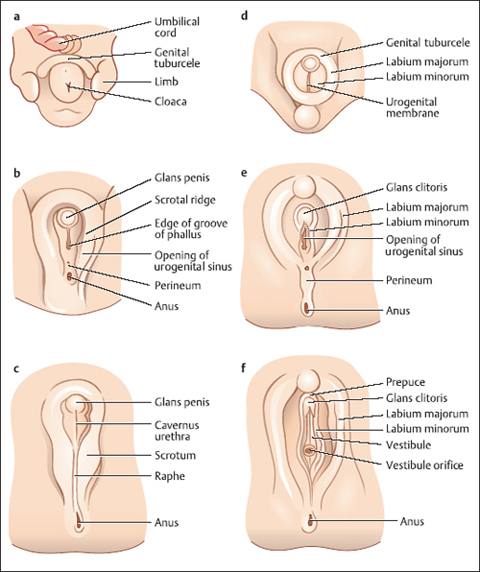
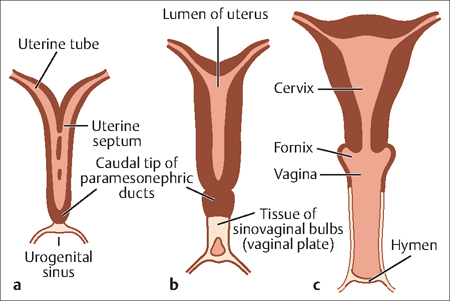
3 Embryology of the Female Reproductive System Shimrit Yaniv Sakem This chapter describes the normal development of the female reproductive system as well as the defects that sometimes occur in the female reproductive tract during embryogenesis. Agenesis: This term refers to failure of an organ to develop during embryonic growth and development. Many forms of agenesis are referred to by individual names, depending on the organ affected. Canalization: The production of a canal structure. External genitalia: These are comprised of the labia majora, labia minora, mons veneris (mons pubis) clitoris, vulvar vestibule and urethral meatus, and glandular structures opening to the vaginal vestibule. Hemivagina: This is a rare urogenital malformation characterized by a transverse vaginal septum. Internal genitalia: The internal genitalia include the uterus, cervix, ovaries, and fallopian tubes. Müllerian duct: The internal female sex duct, which forms on each side of a female embryo to connect the peritoneal cavity with the outside of the embryo. Embryogenesis of the genital tract occurs at 8 weeks of gestation. The external genitalia are derived from the genital tubercle (Fig. 3.1). The labial structures are of ectodermal origin; the urethra vaginal introitus and vulvar vestibule are derived from uroepethelial endoderm. Thus, the upper two-thirds are of müllerian origin, and the lower third is of urogenital sinus origin. The internal genitalia originate from the genital ridge. The embryologic ovaries migrate caudaly to the true pelvis. The primordial follicles remain dormant until adolescence. The müllerian ducts migrate caudally to form the fallopian tubes and fuse in the midline to create the uterus. A vertical midline septum is present until the end of the first trimester (Fig. 3.2), at which time it is reabsorbed. Failure of lateral fusion or of the septal reabsorption will result in what is referred to as müllerian duct anomalies (Fig. 3.3). Malformations of the external genitalia vary from vaginal agenesis, as can be found in Mayer-Rokitansky-Kuster-Hauser syndrome, through to failure of vaginal canalization. Failure of canalization might manifest as imperforated hymen, requiring further evaluation for transverse or lateral axis defects resulting in obstructed hemivagina or nonsignificant septa, which is found in up to 1 in 80 000 women. The incidence of uterine anomalies is between 1 in 100 and 1 in 1000 women. Clinical presentation might be primary amenorrhea, dysmenorrhea, a symptomatic pelvic mass; and more commonly, infertility, repeat abortions, and preterm labor. The most common uterine malformations are listed in Table 3.1. Fig. 3.1 Differentiation to male (a, c, e) and female (b, d, f) external genitalia. Fig. 3.2 Embryogenesis of female internal genitalia.
Definitions
Genital Embryogenesis
| Organ | Abnormality |
| Ovary | Duplication of ovary; secondary ovarian rests; paraovarian cysts (wolffan remnants) |
| Tube | Congenital absence; paratubal cyst (hydatid of Morgagni); hydrosalpinx-accumulation of serous fluid in the fallopian tube, often an end-result of pyosalpinx |
| Vagina |



