Neck Mass
Frances Nadel
Monika Goyal
INTRODUCTION
Neck masses are a common clinical problem in children. Although the list of potential causes is extensive, most are due to benign processes that can be readily diagnosed after a complete history and physical examination. Close follow-up is important to ensure that less common causes in children such as malignancy are not overlooked.
Infectious Causes
Cervical Adenitis
Bacterial infection—Streptococcus pyogenes, Staphylococcus aureus, Group B Streptococcus, oral anaerobes, and Pasteurella multocida Cat scratch disease (Bartonella henselae)
Tularemia
Nocardia
Mycobacterium tuberculosis
Atypical mycobacterium
Reactive Adenopathy
Viral infection—upper respiratory viruses, mumps, measles, herpes virus, Epstein-Barr virus, cytomegalovirus, HIV
Bacterial infection—syphilis, brucellosis
Fungal infection—histoplasmosis, coccidioidomycosis
Parasitic infection—toxoplasmosis, filariasis
Other infections—head and neck infections (tonsillitis, otitis media, tinea capitis)
Lemierre’s Syndrome
Congenital or Vascular Causes
Thyroglossal duct cyst (TGDC)
Branchial cleft cyst
Cystic hygroma
Laryngocele
Dermoid
Cervical thymic cyst
Arteriovenous fistula
Neoplastic Causes
Malignant neoplasms—leukemia, Hodgkin lymphoma, non-Hodgkin lymphoma, rhabdomyosarcoma, fibrosarcoma, thyroid/parathyroid carcinoma, neuroblastoma, metastatic deposits
Benign neoplasms—lipoma, fibroma, neurofibroma, teratoma, osteochondroma, hemangioma
Metabolic or Genetic Causes
Goiter
Thyroid nodule
Traumatic Causes
Hematoma
Congenital muscular torticollis
Subcutaneous emphysema
Cervical spine fracture
Inflammatory Causes (Cervical Adenopathy)
Kawasaki syndrome
Systemic lupus erythematosus
Sinus histiocytosis
Sarcoidosis
Periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome
Toxic Causes
Drug-related adenopathy (e.g., phenytoin)
DIFFERENTIAL DIAGNOSIS DISCUSSION
Reactive Adenopathy
Familiarity with regional anatomy helps to narrow the differential diagnosis in a child who presents with a neck mass. Because most neck masses in infants and children are enlarged lymph nodes, it is important to be familiar with areas of lymphatic drainage. In addition, certain masses present in typical locations that help to identify the cause. The neck is divided into the anterior and posterior triangles, with the sternocleidomastoid muscle (SCM) forming the posterior border of the anterior triangle (Figure 54-1).
It is important to distinguish adenopathy from adenitis. Adenopathy is defined by nodal enlargement. In adenitis, the swelling is usually accompanied by signs of inflammation such as warmth, tenderness, and erythema. The vast majority of children with adenopathy have a benign viral or easily treatable bacterial cause. However, follow-up is important to assess resolution of symptoms and progressive reduction in size so as not to miss unusual infectious, inflammatory, or oncological processes. Moreover, any node >2 cm in diameter warrants further attention, as it falls outside the range of benign hyperplasia. A more detailed review of this topic is covered in Chapter 50, “Lymphadenopathy.”
 HINT: Epitrochlear, popliteal, supraclavicular, or occipital nodes in children <2 years are rarely due to benign lymph node hyperplasia. These nodes, as well as any palpable nodes in the newborn infant, deserve further investigation.
HINT: Epitrochlear, popliteal, supraclavicular, or occipital nodes in children <2 years are rarely due to benign lymph node hyperplasia. These nodes, as well as any palpable nodes in the newborn infant, deserve further investigation.Lemierre’s Syndrome
Lemierre’s syndrome (also known as necrobacillosis or postanginal sepsis) is a rare disease characterized by sepsis secondary to an anaerobic infection of the tonsillar or peritonsillar region and superficial thrombophlebitis of the internal jugular vein. It typically presents with prolonged pharyngitis or tonsillitis followed by lateral neck pain, swelling, and subsequent pulmonary symptoms. The most common bacteria isolated is Fusobacterium necrophorum. The key to diagnosis is having appropriate index of suspicion and confirmation by ultrasound, computed tomography (CT), or MRI demonstrating phlebitis of the internal jugular vein. Management consists of appropriate antibiotics and possible anticoagulation.
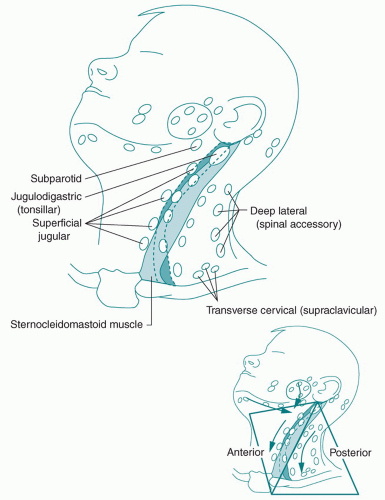 FIGURE 54-1 Division of the neck into anterior and posterior triangles.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|