Several systematic reviews draw attention to a relationship between medical or surgical evacuation of the uterus and subsequent preterm labor though do not suggest potential mechanisms. Saccone et al conclude that “Prior surgical uterine evacuation for either induced termination of pregnancy or spontaneous abortion is an independent risk factor for preterm birth. These data warrant caution in the use of surgical uterine evacuation and should encourage safer surgical techniques as well as medical methods.”
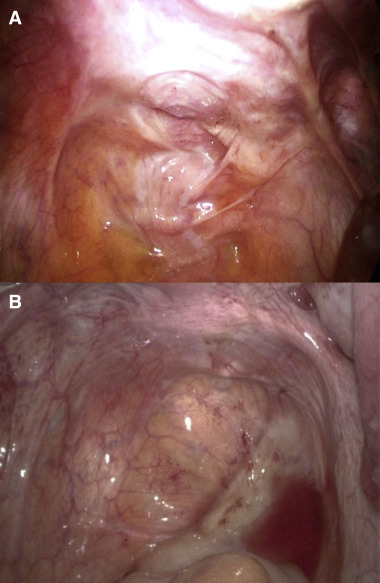
With the restrictive family planning policies in China in recent years, many women have had recurrent or “late” (>12 weeks), surgical or medical evacuations of the uterus. Both may result in injuries to the uterosacral ligaments and the uterovaginal nerves that run through the center of these ligaments. Excessive traction to the cervix during surgical evacuation may cause asymmetric injuries to these ligaments ( Figure , A) whereas excessive uterine activity associated with medical evacuation (10-15% of women in some series) may result in symmetric attenuation or complete absence of the uterosacral ligaments ( Figure , B). Concomitant injuries to vasomotor nerves result in narrowing of arterioles throughout the lower genital tract that is associated with many of the “great” obstetric syndromes including midtrimester loss, preterm labor, and preterm premature rupture of membranes. Medical evacuation complicated by excessive uterine activity may increase the risk of preterm labor compared to surgical evacuation (<12 weeks) in some groups of women. Many Chinese women experience high rates of subfertility, ectopic pregnancy, and pregnancy complications including preterm labor. We believe that denervation of the lower genital tract may create the conditions for “opportunist” infection and some forms of preterm labor. Other surgical interventions such as conization of the cervix may contribute to increasing rates of preterm labor through similar mechanisms. Both may be largely preventable.