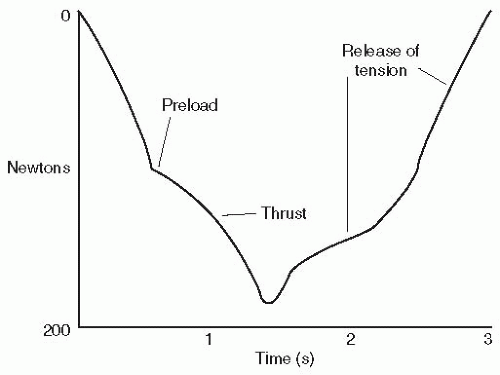 FIGURE 5-16 A qualitative graph of a set-hold type of adjustment thrust. |
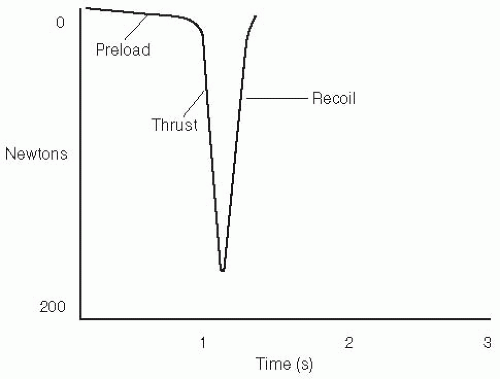 FIGURE 5-17 A qualitative graph of a toggle-recoil type of adjustment thrust. |
patient should be in a plane horizontal to the floor. A skull in a superior head tilt may indicate an AS (-θX) condyle. The PS (+θX) condyle will result in the head tilted inferiorly. The newborn, with underdeveloped cervical musculature, is difficult to inspect for postural abnormalities.
 FIGURE 5-18 The fifth digit is placed on the posterior-inferior aspect of the occiput. |
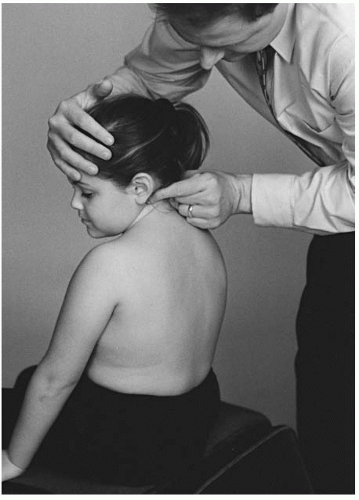 FIGURE 5-19 Motion palpation of the occiput. |
the paraspinal skin temperature instruments (35). To prevent the formation of air gaps at the skin and thermocouple interface, the probes are maintained in perpendicular contact with the skin surface using sufficient pressure. The scanning glide is caudad to cephalad for T2-C0 and cephalad to caudad for T2-S2 (S3 in the smaller patient). The nonamplified instrument should have a glide speed that does not exceed 0.5 to 1.0 cm/s (37). To confirm a suspected temperature differential at a segmental level, the scan should be repeated several times. The accentuated differentials with a repeated scanning procedure are considered more significant than those that diminish. The validity of the procedure is decreased when the existence of moles or other lesions (e.g., blemishes, scar tissue, cysts) are in the path of the instrument glide. The glide and orientation of the instrumentation is modified for the presence of spinal curvature (i.e., scoliosis). Because of the rolling, loose skin of the newborn/infant, any positive findings must be substantiated with other objective findings (e.g., tenderness or edema).
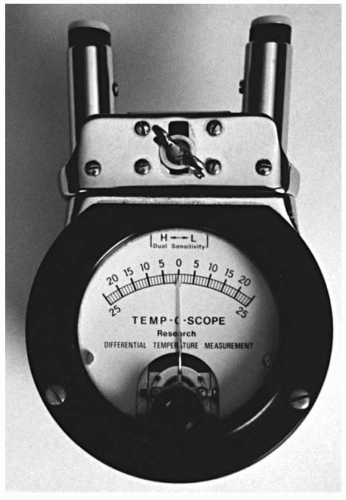 FIGURE 5-20 The Temp-o-scope. |
TABLE 5.1 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
assessment can be further substantiated with stress radiographic studies in flexion and extension and clinical assessments (Fig. 5-21).
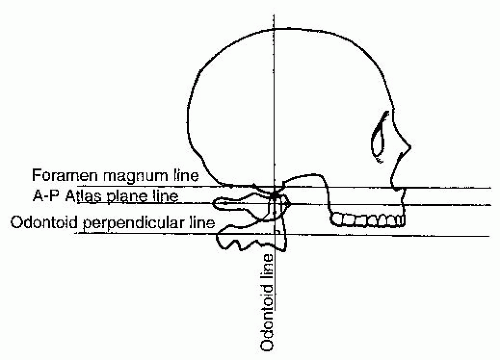 FIGURE 5-21 Relatively normal alignment of C0-C1. Modified from Herbst RW. Gonstead Chiropractic Science and Art Mt. Horeb, WI: Sci-Chi Publications, 1968; p. 133. |
TABLE 5.2 | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
occiput and create a slight separation from the atlas. The thrust is an arcing anterior to posterior and slightly superior to inferior movement. Laterality (e.g., PSLS, PSRS) is corrected by the doctor’s contact. To correct condyle rotation, the infant’s head is pre-positioned with slight rotation before the thrust. For posteriority (e.g., PSLSLP, PSRSRP), the head is slightly rotated away from the contact hand (Fig. 5-26). The anterior listing of PSLSLA or PSRSRA is pre-positioned with slight head rotation toward the side of the doctor’s contact hand (Fig. 5-27).
 FIGURE 5-22 The condyle block comes in a variety of sizes to accommodate the cervical spine. |
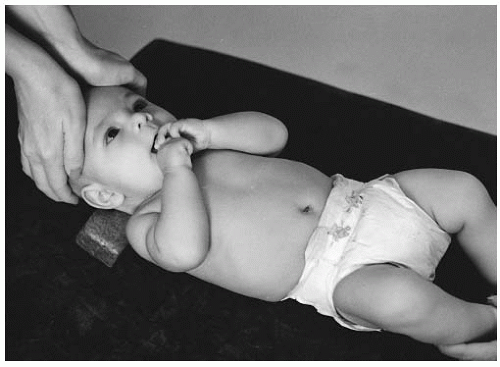 FIGURE 5-23 The thenar eminences contact the glabella for the anterior-superior occiput. |
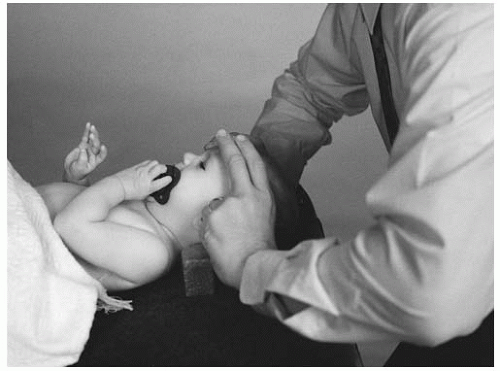 FIGURE 5-24 Fingers on the glabella with the thumbs wrapped around the posterior occiput. |
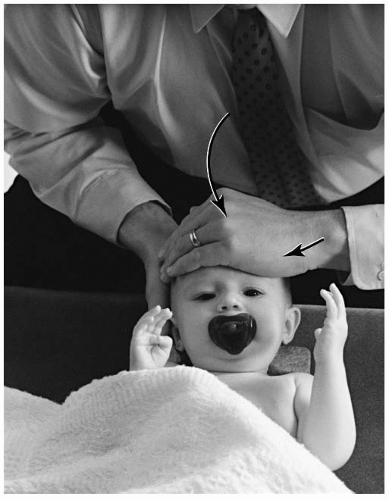 FIGURE 5-25 Single hand contact for an ASLS listing. The condyle block is used for all supine AS set-ups. |
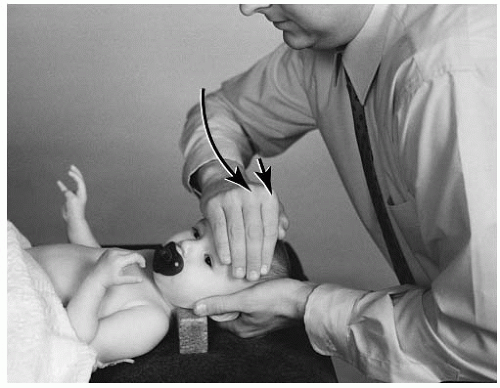 FIGURE 5-26 Slight head rotation of the infant’s head away from the contact hand will correct the axial rotation in an ASRSRP listing. |
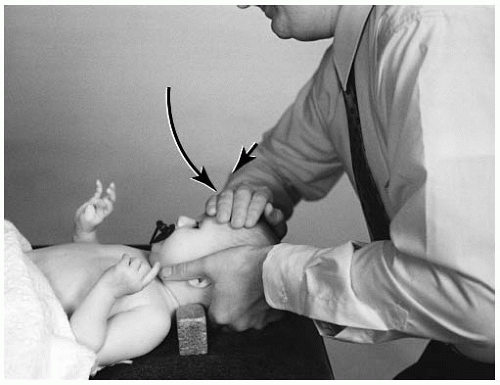 FIGURE 5-27 On the lateral side of occiput the doctor will squat or kneel behind the bench, contacting the glabella of the frontal bone on the side of laterality of the listing. The opposite hand will cup the posterior occiput and slightly lift to separate the occipito-atlantal joint. Head rotation toward the contact hand positions the infant for an ASRSRA listing. |
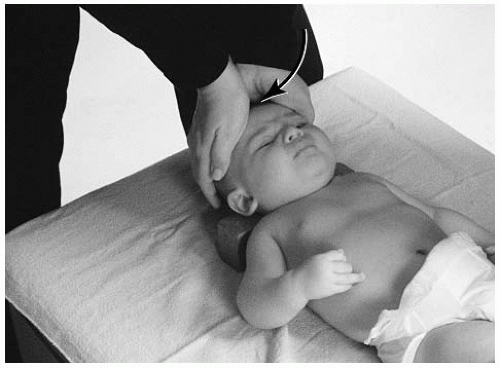 FIGURE 5-28 Supine AS condyle adjustment. Both thenar eminences are placed on the contact site. The fingers of both hands are wrapped around posterior to the occiput creating a slight lift. The doctor’s elbows should stay close to the side of the body. |
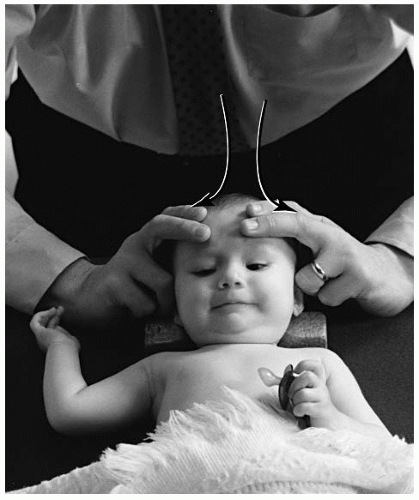 FIGURE 5-29 Supine AS condyle adjustment. Place the second and third digits of both hands on the contact site, the thumbs are wrapped around posteriorly to the occiput creating a slight lift. The doctor’s elbows should stay close to the side of the body. |
booster chair) may be used on the adjusting chair. The condyle block will be positioned behind C1-C7 and held there with the doctor’s abdomen (Fig. 5-31). The stabilization strap or the parent’s hand can also be placed on the child’s abdomen and chest to further stabilize the patient. For an AS listing, the flat palm of the doctor’s hand will contact the center of the glabella and supra orbital margin. The opposite hand will overlap the contact hand for stabilization (Fig. 5-32). An alternative set-up is for the doctor to interlink his or her fingers (Fig. 5-33). Pre-tension at the joint is obtained with slight head flexion. Before the thrust, the doctor’s elbows should be positioned close to the side of his or her body. This will provide for a smoother glide during the arc of the adjustment. Laterality is corrected by the doctor standing slightly toward the side of listing. The contact hand for a lateral misalignment (e.g., ASRS, ASLS) is the same hand as the side of listing. Condyle rotation (e.g., ASRSRP, ASLSLA) is corrected when the doctor pre-positions the head. For anteriority, the head is slightly rotated to the side of the contact hand (Fig. 5-34). Posteriority is corrected with slight head rotation away from the contact hand (Fig. 5-35).
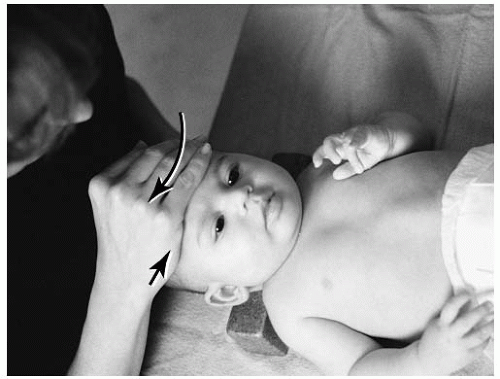 FIGURE 5-30 The doctor squats on the side of laterality, placing the right thenar eminence on the contact site for the ASRS listing. The stabilization hand is wrapped around the occiput, creating a slight lift. The doctor’s elbows should stay close to the side of the body. |
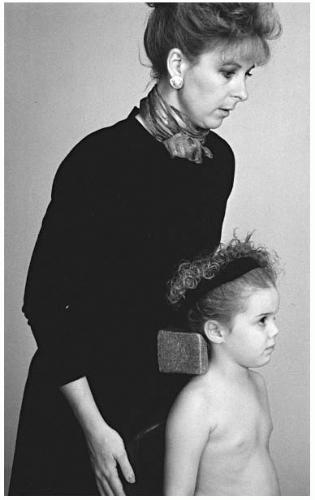 FIGURE 5-31 The condyle block is placed behind the patient’s C1-C7 spine. The doctor’s abdomen will hold the block. |
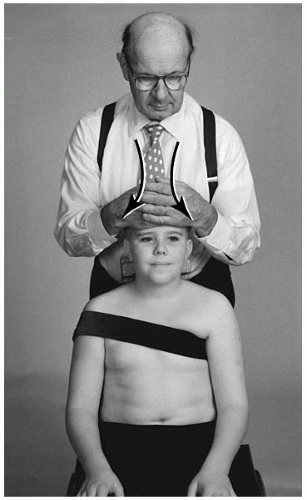 FIGURE 5-32 For the AS listing, the flat palm of the doctor’s hand contacts the center of the glabella, and the opposite hand will overlap the contact hand. |
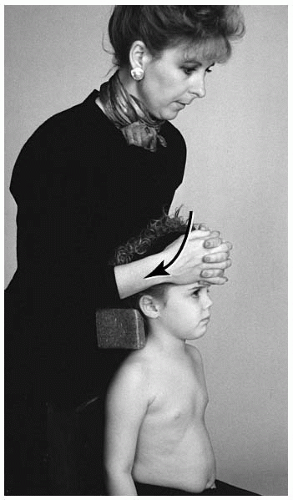 FIGURE 5-33 An alternative AS set-up is for the doctor to interlink his or her fingers. |
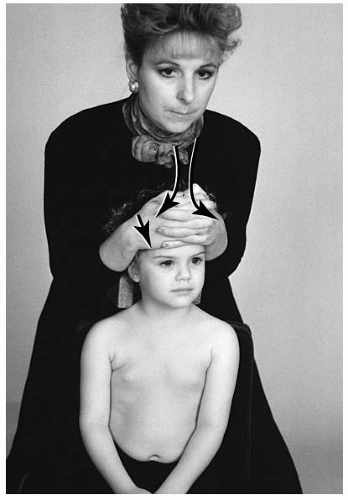 FIGURE 5-34 For the ASLSLA listing, the head is rotated to the side of hand contact. |
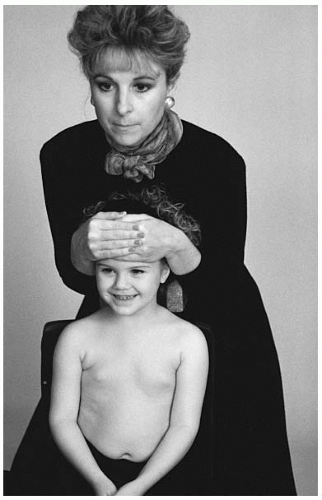 FIGURE 5-35 The head is rotated away from the contact hand for the ASLSLP listing. The doctor’s elbows are kept close to his or her sides. |
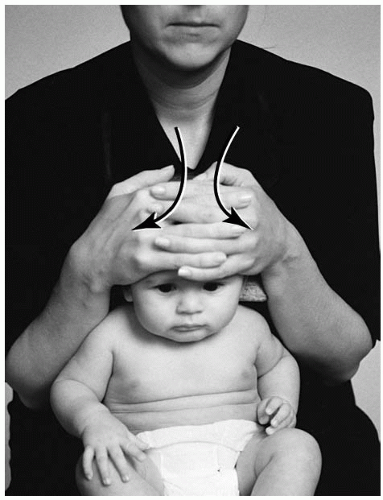 FIGURE 5-36 The infant is placed between the thighs of the doctor. The doctor places either thenar eminence on the contact site for the AS listing. The stabilization hand is placed on top. A second alternative is the doctor interlocking his or her fingers. The doctor’s elbows should stay close to the side of his or her body. |
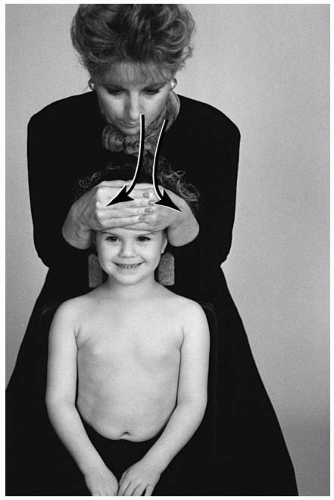 FIGURE 5-37 The smaller child may be raised in the chair by a pelvic pillow for the AS set-up. Either thenar eminence is placed on the contact site. The opposite (stabilization) hand is placed on top of the adjusting hand. A second option is for the doctor to interlock the fingers of both hands and placing them the contact site. The doctor’s elbows should stay close to the side of his or her body. |
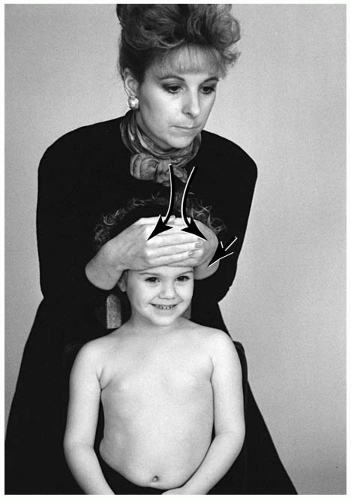 FIGURE 5-38 Seated ASLS condyle adjustment. The left thenar eminence is placed on the contact site. The stabilization hand is placed on top of the adjusting hand. The doctor’s elbows should stay close to the side of his or her body. |
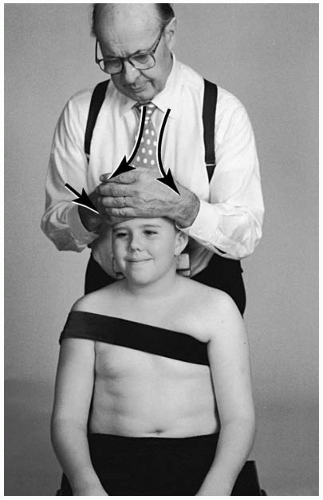 FIGURE 5-39 Seated ASRSRA condyle adjustment. The right thenar eminence is placed on the contact site. The stabilization hand is placed on top of the adjusting hand. The head is rotated slightly toward the doctor. The amount of rotation is in direct proportion to the amount of listing to be corrected. The doctor’s elbows should stay close to the side of his or her body. |
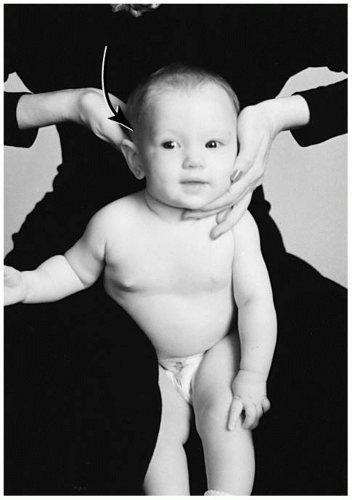 FIGURE 5-40 The infant can be placed between the thighs of the doctor. The doctor stabilizes with the chest or abdomen, combined with a slight medial thigh pressure. |
mastoid and the fingers will wrap around the C1-C2 articulation.
 FIGURE 5-41 The doctor’s thenar eminence will contact the supramastoid groove on the side of listing. |
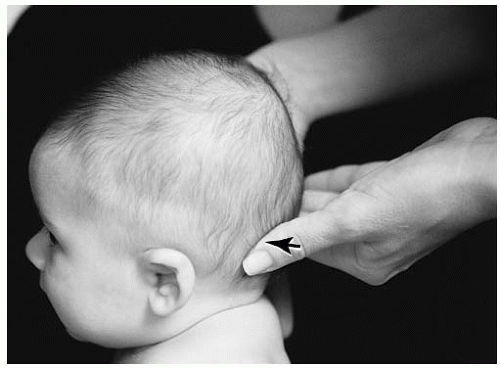 FIGURE 5-42 Set-up for a PSLS adjustment. |
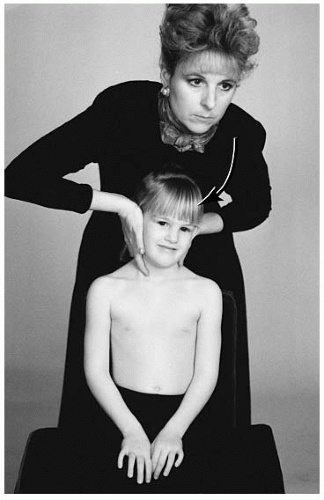 FIGURE 5-43 The head is rotated toward the doctor’s contact hand for the PSLSLA listing. |
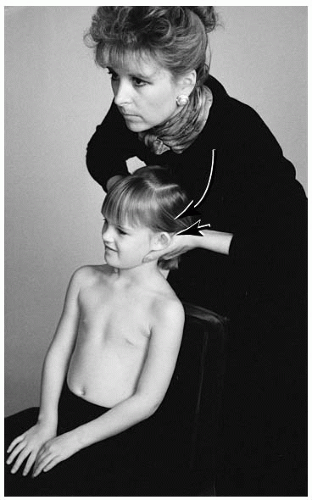 FIGURE 5-44 For the PSLSLP listing, the head is rotated away from the contact hand. The thrust is posterior to anterior, lateral to medial, with an inferiorward arcing movement. |
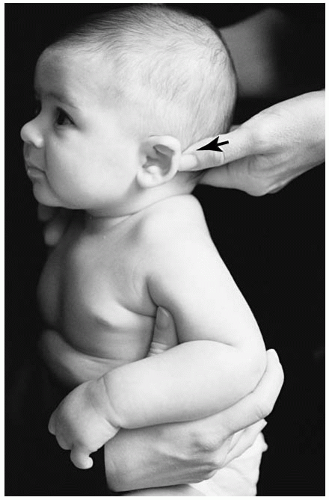 FIGURE 5-45 Seated PSLS set-up. The left distal end of the adjusting thumb or the thenar eminence is placed on the contact site. The stabilization hand supports the cervical musculature on the opposite side. |
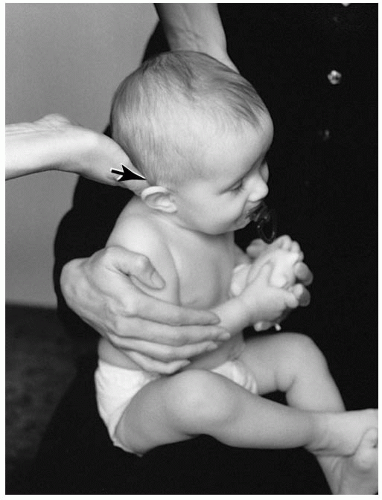 FIGURE 5-46 Seated PSRS listing. The right distal end of the adjusting thumb or the thenar eminence is placed on the contact site. The stabilization hand supports the cervical musculature on the opposite side. |
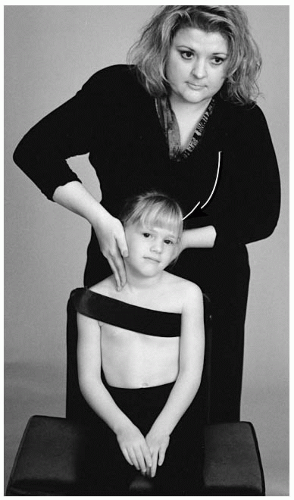 FIGURE 5-47 The PSLSLA condyle adjustment. The left thenar eminence is placed on the contact site. The stabilization hand is placed on the cervical musculature on the opposite side. The head is rotated toward the doctor. The amount of rotation is in direct proportion to the amount of listing to be corrected. |
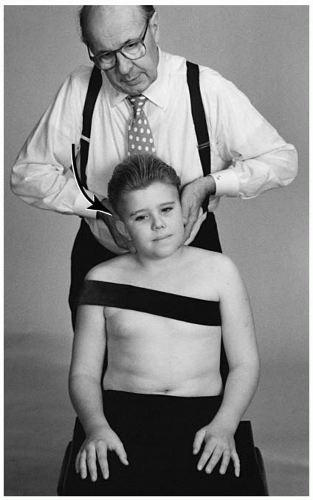 FIGURE 5-48 Seated PSRS condyle adjustment. The right thenar eminence is placed on the contact site. The stabilization hand is placed on the cervical musculature on the opposite side. |
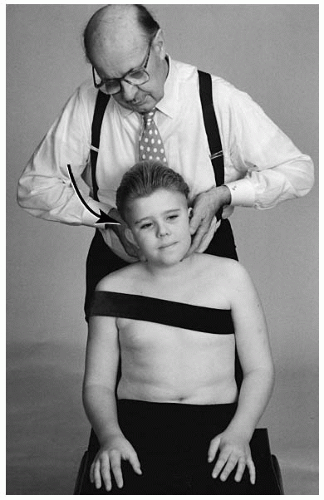 FIGURE 5-49 Seated PSRSRP condyle adjustment. The right thenar eminence is placed on the contact site. The stabilization hand is placed on the cervical musculature on the opposite side. The head is rotated away from the doctor. The amount of rotation is in direct proportion to the amount of listing to be corrected. |
must be determined. A posteriorly rotated atlas will be confirmed when the doctor can demonstrate restriction of that movement. A left posterior atlas (e.g., ASLP) will reveal restricted range of motion when the doctor rotates the patient’s head to the right. Likewise, a clockwise (+θ) restriction of the atlas reveals right posteriority (e.g., ASRP). The left anterior atlas (e.g., ASLA) is determined when the range of motion clockwise is restricted upon rotation. The ASRA listing is concluded when counterclockwise motion is diminished. The anterior “A” listing is often more difficult to determine.
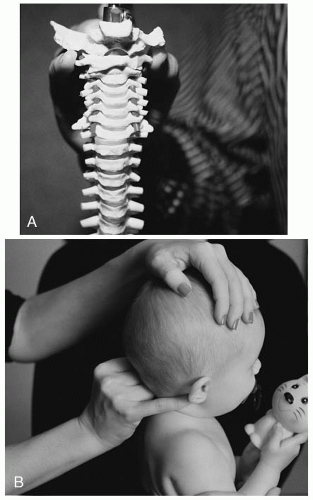 FIGURE 5-50 A,B: Depending on the size of the patient, the fifth or second digit will contact one side of the atlas transverse process. The thumb will contact the opposite transverse process. |
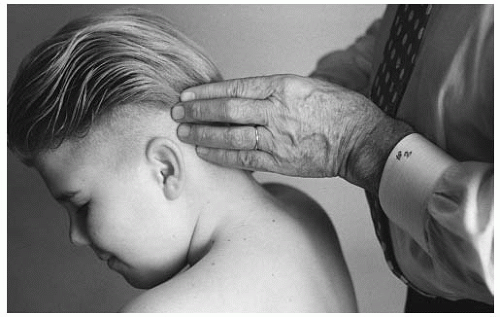 FIGURE 5-51 Dvorak’s maneuver may reveal rotational fixation in the upper cervical (C1-C2) region. |
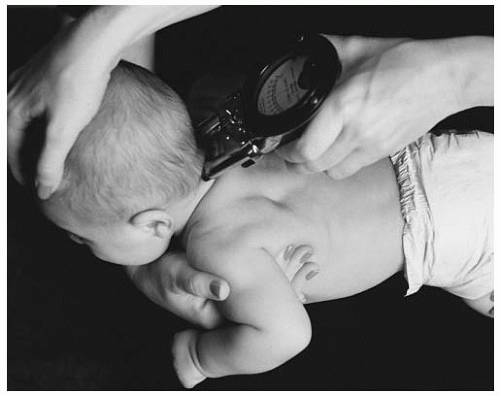 FIGURE 5-52 The infant’s baby fat may interfere with the gliding procedure. The parent or doctor may have to assist with a superiorward skin pull. |
The procedure for this examination is to glide the instrument from caudad to cephalad. Suboccipital hair is also another factor that may give a false positive finding. If a true positive finding does occur, the doctor must further determine through other examination methods if the reading reflects a C1 or C2 involvement due to the proximity of the articulations.
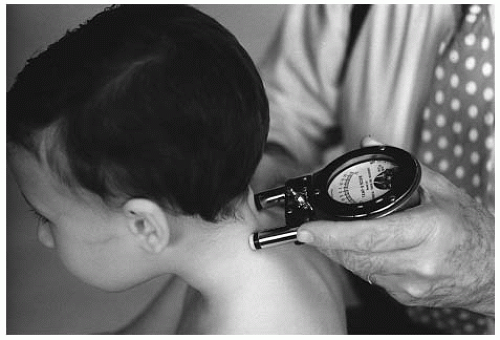 FIGURE 5-53 The doctor may stabilize the younger patient by bracing the shoulder or abdomen. |
TABLE 5.3 | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
the doctor’s stance should be slightly leaning forward toward the patient. For the anterior (“A”) listing, the doctor’s stance should be slightly leaning away from the patient. The parent may assist by stabilizing the infant’s head and body.
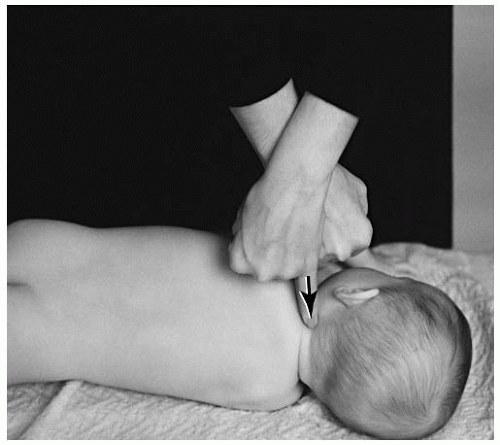 FIGURE 5-54 The atlas listing should be placed with the involved side up for a side posture set-up. |
 FIGURE 5-55 The infant may be placed on the lap of a parent for an atlas set-up. The parent will stabilize the infant. |
 FIGURE 5-56 A taller doctor may place the toddler between his or her legs for an atlas set-up. |
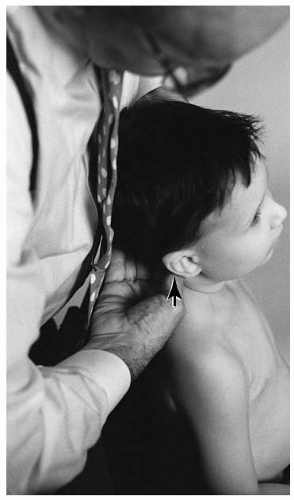 FIGURE 5-57 On the side of atlas laterality, the doctor will contact the antero-lateral aspect of the transverse process. |
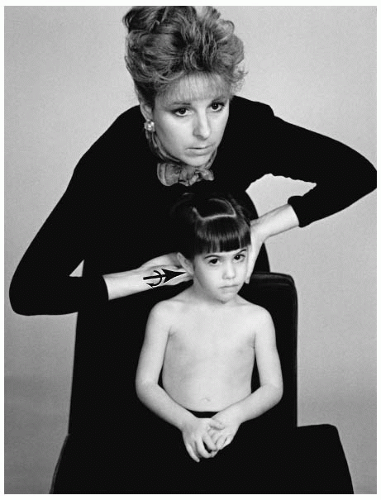 FIGURE 5-58 To eliminate the atlas posterior rotational listing, the head is rotated away from the contact site. |
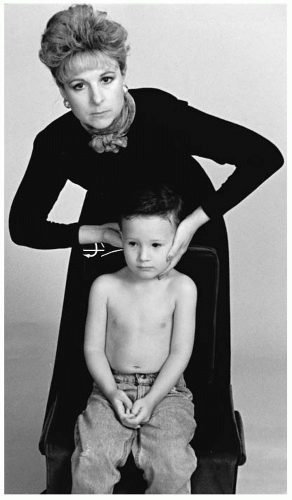 FIGURE 5-59 The head is rotated toward the side of the contact for the ASRA listing. |
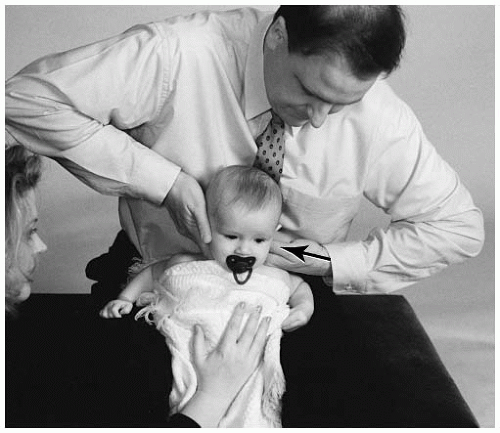 FIGURE 5-60 Seated ASL adjustment. The distal tip of the left thumb is on the contact site. The stabilization hand is placed cupping the opposite ear and stabilizing the C2-C3 articulation and the lateral musculature. |
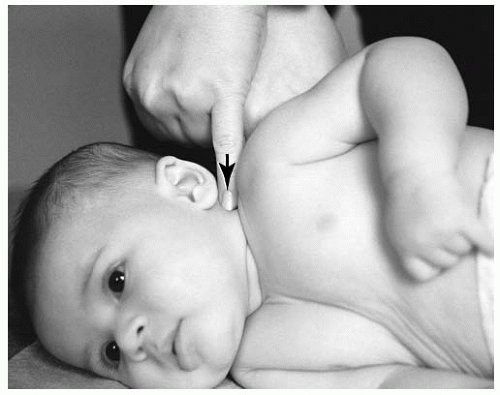 FIGURE 5-61 Set-up for a lateral ASLS listing. The distal tip of the fifth or second digit or thumb is on the contact site. The stabilization hand will support the contact hand by placing the fifth or second digit or thumb upon the nail bed of the contact hand. |
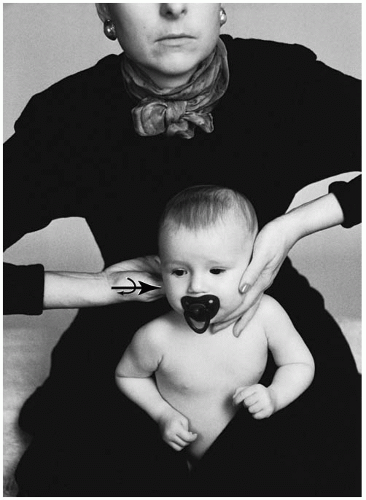 FIGURE 5-62 Seated ASRA adjustment. Distal tip of the right thumb is placed on the contact site. The stabilization hand is placed cupping the opposite ear and stabilizing the C2-C3 articulation and the lateral musculature. |
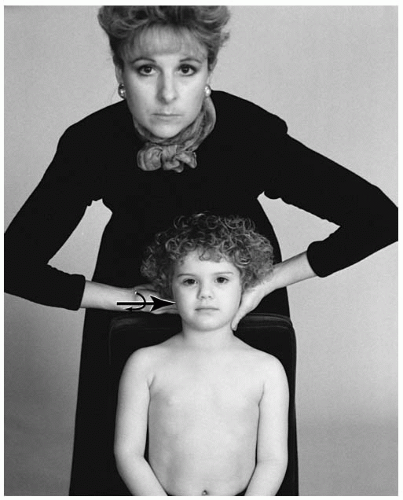 FIGURE 5-63 Seated ASR adjustment. The child may need to be raised on the chair by the pelvic pillow. The distal tip of the right thumb is on the contact site. The stabilization hand is placed cupping the opposite ear and stabilizing the C2-C3 articulation and the lateral musculature. |
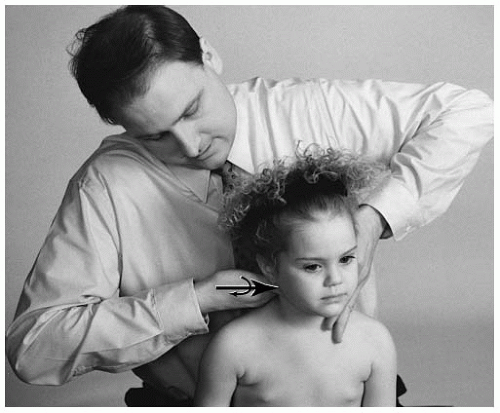 FIGURE 5-64 Seated ASRP adjustment. A taller doctor may place the patient between his or her thighs. The distal tip of the right thumb is on the contact site. To correct the rotational component (-θY), the head is slightly rotated away from the side of contact. The amount of rotation is in proportion to the rotational component. The stabilization hand is placed cupping the opposite ear and stabilizing the C2-C3 articulation and the lateral musculature. |
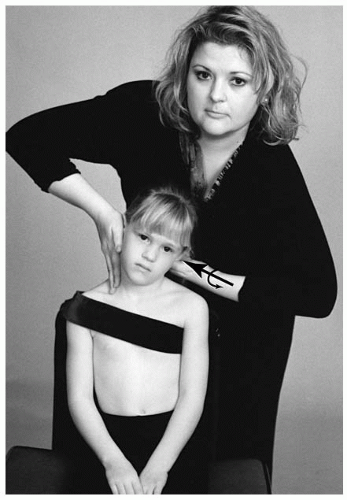 FIGURE 5-65 Seated ASL adjustment. The distal tip of the left thumb is on the contact site. The stabilization hand is placed cupping the opposite ear and stabilizing the C2-C3 articulation and the lateral musculature. Both arms should be opposed to each other when the set-up is completed. |
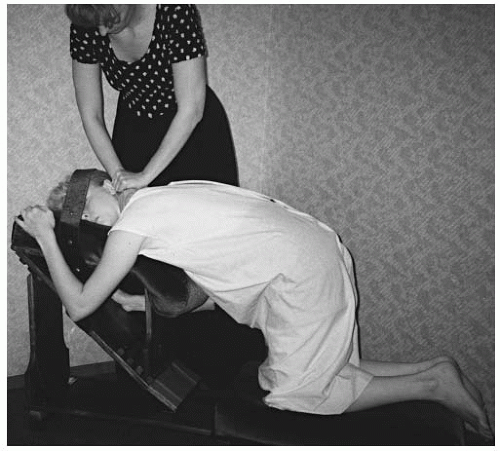 FIGURE 5-66 The modified toggle set-up is used for the AIL listing. The knee-chest table is suggested. The soft portion of the cephalad (right) hand is placed on the contact site. The caudad (left) hand will wrap around the adjusting hand. |
be noted that the capsular ligaments are less taut in the cervical spine. This allows for increased range of motion.
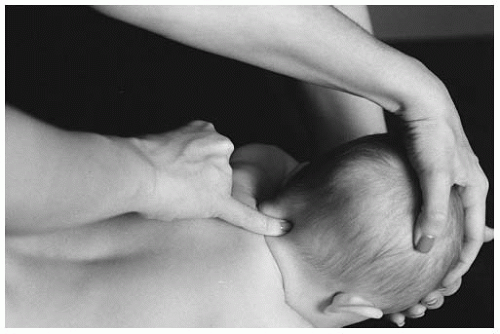 FIGURE 5-67 The distal end of the fifth digit contacts the spinous process of the cervical vertebra. The opposite hand supports the crown of the head. |
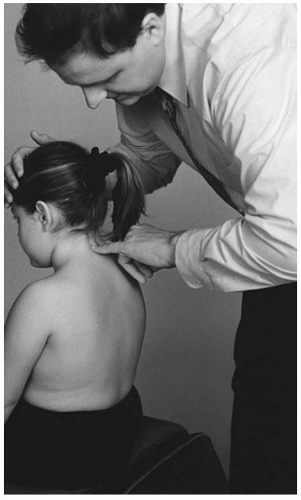 FIGURE 5-68 The doctor initiates the lateral bending of the cervical spine with the stabilization hand. The motion begins in the neutral position, and lateral bending is analyzed one side at a time. |
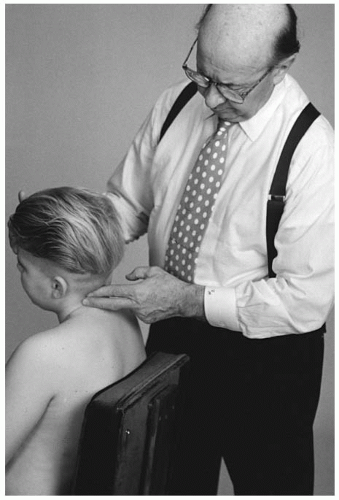 FIGURE 5-69 Global scanning of cervical segments is not recommended. |
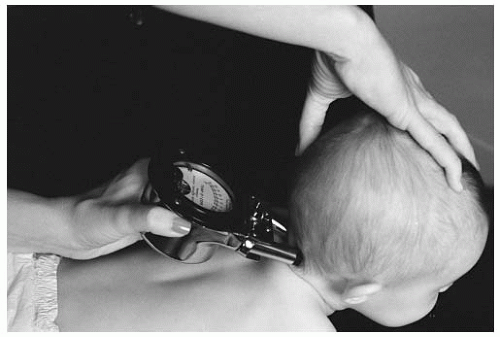 FIGURE 5-70 Stabilizing the cervical spine is necessary to prevent infant movement during instrumentation scanning. |
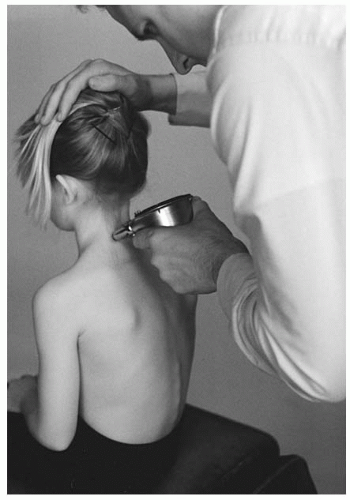 FIGURE 5-71 The instrument is glided inferior to superior on the cervical spine. |
coupling compensation and unnecessary spinous rotation. The set-up procedure for the chair adjustment is as follows:
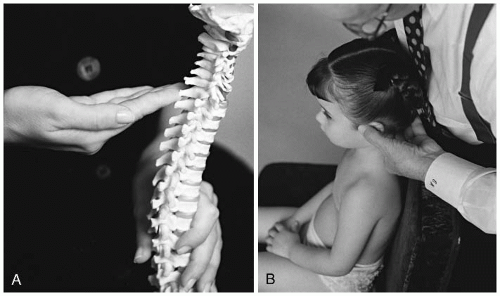 FIGURE 5-72 A,B: The first digit is supported by the second through the fourth digit as it contacts the spinous process or lamina listing. |
Lower the patient’s head into a flexed position. The doctor will create a tissue pull in the line of correction.
With the first digit (distal, lateral, and palmar aspects), contact the inferior and lateral border of the spinous process or the medial aspect of the lamina (for lamina contacts).
The stabilization hand will assist in bringing the head into a neutral position and slightly posterior.
Slightly laterally flex (10 to 15 degrees) the head to the side of contact.
On the opposite side, place the stabilization hand on the cervical segments.
Following the line of correction, the contact hand and forearm will perform the thrust. The thrust is a very quick movement. The stabilization hand will not produce any force during the thrust.
After the adjustment, the segment that has been contacted should be held for a moment. This will allow for the viscoelastic elements of the segment to respond.
To protect the vertebral arteries and the ligamentous elements of the joint, the doctor should avoid positioning in or thrusting on the cervical spine with rotation or rotation with extension.
cervical musculature (Fig. 5-74). The purpose of this contact is to stabilize the segments above and below the vertebra that will receive the thrust. The stabilization hand is not used to introduce any thrust or motion during the adjustment. To reinforce the vertebra that will be adjusted, the stabilization hand can distribute slight inferior pressure to the segment below. This will create a foundation to set the vertebra upon.
 FIGURE 5-73 The thumb of the thrust hand contacts the ramus of the mandible. The contact should maintain an arch before and after the thrust. |
any other listing (i.e., set-up and thrust for a PR is performed as a PLI-la);
normal FSU is present;
infection of the contact vertebra;
fracture or destruction of the neural arch or spinous process;
long lever set-ups;
the doctor is contacting broadly (overlapping segments) with the adjusting hand;
bringing the segment to pre-tension with traction, extension, flexion, lateral flexion of rotation; and
producing a thrust with unnecessary vectors as stated in item 1.
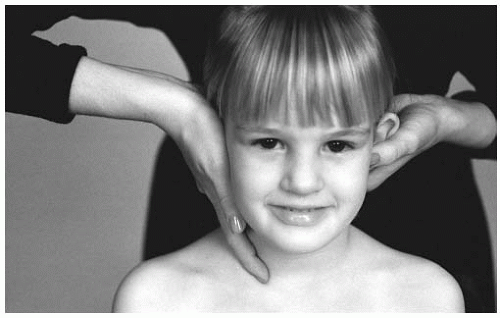 FIGURE 5-74 The palmar surface of the stabilization hand will contact the lateral cervical musculature. |
TABLE 5.4 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
the patient in an upright position can be accomplished with the assistance of the parent. The parent will seat the infant in an upright position on their lap and support the chest and back with both hands (Fig. 5-76). The doctor should carefully stabilize the opposite cervical musculature to prevent the introduction of unnecessary forces to other segments.
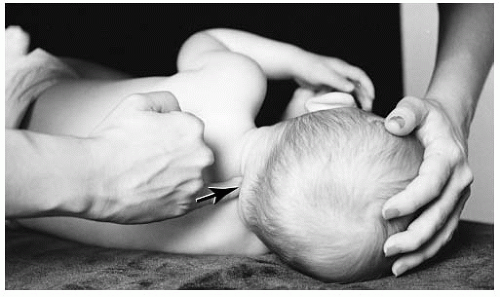 FIGURE 5-75 Placed in the side posture position, the spinous process is contacted by the distal end of the fifth digit. |
large male hand on the spinous process of a newborn) to specifically contact the segment, leading to overlap on additional segments.
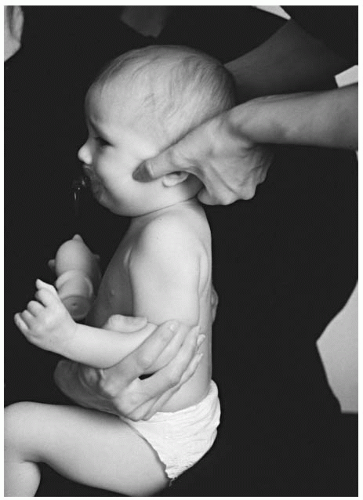 FIGURE 5-76 The older infant may be placed on the parent’s lap for a seated cervical set-up. |
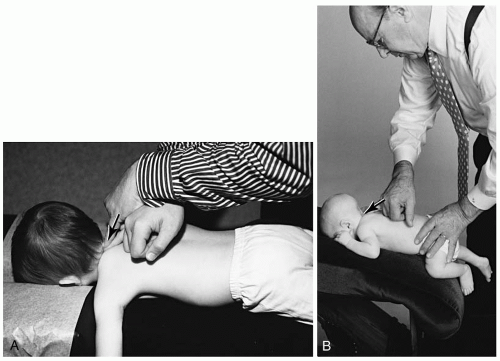 FIGURE 5-77 A: The hi-lo table may be used for cervical adjustments. B: The infant may be placed on the head piece of the knee chest table. The distal end of the fifth digit contacts the spinous process and the stabilization hand secures the infant’s position. |
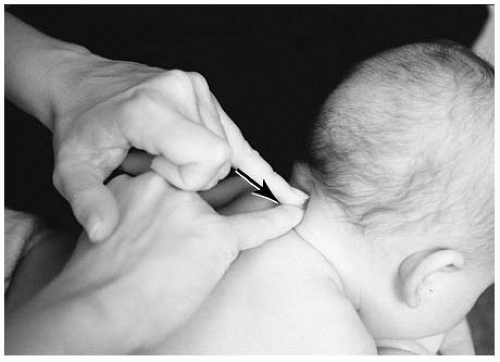 FIGURE 5-78 C2 posterior prone adjustment. The distal end of the fifth digit is placed on the contact site. To increase the depth of the thrust, the stabilization distal digit (e.g., fifth, second, thumb) will be placed on the adjusting nail bed. The doctor’s forearms should follow the plane line of the joint. |
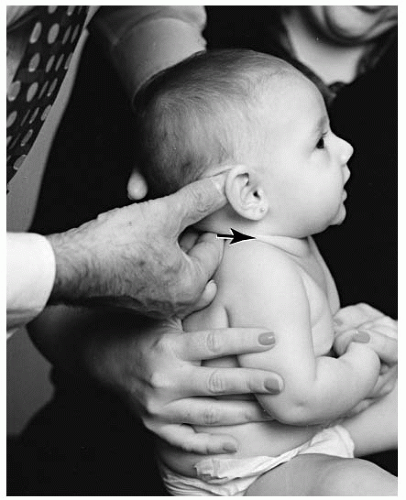 FIGURE 5-79 C3 posterior seated adjustment. The distal (and palmar) end of the right second digit is placed on the contact site. To increase adjusting hand stabilization, the third digit is placed next to the second digit. The palmar surface of the stabilization hand is placed on the opposite lateral musculature of the cervical spine. The thenar eminence of the stabilization hand is below the ear and thumb along the angle of the jaw. The doctor’s forearms should follow the plane line of the joint. |
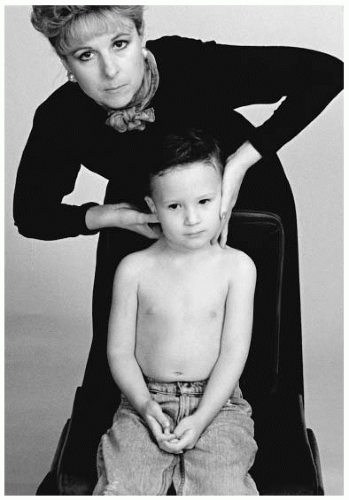 FIGURE 5-80 Seated C7 PR adjustment. The distal (and palmar) end of the right second digit is placed on the contact site. To increase stabilization of the adjusting hand, the third digit is placed next to the second digit. The contact hand thumb is placed on the ramus of the mandible. The contact thumb should not pull on the skin near the eye or be placed on the temporomandibular joint. The palmar surface of the stabilization hand is placed on the opposite lateral musculature of the cervical spine. The thenar eminence of the stabilization hand is below the ear and thumb along the angle of the jaw. The doctor’s forearms should follow the plane line of the joint. |
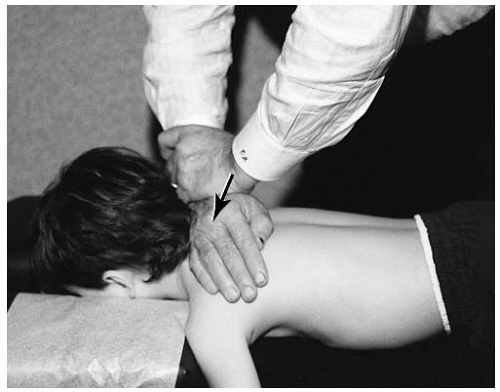 FIGURE 5-81 Prone C6 PR adjustment. The lateral border of the distal end of the right fifth metacarpal. To increase stabilization of the adjusting hand, the stabilization hand is placed on top of the adjusting hand with the fingers wrapped around the wrist. |
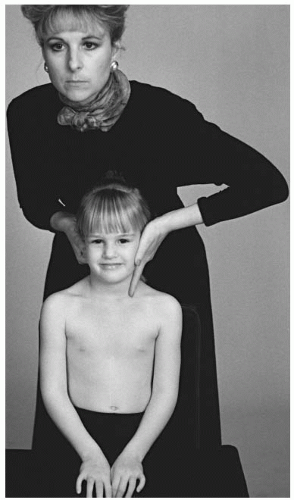 FIGURE 5-82 Seated C5 PRS adjustment. The distal (and palmar) end of the right second digit is placed on the contact site. To increase stabilization of the adjusting hand, the third digit is placed next to the second digit. The thumb of the contact hand is placed on the ramus of the mandible. The palmar surface of the stabilization hand is placed on the opposite lateral musculature of the cervical spine. The thenar eminence of the stabilization hand is below the ear and thumb along the angle of the jaw. The doctor’s forearms should follow the plane line of the joint. |
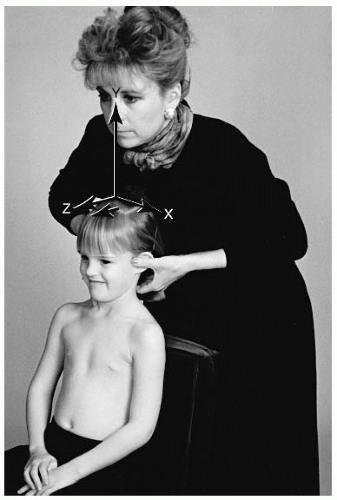 FIGURE 5-83 Seated C5 PRI-la adjustment. The distal (and palmar) end of the left second digit is placed on the contact site. To increase stabilization of the adjusting hand, the third digit is placed next to the second digit. The thumb of the contact hand is placed on the ramus of the mandible. The palmar surface of the stabilization hand is placed on the opposite lateral musculature of the cervical spine. The thenar eminence of the stabilization hand is below the ear and thumb along the angle of the jaw. |
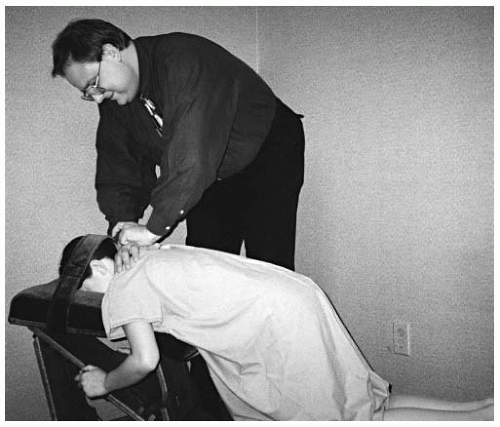 FIGURE 5-84 C2 PR knee chest adjustment. The lateral aspect of the right fifth metacarpal is placed on the contact site. The stabilization hand is rested on top of the adjustment hand. The doctor’s forearms should follow the plane line of the joint. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


