Risk Prevention, Risk Management, and Professional Liability
Risk Prevention, Risk Management, and Professional Liability
Gerald B. Hickson
Ilene N. Moore
DEFINITIONS
Adverse event (AE)—Undesired occurrence resulting from complication and/or error.
Adverse outcome (AO)—Undesired clinical outcome without implying cause. AOs may be due to: (a) the underlying pathologic disease process, (b) complication of treatment, (c) medical error, or (d) perception of a disappointing result.
Complication—A known risk of a specified procedure, operation, medication, therapy, or treatment plan.
Medical error—Failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.
Near miss—Event or deviation from best practice that did not cause harm but may signal risk for other patients.
This chapter addresses the myths and realities surrounding “risk management.” The goals of the chapter are for the gynecologic surgeon to better understand:
Health care’s increasing focus on safety (Introduction)
Incidence of AEs, which patients sue, why they sue, and whom they sue (Section I: The Genesis of Malpractice Claims)
Best practices for professional self- and group-regulation and learning from near-misses and AEs in order to promote patient safety and reduce claims risk (Section II: Professionalism and Risk Prevention)
Best practices for managing the aftermath of risk events (Section III: Managing Risk Events)
Medical malpractice law, discovery, trial, settlement, alternative dispute resolution (ADR), and tort reform (Section IV: Litigation)
We begin with a case:
Ms. AJ is a 46-year-old G3P3Ab0 female with a 5-year history of uterine fibroids. She notes increasing menorrhagia and pelvic pressure over the past 2 years with an increase in uterine size to 20 weeks. Dr. GYN has treated her conservatively but now recommends a hysterectomy. He engages Ms. AJ in an informed consent discussion, covering treatment options and their potential risks and benefits. Ms. AJ agrees to a total abdominal hysterectomy (TAH), and surgery is scheduled.
On the day of the procedure, her husband waits in the surgical waiting room for word that his wife is out of the operating room. He inquires several times at the reception desk, always told, “Someone will come out to talk with you.” No one does before his wife is transported to her inpatient room.
On arrival to his wife’s room, Mr. J meets the advanced practice nurse on Dr. GYN’s team, Ms. NP. In response to Mr. J’s questions, Ms. NP states, “You will have to ask Dr. GYN.”
Dr. GYN does not round on Ms. AJ until the following morning. Ms. AJ mentions that she expected to see him after surgery. Dr. GYN states, “I’m here now, so what do you want to know?” and proceeds to discuss in general terms that the surgery took a little longer than anticipated but overall the procedure went well. He checks her dressing, turns, and leaves the room.
On postoperative day (POD) 3, Ms. AJ tells Ms. NP that she is having low abdominal pain. Ms. NP states that pain is normal postoperatively, and she will prescribe some pills to take at home. She discharges Ms. AJ and instructs her to keep her post-op follow-up appointment with Dr. GYN, scheduled for 3 weeks hence.
INTRODUCTION
Health care delivery in the United States is evolving. Press coverage related to the Institute of Medicine (IOM)’s landmark studies, To Err Is Human and Crossing the Quality Chasm, accelerated public and industry recognition of patient harm caused by medical care. Most distressing was the IOM’s estimate that 98,000 people die annually in the United States as a result of medical error, with countless more injured. Unfortunately, progress aimed at making health care safer has been slow despite more than a decade of increased awareness and investment in research and safety initiatives. A study of 10 North Carolina hospitals by Landrigan et al. illustrates this point. The hospitals’ overall harm rate did not change between 2002 and 2007. Furthermore, two thirds of the harms were judged preventable. Despite the overall finding, a closer look at the data revealed a range of results among the study sites, suggesting that some appeared to have tackled risk issues more successfully than did others.
The fact is, safety and quality vary among, and even within, practices, hospitals, and health care systems. Some patients experience well-coordinated, timely, efficient, and effective service, while others receive fragmented, delayed, redundant, or inadequate care. As society becomes less tolerant of unsafe conditions and avoidable AEs, the focus on claims management must shift to an emphasis on risk prevention.
Utilizing evidence-based best practices, professionals must move patients out of harm’s way through risk surveillance, apply analytic methodologies to identify factors that contribute to AEs, fix defective systems, and hold professionals accountable. Furthermore, professionals must treat patients, their families, and each other with respect. Private and public payors are leveraging their market power to encourage practices that promote safety, improve outcomes, and manage costs. The Centers for Medicare and Medicaid Services (CMS), for example, uses a payment withholding and reward system to incentivize professionals and hospitals to achieve lower hospital-acquired infections rates, reduced need for hospital readmissions, and integration of patient perceptions of care into quality standards. Payors also deny reimbursement for the extra care needed to treat outcomes they deem avoidable or place liens for reimbursement against patientclaimants’ jury awards and settlements.
SECTION I: THE GENESIS OF MALPRACTICE CLAIMS
KEY POINTS: GENESIS OF CLAIMS
•
Many patients with valid potential claims do not sue.
•
Noneconomic factors play a significant role in patients’ and families’ decisions to sue.
•
Claims are nonrandomly distributed.
•
3% to 8% of physicians by specialty account for over half of all risk management expenses.
•
Risk status appears constant over time.
•
Unsolicited patient complaints are related to malpractice claims risk.
•
Intervention with high-complaint physicians can lower claims risk.
Incidence of AEs
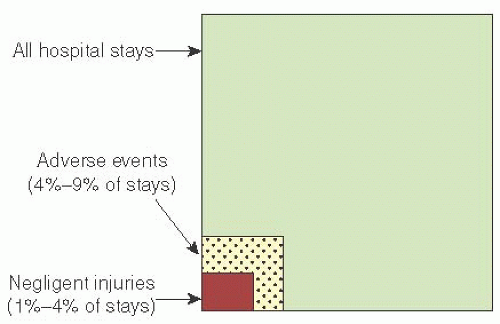
Responding to the malpractice insurance crisis of the 1970s, the California Hospital Association organized a study in which 21,000 medical charts from all 1974 hospitalizations at 23 California hospitals were reviewed. Mills reported that the study found almost 5% of inpatients (7% if over 65) experienced AEs. Nearly one fifth of the AEs were further classified as injuries for which the professional staff and/or hospital would likely be liable, that is, due in whole or in part to medical negligence.
The Harvard Medical Practice Study I (HMPS I) reported similar findings from a review of 30,000 New York State hospital records from the year 1984. The overall AE rate was 3.7%; for those over 65, the AE rate was 5%. Twenty-eight percent of the AEs involved negligence (Fig. 4.1). Replicating the study in Colorado and Utah, the researchers found essentially the same results.
Other studies, including some from the international community, also confirm that the majority of AEs do not involve negligence.
Who Sues?
Or, to rephrase, who are the claimants in medical malpractice cases?
Danzon reported that in the 1970s no more than one out of 10 patients injured by care filed suit. In the HMPS III, Localio and colleagues found an even lower claims rate among injured patients. HMPS III matched 47 malpractice cases to the 30,000 1984 HMPS I hospitalizations. In only eight of the 47 cases did medical record review demonstrate evidence of negligence. However, these eight cases represented only two percent of the patients with AEs attributable to medical negligence. The majority of claims were instead filed by patients whose AE did not result from negligence; for every suit with an AE attributed to negligence, five to six suits lacked such evidence. The results were consistent with Mills’ earlier observation that “most patients who file lawsuits for medically caused disabilities do so without real knowledge about presence or absence of legal fault as the cause of their disability”. HPMS III remains an important study for its insight into the fact that much of the legal activity involving allegations of medical malpractice represents circumstances where care was appropriate, but the patient or family do not appear to understand or accept.
A later study of 1,452 medical malpractice cases conducted by Studdert et al. found that, in comparison to HMPS III, three out of five claims are legally justifiable. What might account for the higher proportion of cases deemed valid? We suggest four potential factors: (a) study methodology, (b) threshold for finding preventable harm, (c) evolving error disclosure practices, and (d) case selection.
FIGURE 4.1 Adverse events versus negligent injuries. Adapted from Bovbjerg RR. Medical malpractice: problems & reforms— a policy-maker’s guide to issues and information. Washington, DC: The Intergovernmental Health Policy Project, George Washington University, 1995; Mills DH. Whither malpractice regulation? West J Med 1988;149:611; deVries EN, Ramrattan MA, Smorenburg SM, et al. The incidence and nature of in-hospital adverse events: a systematic review. Qual Saf Health Care 2008;17:216; Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard Medical Practice Study I. N Engl J Med 1991;324:371.
The study methodologies differed in that HMPS III reviewed patients’ medical records for evidence of AEs and negligence, while Studdert reviewed insurers’ closed claims. Documentation in medical records can be incomplete or absent. In contrast, insurers’ files contain deposition transcripts and/or witness interviews that may reveal evidence of negligent events not found in medical records.
Second, because of our evolving understanding of how faulty systems and human factors intersect to cause error, some of the “no negligence” AEs in HMPS III might be characterized today as avoidable error-based AEs. The IOM definition of error (“the failure of a planned action to be completed as intended or the use of wrong plan to achieve an aim”) captures the notion that occurrence of an unintended outcome itself signals likelihood that faulty systems and/or human decisionmaking contributed. Reassignment of some of the 47 HMPS III cases would likely have brought HMPS III’s valid:invalid ratio closer to Studdert’s.
The third potential reason for Studdert finding a higher percentage of justifiable claims may relate to increasing error disclosure. Some patients who might otherwise never realize medical error caused them harm may sue once this information is disclosed. However, the data so far suggest that disclosure does not lead to more suits nor an increase in overall liability costs; rather, disclosure may reduce suit and claims rates, time to resolution, average payouts, and legal costs.
A fourth factor is that plaintiff’s attorneys today are likely more selective about which cases they accept. Attorneys take malpractice cases on a contingency (rather than hourly pay) basis and are not paid if they lose. Thus, accepted cases must potentially yield a recovery large enough to cover attorney fees and upfront costs, including experts’ travel expenses and billings for time spent reviewing cases, executing certificates of merit (in states where required), and testifying.
Rice reports: “Experienced malpractice attorneys say they tend to be very judicious about what they pursue.”
Shepherd reports that “Over 75 percent of the attorneys… survey[ed] indicate[d] that they reject more than 90 percent of the cases that they screen…over half…responded that, even for a case they are almost certain to win on the merits, they will not accept the case unless expected damages are at least $250,000.”
In sum, it is important to recognize that there are patients who are injured by medical care, and a significant proportion of injury is due to avoidable error. However, most patients with valid claims do not pursue litigation. Although many claims are valid, there still remain patients who file claims despite little or no evidence of bad care. We now examine what motivates patients and families to contact an attorney.
Why Do Patients Sue?
Some professionals assert it is all about “ambulance-chasing lawyers” and plaintiffs’ desire for money; however, the evidence suggests that decisions to sue are more complex. In one study where families were asked why they had sued their obstetrician, many offered more than one reason. Money was mentioned as a reason for contacting an attorney by a quarter of the families, but most identified a host of noneconomic reasons: wanting to “make sure this doesn’t happen to anyone else” (19%), needing information (20%), feeling their loved one would have no future (20%), believing there was a cover-up (24%), and advice from an “influential other” (33%). Only one respondent indicated that she had been solicited by an attorney. In the United Kingdom, Vincent et al. also found noneconomic factors more prominent in patients’ decisions to sue than the need for financial compensation.
While some factors are outside a professional’s control, how and what information a professional provides to the patient is not. As gynecologic surgeons reflect about their personal risk prevention strategies, it is beneficial to examine the types of informational issues families cited as reasons for filing: no one would tell them what was wrong, their physician would not answer questions, and no one warned them that the problems might be permanent. The need to understand is normal. Patients want answers if only to help dispel fears that somehow something they did contributed to the AO.
If patients do not raise questions, do not assume they have none. Make clear through your verbal and nonverbal communications that you want to address their questions. If you are asked questions, say what you know but be careful about speculation. If you do not know the answer, say so. Specify when you expect to be able to follow up with more answers, and make certain that you do follow up.
Patients and families may claim they did not receive clear explanations of what happened even when the professional tried. When you provide answers, seek to confirm that they understood utilizing “teach-back” methods; do not equate a head nod with comprehension.
Ineffective communication may also lead to allegations of cover-up or incompetence, especially if other professionals provide conflicting information or “joust” (criticize the treating professional, practice, or health care institution). For the one third of families in the study who decided to file suit based on the “advice” of an “influential other,” most often it was a health care professional who told them the bad outcome was a result of poor care and/or that they should sue. The following represent examples of reported communications:
“The nurse practitioner told me, “They gave you the wrong medication when they discharged you. That’s why you’re having this problem.”
“After talking to the anesthesiologist, I realized it clearly was the surgeon’s fault. I had no idea that the bad outcome was related to Dr. XX’s care until he suggested….”
“Influential others” fill gaps when patients have unanswered questions, residual concerns, lack of trust in the professional, or worries about the future. Healthcare professionals should remain alert to the possibility of error by others. However, by jousting and offering gratuitous negative comments, they bear some responsibility for inflaming and undermining colleagues’ relationships with their patients, which can contribute to unnecessary litigation. Thus, professionals should ask themselves a set of questions before commenting about care delivered by others:
Do I have all the data?
Am I certain the history provided by the patient is accurate?
Do I have the expertise, or am I making a judgment about someone who practices in another field?
Whenever possible, professionals should seek direct clarification of the facts of the case from colleagues who provided care to the patient. If direct contact is not possible, reviewing the medical records may shed light.
If needed information is not available or what is learned does not reassure, then reporting through appropriate channels is professional. In the group setting, the reporter can make practice leaders aware. In the hospital setting, one should utilize an online reporting system (if available) and/or directly contact designated personnel such as risk managers and/or safety and quality officers. In other words, commitment to safety means that colleagues and team members raise questions with the involved parties, route concerns for objective review, and if information emerges that impacts the patient, share it with him/her in a professional manner. Arguing at the patient’s bedside or rushing to tell a patient or to comment in the medical record that a previously treating professional “messed up” is not consistent with principles of professional disclosure.
Inflammation and communication failures can trigger unnecessary claims. Examples of such circumstances include the following: (a) The AO is not due to medical mishap, but the patient believes it is; (b) a medical error did not result in harm, but the patient believes it to be the cause of his/her outcome; and (c) medical error caused harm, but failed opportunities to address the patient’s and family’s needs spurred their decision to pursue legal action and/or to make unreasonable demands. Understanding the reasons families sue can help professionals reflect and act in ways to prevent claims that might be avoided.
Who Gets Sued?
Many physicians assert there is little they can do to prevent malpractice claims, citing as “fact” that “everyone in my specialty gets sued.” It is true that overall claims rates vary by specialty. Jena et al. and Kane found neurosurgeons and cardiothoracic surgeons to share claims rates of 19% per annum; general surgeons, 15%; and obstetrician-gynecologists, 12%. (Obstetrician-gynecologists also account for the highest number of indemnity payments of over one million dollars.) In comparison, psychiatrists, family physicians, and pediatricians experience overall rates of 3% to 5%.
Such aggregate statistics suggest that claims are common and likely inevitable over the course of a career. They do not tell the whole story, however, for claims rates do not address the distribution of claims among physicians. In fact, claims are nonrandomly distributed, and a small subset of physicians within any specialty accounts for a disproportionate share of claims and payouts. Studying physicians in Florida, Sloan and colleagues reported that, depending on the specialty, 3% to 8% of physicians account for 75% to 85% of all indemnity payouts within their specialty: 8% of surgical subspecialists, 6% of obstetrician-gynecologists, and 3% of medical specialists.
Other studies have confirmed nonrandom distribution of claims and payouts within multi-specialty groups. Furthermore, the propensity to attract claims persists over time; physicians with high numbers of past claims appear to continue this pattern into the future.
Is there something different about physicians who experience multiple claims compared with peers who are seldom or never sued, or are they just unlucky? Four likely hypotheses are that high suit physicians: (a) care for a more litigious population, (b) care for the sickest patients, (c) are less technically or clinically competent than low-suit colleagues, and/or (d) do not “connect” as well with patients.
Well-educated, higher income patients are more likely to sue than are those who are elderly, poor, or uninsured. However, Entman and colleagues found no difference in practice demographics for obstetrician-gynecologists with a history of multiple claims when compared with peers in their community with few or no claims.
Review of patient medical charts from the practices of high versus low claims obstetrician-gynecologists also revealed no significant differences in patient mix, acuity, documentation practices, or evidence of marginal care. The area in which high claims physicians did differ, however, was in how they were perceived by patients. The researchers asked open-ended questions of the patients (none of whom had filed suit against their physician) whether any aspects of care failed to meet or exceed their expectations. Their responses could be sorted into concerns about their physician’s communication skills, care and treatment, access and availability, and “humaneness” during labor and delivery. The following are sample patient comments from the interviews:
“He did a very poor job of communicating… discounted everything that we said.”
“Dr. X offered no information. I felt he was hiding information.”
“…never gives me more than 5 minutes.”
“He was terrible with this pregnancy and was even worse with the next one, but the HMO said I had to stay with him. I kept hoping to get his partner, but never lucked out. I’m not getting pregnant anymore because of him.”
Patients whose obstetricians had a history of multiple lawsuits voiced three times more complaints about their care than did patients of low-suit physicians. In other words, the same small group of physicians responsible for high numbers of malpractice cases was also associated with higher numbers of patient complaints and dissatisfaction.
Identifying Professionals at High Risk of Claims
If physicians with high numbers of malpractice cases have significantly higher complaint rates than do their peers with few or no claims, is the converse also true? Do patient complaints identify physicians at high risk for claims? If they do, perhaps it is possible to identify high-risk physicians by a method other than waiting for lawsuits.
Unsolicited “patient complaints” are the stories patients and families share with practice and hospital representatives about their care experiences:
“The GYN… didn’t listen… just cut me off… made me worry about the treatment plan.”
“[Patient] described the exam as torture… Dr. XX was yanking and shoving the speculum… it hurt worse than her surgery.”
“They left me sitting in the stirrups… then Dr. XX made a very inappropriate remark and left the room… I felt humiliated.”
Capturing patient complaints allows opportunities for “service recovery,” that is to say, helping to “make right” what patients and families perceive as wrong. Hickson and colleagues hypothesized that coding and aggregating unsolicited patient complaints over time would reveal risk patterns. Studying unsolicited patient complaints at an academic medical center Hickson et al. and Moore et al. found:
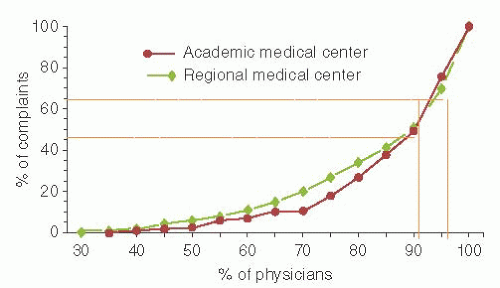
Most physicians were associated with few or no unsolicited patient complaints over a 6-year audit period. Five percent of physicians were associated with nearly one third of all patient complaints (Fig. 4.2).
Risk management activity was associated with three characteristics of physician practice: unsolicited complaint numbers, specialty, and productivity as measured by relative value units (RVUs) by discipline. Logistic regression analysis revealed, however, that of the three predictors of risk, unsolicited complaints and risk management activity were most closely linked.
Association of physician productivity with lawsuit risk was minor when compared with patient complaints and disappeared for physicians with multiple lawsuits. In other words, the unique ability of a physician and his/her practice to create dissatisfaction among patients overwhelmed productivity as a predictor of high claims experience.
Nine percent of physicians, as a group, were associated with the highest numbers of unsolicited complaints and 50% of all risk management expenditures and payouts.
A follow-up study at a regional medical center affirmed the results (Fig. 4.2).
Stelfox et al., Fullam et al., Cydulka et al., and Levtzion-Korach et al. have confirmed the relationship between patient complaints and claims experience. Furthermore, any relationship between patient satisfaction survey data and risk management activity disappears once patient complaints are entered into the model. Complaint distribution patterns similar to those from the multispecialty group studies are also seen for single physician specialty groups including trauma, urology, and cardiothoracic surgeons and can support targeted interventions to help reduce unnecessary risk.
In sum, the empirical data demonstrate that professionals’ own behaviors and practices are primarily responsible for inspiring claims rather than external factors. Malpractice claims should not be viewed as just an expected “cost of doing business.” Rather, AOs are more likely to lead to claims when patients are dissatisfied with their physician’s practice and/or interpersonal behaviors. Unless high-risk professionals are willing and able to address sources of patient dissatisfaction, their malpractice costs will continue to exceed those of their low-risk colleagues.
SECTION II: PROFESSIONALISM AND RISK PREVENTION
Traditional risk management programs focus primarily on managing claims. Skillful management of potential claims is, of course, important to gynecologic surgeons when their patients are unhappy about outcomes of care. Modern risk prevention programs, however, also proactively identify sources of risk through surveillance and monitoring, utilize methodologies that elucidate “sharp end” (obvious) and “blunt end” (less obvious) contributors to AEs, and take corrective action to fix defective systems and remedy deficient human performance and behavior. Both risk mitigation and proactive management of potential claims (Section III) reduce medicolegal costs.
Organizations with a knowledgeable risk prevention/management department and stakeholders with aligned interests can help reduce risk of patient harm and individual professionals’ risk for claims. One way to lessen your own risk is to practice in a setting with a good, integrated, aligned risk prevention program.
KEY POINTS: BEST PRACTICES FOR RISK PREVENTION
•
Promoting professional behaviors to support teamwork
•
Early reporting and timely review of unexpected AOs, suspected errors, and near misses
•
Event analysis methodologies to understand “how and why” the risk event occurred and a process for fixing system defects
•
Remediation of human performance and behaviors that threaten patient safety and increase risk of medical malpractice claims
Professionalism
Professionalism is the fundamental human force behind the goal of making medicine safer and kinder. Professionalism requires more than clinical knowledge. Beyond the need for cognitive and technical competence are the essential behavioral dimensions: modeling respect, communicating effectively, being available, and demonstrating willingness to give and receive feedback. The Joint Commission’s requirement for Ongoing Professional Practice Evaluations reflects growing recognition that the ability to deliver safe, high-quality patient care requires competency in this complex skill set.
Professionalism promotes teamwork; unprofessional behavior creates team dysfunction. Rosenstein and O’Daniel’s survey of perioperative personnel found disruptive behaviors to be common. Study participants linked unprofessional behaviors with communication failures as well as distractions leading to momentary lapse of attention, well documented by others as contributors to errors and AEs. Sample comments from study participants included:
“Some surgeons seem to believe that they have the right to be rude…and disrespectful to non-physicians. It makes it very difficult to perform at a high level when one is constantly in fear of being screamed at.”
“We have some… team-oriented surgeons… but the ones who are disruptive make it so intensely difficult that it is overwhelming. Unfortunately, as good as the good ones are, they can’t outweigh how bad the bad ones are.”
Professionals are committed to self-assessment of their performance and continually seek ways to improve. Professionals are also committed to group regulation. Risk prevention, therefore, includes methodologies to identify and address unprofessional interpersonal and practice behaviors that threaten safety. Professionals’ commitment to group regulation is evidenced by their participation in related activities, including peer review. Professionals further assume personal responsibility for identifying faulty systems within the environment, work to “fix” systems thus identified, and disseminate information about best practices.
Reporting and Timely Review
How do professionals learn about threats to safety within their practice, group, or health care institution? Active reporting is a critical component of a risk prevention program. Professionals, support staff, patients, and families are all observers, and by lowering barriers to reporting, they help identify threats to safety and quality. Information on how to report should be disseminated so that all potential reporters, including patients, know how to report within the practice or health system (e.g., by phone, written contact, face-to-face, and/or electronic reporting) and to whom they should report (e.g., patient relations personnel, practice leaders, or a risk manager).
Practices, health care organizations, and malpractice insurance carriers should make clear in their policies what types of events health care professionals and personnel are to report. These should include sentinel events, errors or suspected errors with consequences (e.g., lengthened hospital stay, temporary or permanent disability, death), near misses, coworker concerns about performance or conduct, information about unsafe conditions or faulty equipment, and patient/family complaints of which they are aware.
Early reporting of suspected risk events, near misses, or patient injury to the professional’s risk manager or malpractice carrier is always good. Reporting permits timely review and optimal management of a potential claim. Designated personnel must promptly address each report, review the asserted issues, and assemble a response and action plan. Reports should also be entered into a database for tracking, trending, and identifying patterns.
Early reporting also allows an opportunity to quickly address patient and family concerns and rebuild trust. In particular, when avoidable error with harm is identified, disclosure with apology may reduce inflammation and therefore risk of a lawsuit. Emerging evidence suggests that honesty and proactive risk prevention strategies help avert litigation and reduce claims costs.
Despite its critical importance, professionals sometimes hesitate to report. Possible reasons include lack of clarity about the mechanism for reporting and loyalty to the professionals involved in the incident. Because of concerns that even anonymous reporting will invite retribution from those who are the subject of the report, explicit nonretaliation language should be a part of the reporting policy to protect reporters and must be enforced.
Ultimately, failure to report is not consistent with being a professional. Reporting is part of one’s commitment to selfand group-regulation. Success of surveillance relies on team members recognizing the value of reporting safety risks, understanding it is an expectation and part of their professionalism, and making it psychologically safe for all to speak up when they observe practices that appear unsafe.
Event Analysis Methodologies
If harm or the potential for harm is suggested by a report, professionals try to understand what happened and why. Event analysis methodologies represent best practices in seeking to understand how errors occur and how to prevent them. Practices, health care organizations, and medical malpractice insurance carriers should endorse utilization of event analysis in order to identify and address faulty systems and individuals.
Common event analysis techniques include: (a) risk management file review (b) root cause analysis (RCA), also termed event analysis, or multicausal analysis and (c) multidisciplinary morbidity, mortality, and improvement (MMM&I) conference. The tools support a balanced focus on systems and individual accountability, and the information uncovered by the analyses is what drives risk prevention efforts.
Protecting event analysis activities from discovery may vary by state, and you will want to seek legal advice to set up these processes. Even in states where legal protection of such activities is untested, professionals’ commitment to continual learning and improvement can help them work through how best to achieve what is right for patients and their care.
Risk Management File Review
Risk management file review is the foundation for evaluating all claims and potential claims, whether the insurer is a carrier or a self-insured entity. The case is assessed for potential liability by reviewing, for example, medical records, witness interviews, and consultant/expert reports. Reviewers seek to identify strengths and weaknesses in individual cases, including medical conditions likely to have led to the same outcome in the absence of medical or nursing error, and patient actions that may have contributed.
The risk prevention lens, in contrast, views cases as opportunities to learn about modifiable contributory factors that can prevent future occurrences. For example, a traditional risk manager may focus on poor documentation that represents a weakness in a case and suggest better documentation in the future to make cases more defensible. A risk prevention lens would disseminate the notion that poor documentation impairs team communication and therefore the ability of the team to achieve intended outcomes. Exhorting improved documentation practices through the latter lens serves to increase patient safety in a broader sense.
Although the traditional risk management model cautions against sharing results of a review for fear the opposing litigant could gain access to that information during discovery, modern risk prevention recognizes that waiting years for a case to close before disseminating lessons learned inhibits professionals’ ability to improve care. Coded and aggregated medicolegal data can be used to identify recurring safety themes and individual and group patterns, and when consolidated with claims files data within larger consortia (e.g., the Harvard-based CRICO/RMF), allow identification of common areas of risk. Larger databases can help prioritize areas in which best practice standards should be developed, disseminated and implemented. For example, the American Society of Anesthesiologists (ASA)’s review of over 5,000 closed claims dating from the 1970s through 1994 transformed a medical discipline’s safety record. Practice changes such as use of end-tidal CO2 monitoring and intraoperative pulse oximetry, virtually eliminated claims for undetected esophageal intubation and inadequate ventilation.
Root Cause Analysis
RCA is a tool for drilling down and understanding what caused an AE. RCAs are designed to explore AEs for factors that represent variation in performance by systematically teasing out both sharp and blunt end contributors to AEs. RCAs attempt to answer three questions: What happened? Why did it occur? (“Ask five times.”) What can be done to prevent recurrence? Follow-up should occur and the action plan assessed for effectiveness.
In smaller practices, a designated group can develop expertise in RCAs. In larger settings, participants in RCAs generally include a trained facilitator, team members, managers of involved service areas, risk managers, and quality and safety officers. Causative factors are coded, action plans developed, and professionals and staff educated. Percarpio and Watt’s recent study of Veterans Affairs medical centers suggests that committing resources to RCAs results in safety improvements such as lower postoperative complication rates.
Multidisciplinary Morbidity, Mortality, and Improvement Conference
The MMM&I conference is an educational forum, open to a broader range of individuals than attend an RCA. MMM&I attendees include professional, clinical, administrative, and clerical staff. In the hospital setting, attendees likely also include pharmacists and learners. The conference is designed to help attendees feel comfortable speaking up about circumstances and behaviors that contributed to an AE (psychological safety) and to lessen the inhibitory effect of the hierarchy. In addition, by reminding everyone that errors occur, the MMM&I can help start the healing process for professionals involved in the case.
In contrast to traditional M&M (morbidity and mortality) conferences, which tend to focus on individual performance (sometimes perceived as “shame and blame”), MMM&I conferences review a case within a framework of factors known as common contributors to failures or errors resulting in AEs. In one model, six domains (policies, environment, equipment, communication, procedures, and people) are set up as a “fishbone” or cause-and-effect Ishikawa diagram to identify all factors that contributed to failures. The “I” (Improvement) of the MMM&I results when a work group prioritizes identified issues and develops a follow-up action plan and assigned team members complete tasks and provide feedback.
Aggregating analyses from MMM&I conferences can identify recurring factors that underlie failures and help focus efforts on highest-yield projects. For example, one department of obstetrics-gynecology aggregated analyses of inpatient women’s health cases and identified contributory factors such as jousting, ineffective communications, lost and overlooked documents, inadequate supervision, failure to follow policies, and equipment issues. Patterns suggested that improved systems for alerting key professionals for emergencies and facilitating intercaregiver communication would help remedy these issues. As a result, the department established a team to identify best practices and trained all clinical personnel.
Remediating Human Performance and Behavior
Unsolicited patient complaints support risk prevention efforts. Complaints help identify opportunities for service recovery, learning about threats to safety, and supporting interventions for professionals at high risk for claims.
Only a fraction of the patients who are unhappy with their care complain. For each patient who voices a complaint, many dissatisfied patients do not (estimated ratios range from one out of three to fewer than one in fifty). Patients who do not share their concerns with you or your group may instead tell family, friends, neighbors, and, increasingly, the general public via social media. Professionals should therefore make every effort to narrow the gap between voiced and unvoiced dissatisfaction by making it easy for patients to file complaints and responding professionally to those complaints by providing service recovery.
Patients and families also serve as the “canary in the mine.” Murff found, for example, that admissions with surgical complications generate more complaints than surgical admissions without complications. Unsolicited complaints at times are the first (and sometimes only) notice of errors and sentinel events:
“I had a cystocele and a rectocele… After surgery I went for my checkup and she explained that it was my rectocele falling and now I had an enterocoele… she never repaired the rectocele during my first surgery… because she thought if she pulled everything up tight, it would take care of it… I am now faced with a third surgery for same problem.”
Additionally and as previously discussed, patient complaints may be used to identify and address professionals with a disproportionate share of complaints and at high malpractice claims risk. Vanderbilt’s Patient Advocacy Reporting System is a risk prevention tool that utilizes a reliable process to collect and code complaints and aggregate and analyze the data. The tool supports a risk prevention program in which professionals are made aware of their high numbers of complaints and associated high-risk status through a committee organized in accordance with the requirements of their state’s peer-review statutes.
Volunteer peer “messengers” are trained to conduct nondirective, nonjudgmental interventions with identified professionals and share individualized and local and national comparative data. The messenger asks his/her colleague to reflect on why he or she appears to stand out. The majority of professionals respond to peer-based intervention by reducing complaint numbers and claims risk.
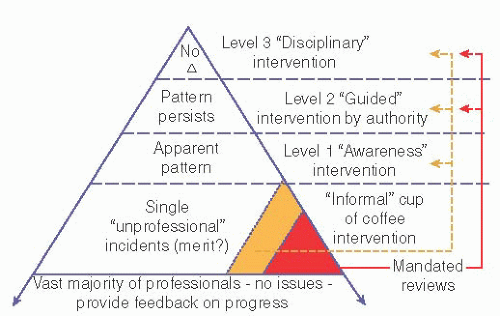
Follow-up data are provided at intervals to help professionals evaluate the effectiveness of self-directed changes in their practice or interactive style. As illustrated by the Promoting Professionalism Pyramid model (Fig. 4.3), if complaints continue after peer-based interventions, the professional is escalated to the next tier. An appropriate “authority figure” then develops a specific accountability action plan designed to assist the professional. The plan may include coaching, relevant continuing education, a practice review and redesign, and/or medical evaluation to rule out conditions that require further attention, such as substance abuse, psychiatric disorder, or cognitive impairment.
The Role of the Insurance Carrier and Risk Manager
As a gynecologic surgeon, reflect on your relationship with your malpractice carrier (or self-insured health system), risk manager, and any personal experience you may have had with claims. Identifying patterns and threats to safety helps professionals focus on education and resources where they can most favorably impact patient care and risk prevention.
Do your carrier and risk manager:
Encourage and make early reporting accessible?
Support risk management file review, RCAs, and MMM&Is?
Promote patient complaint collection, analysis, and intervention with high-risk individuals?
Offer on-site practice review to identify risk issues?
Incentivize you to adopt risk prevention procedures and participate in safety initiatives?
In spite of the best risk prevention strategies, some confluence of the human condition and systems failures interact in ways to create a risk event. Even so, it may be possible to identify early and respond in a way to avert the level of anger that can make managing risk more challenging.
The genesis of a potential lawsuit may begin before an AE occurs or is recognized. From the time a patient first calls a physician’s office for an appointment, or tries to find a parking space, the practice is either building credit or is creating debt with the patient:
In Ms. AJ’s case, Dr. GYN seemed professional at their first meeting, providing an explanation of her procedure and answering questions. Her postoperative experience created concern. Postdischarge, Ms. AJ’s frustration mounted.
At home (POD 4), Ms. AJ continues to have low abdominal discomfort. She feels her abdomen is swollen and experiences persistent back pain. Ms. AJ calls Dr. GYN’s office and asks to speak with him. Ms. NP returns the call. Ms. NP states she doubts symptoms are related to surgery. She promises to get back to Ms. AJ as soon as she has a chance to talk with Dr. GYN. Ms. AJ does not receive a callback that day. The next morning (POD 5), Ms. AJ leaves a voice mail as prompted by the office messaging system, asking if she can be checked by Dr. GYN because she is feeling “really bad.”
Ms. AJ does not hear back. That afternoon, Ms. AJ calls her primary care physician who suggests she go to the emergency department for evaluation. Dr. ED orders an abdominal CT scan with contrast. The study reveals extravasation of dye into the abdominopelvic region. An intravenous pyelogram (IVP) confirms leaking dye from the left ureter. Dr. ED calls Dr. GYN’s answering service. Dr. GYN’s partner calls back and asks Dr. ED to call a urologist to admit Ms. AJ because Dr. GYN is out of town and the patient will need a urologic procedure.
Ms. AJ is admitted. Dr. GYN is informed the next morning.
Once a professional realizes that his/her patient has experienced an AE, some thoughts may come to mind:
This is a recognized complication, right? (It was covered in the informed consent process….)
What do I say to my patient?
Should I report this to my practice leaders, risk manager, or malpractice carrier?
Do I have liability exposure? Will I be sued?
I wonder what Dr. ED and Dr. Urology are saying to my patient….
Could the “complication” have been identified sooner?
Knowing that the practice and/or health care organization is principled, “aims to do right” by patients and families, has the right tools to manage the situation, and offers guidance to team members, can help make an uncomfortable situation more tolerable for professionals. If your carrier or hospital does not offer information about a comprehensive approach to risk management after an event, you should ask what they do.
Dr. GYN goes to see Ms. AJ. She appears upset. Ms. AJ tells Dr. GYN that no one in his office listened when she reported continued discomfort, and she feels she should not have had to contact her primary care physician to get help; Dr. GYN did the surgery so he should have responded. She fears that the delay has led to a more serious problem. Ms. AJ also mentions that the urologist kept shaking his head when she told him how no one in Dr. GYN’s office seemed to take her seriously.
At the time an AE is recognized, the cause—complication? error? combination?—is often not clear. In some cases, objective review never fully elucidates the answer. Even if a professional is confident that what the patient is experiencing is a complication that happens under even the best of circumstances, patients and their families may still wonder if extra care might not have prevented the event. So, too, should the involved professional.
KEY POINTS: BEST PRACTICES FOR RISK MANAGEMENT AFTER AN AE
•
Coordinate care for the patient’s medical and emotional needs
•
Support emotional needs of involved team members
•
Notify your carrier or group or hospital risk manager if an error is identified, suspected, or unclear
•
If appropriate, dispatch trained individuals within the practice, group, or hospital to meet with the patient and family to assist with service recovery
•
Engage in a process of disclosure with the patient and offer an apology if error is identified. “Patient” includes family members or other parties authorized by the patient or legal guardians
•
Consider reimbursement of out-of-pocket expenses and early settlement offers. (This is done by risk management professionals.)
Coordinating Care for the Patient’s Medical Needs
After an AE, a professional should not delay care for his/her patient but does need to ask, “Do I need help in caring for the patient?” “Do I have the expertise to address the adverse outcome?” Do not be tempted to deliver care outside your usual scope of practice; arrange appropriate consultations from other professionals.
Furthermore, irrespective of whether you or another specialist manages the patient’s current medical needs, it is important that you do not abandon your patient. Continue to visit and follow the patient. If patients do not see their physician, especially after an AE with error, patients may believe you are avoiding them for one of two reasons: either you don’t care or you feel guilty.
Only gold members can continue reading. Log In or Register to continue