Case note
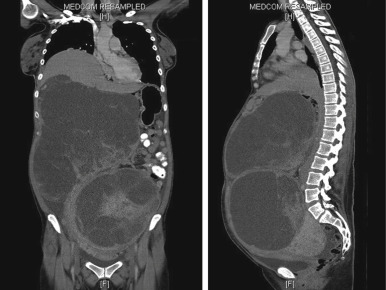
A 31-year-old nulliparous woman presented to the Gynaecology-Oncology service for the evaluation of progressive abdominal distension and early satiety over the preceding 2 years. Her menstrual cycles were regular with no abnormal uterine bleeding. She had no previous surgeries, and her family history was significant for breast and endometrial carcinoma. On examination, the abdomen was distended to the xiphisternum with a 40-week sized pelvi-abdominal mass without regional or supraclavicular lymphadenopathy. The cancer antigen 125 level was elevated at 430 units/mL, and computed tomography scan corroborated the presence of 2 large complex solid-cystic masses that appeared to be ovarian in origin ( Figure 1 ).
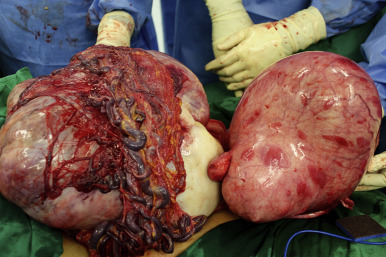
At laparotomy, however, the clinical suspicion of a bilateral ovarian neoplasm was quelled, because both ovaries appeared normal. Instead, a giant multilobulated abdominal mass was seen bathed in straw-colored ascites and adherent to the greater omentum via engorged, serpentine vessels ( Figure 2 ), in keeping with a parasitic leiomyoma. The uterus, which was separate from this mass, was enlarged irregularly by subserosal leiomyomas. An infracolic omentectomy was performed, which enabled the mass to be resected en-bloc.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


