43 Premenstrual Syndrome Robert L. Barbieri The premenstrual syndrome (PMS) is defined as the presence of both physical and behavioral symptoms that occur repetitively in the luteal phase of the menstrual cycle and functionally interfere with some aspect of the woman’s life. Premenstrual dysphoric disorder (PMDD) is a severe form of PMS in which symptoms of irritability, anger, and emotional tension predominate over somatic symptoms such as bloating. The characteristic feature of both PMS and PMDD is the recurrent, cyclic nature of symptoms and a marked on/of nature of the symptoms that begin in the luteal phase of the menstrual cycle and completely remit after the cessation of menses. PMDD is distinguished from PMS by the predominance of mood symptoms, especially anger and irritability. PMS and PMDD cannot be diagnosed by histopathologic analysis of a tissue biopsy, nor by measurement of a serum analytes in the laboratory. PMS and PMDD are diagnoses based on the report of symptoms by the patient. There is no universally accepted method for diagnosing PMS and PMDD. Over the past decades, the diagnostic criteria used for these two entities have changed and evolved. It is likely that the diagnostic criteria for PMS and PMDD will continue to change. A widely used approach for diagnosing PMS is the stepwise algorithm recommended by investigators from the University of California, San Diego.
Definition
Diagnosis
| Afective symptoms | Somatic symptoms |
| Depression | Breast tenderness |
| Angry outbursts | Abdominal bloating |
| Irritability | Headache |
| Confusion | Swollen extremities |
| Social withdrawal | |
| Fatigue |
Source: From Mortola JF, Girton L, Yen SSC Am J Obstet Gynecol 1989;161:1682
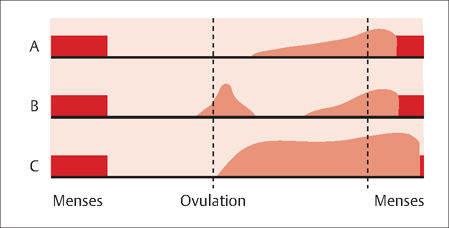
Fig. 43.1 Three patterns of premenstrual symptoms The red shading represents the timing and severity of the premenstrual symptoms In all three patterns, the symptoms are most prominent in the luteal phase of the menstrual cycle Pattern A represents a typical pattern with most symptoms during the second half of the luteal phase and symptom severity peaking late in the luteal phase In pattern B symptoms are also present around the time of ovulation Pattern C represents a severe example of premenstrual syndrome with symptoms throughout the luteal phase and extending into the first portion of menses, before subsiding during the following follicular phase.
PMDD is diagnosed based on the criteria in the Diagnostic and Statistical Manual of Mental Disorders, DSM-IV. To diagnose PMDD, the clinician needs to prospectively document that characteristic behavioral and physical symptoms are present for 1 week prior to menses and that the symptoms resolve within 5 days of the start of menses. Five symptoms must be present, and at least one symptom must be one of the first four on the list:
- feeling sad or hopeless
- feeling tense, anxious, or on the edge
- marked lability of mood interspersed with frequent tearfulness, and/or
- persistent irritability, anger, and increased interpersonal conflicts
Other symptoms that qualify include:
- decreased interest in usual activities
- difficulty concentrating
- feeling fatigued
- changes in appetite
- hypersomnia or insomnia
- being overwhelmed or out of control
- other physical symptoms such as breast tenderness or swelling, headaches, joint or muscle pain, bloating, or weight gain
Many women initially thought to have PMS or PMDD have marked symptoms during the follicular phase of the menstrual cycle, well after the cessation of menses. These women most likely have another problem such as an anxiety disorder or depression, rather than PMS or PMDD.
Prevalence and Epidemiology
Using strict definitions of PMDD and PMS, the prevalence of PMDD is reported to be about 4% and the prevalence of PMS has been reported to vary widely among different populations with rates in the range of 5–30%. Multiple studies have reported that premenstrual symptoms have a high degree of heritability. In addition, studies suggest that major depression and PMS are distinct disorders that overlap somewhat, but are not part of single continuum.
Etiology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


