The high rate of unintended pregnancies and the relatively high failure rates with the typical use of reversible methods of contraception are strong indications of a need for longacting contraceptive methods that simplify compliance. Two effective and popular methods are available, contraceptive implants (systems with the sustained release of a progestin) and depot-medroxyprogesterone acetate (Depo-Provera).
Injectable depot-medroxyprogesterone acetate is a long-acting (3 months) agent that has been part of the contraceptive programs of many countries for more than 25 years. This experience has demonstrated it to be safe, effective, and acceptable. It is not a “sustainedrelease” system, but its action is the same.
There are three major implant systems, Implanon, Norplant and Jadelle (formerly called Norplant-2). A Chinese version is called Sinoplant II. Both Jadelle and Sinoplant II contain 150 mg levonorgestrel. Unfortunately, Norplant was withdrawn from the U.S. market in a business decision dictated by profit and liability despite the fact that Norplant provided an excellent option for contraception. Jadelle is approved by the U.S. Food and Drug Administration, but it has not been marketed. In many parts of the world, Jadelle has replaced the use of Norplant; however, Norplant is still used worldwide.
Implanon differs from Norplant and Jadelle in many pivotal aspects, chiefly one rod instead of Norplant’s 6 capsules and Jadelle’s two rods, and a less androgenic progestin.1,2 Like Norplant, Implanon has been extensively marketed throughout the world with a good track record and high continuation rates. Contraceptive implants are approved in more than 60 countries and used by approximately 11 million women.2
The long-acting progestin methods are as effective as sterilization and IUDs, and more effective than oral and barrier contraception.3 An important reason for this high efficacy in actual use is the nature of the delivery systems themselves, which require little effort on the part of the user. Because compliance does not require frequent resupply or instruction in use, as with oral contraception, the actual or typical use effectiveness is very close to the theoretical (lowest expected) effectiveness.
Sustained-release methods require less of the user, but they demand more of the clinician. Implants involve minor operative procedures for placement and for discontinuation. Clinicians have a special responsibility to become skillful in the operations required to remove implants and to be available to women when those skills are required to terminate use. Disturbances of menstrual patterns and other side effects prompt many more questions from patients about these methods than about use of the familiar oral, intrauterine, and barrier contraceptives.4
Implant Systems
Norplant was developed by the Population Council and first approved in 1983 in Finland, where it was manufactured. It was approved in the U.S. in 1990, marketed in 1991, and withdrawn from the market in 2002.
Norplant is a “sustained-release” system using silastic tubing permeable to steroid molecules to provide stable circulating levels of synthetic progestin over years of use. The Norplant system consists of 6 capsules, each measuring 34 mm in length with a 2.4 mm outer diameter and containing 36 mg crystalline levonorgestrel. The capsules are made of flexible, medical-grade silastic (polydimethylsiloxane and methylvinyl siloxane copolymer) tubing that is sealed shut with silastic medical adhesive (polydimethylsiloxane). The 6 capsules contain a total of 216 mg levonorgestrel, which is very stable and remained unchanged in capsules examined after more than 9 years of use.
Jadelle was also developed by the Population Council and manufactured in Finland. It was approved in the U.S. in 1996, but never marketed. The thin, flexible Jadelle rods are wrapped in silastic tubing (the same material used by Norplant), 43 mm in length and 2.5 mm in diameter, thus slightly longer and thicker than Norplant.5 Each rod contains 75 mg levonorgestrel for a total of 150, 66 mg less than that in the 6 Norplant capsules. Whereas the levonorgestrel in Norplant is packed into the capsules in crystal form, the core of the Jadelle rod is a mixture of levonorgestrel and an elastic polymer (dimethylsiloxane/methylvinylsiloxane). Long-term clinical trials indicate that the performance and side effects are similar to Norplant, but removal is faster.6,7
Norplant average release rate:
First month
—
85 μg levonorgestrel daily
After 1 year
—
35 μg
After 2 years
—
30 mg
Jadelle average release rate:
First month
—
100 mg levonorgestrel daily
After 1 year
—
40 μg
After 2 years
—
30 mg
Because the release rates with the two levonorgestrel systems are comparable, it is reasonable to conclude that clinical studies with Norplant and Jadelle should yield similar results. In the discussion that follows, the more-studied product, Norplant, is often cited, but clinicians can assume that the findings apply as well to Jadelle.
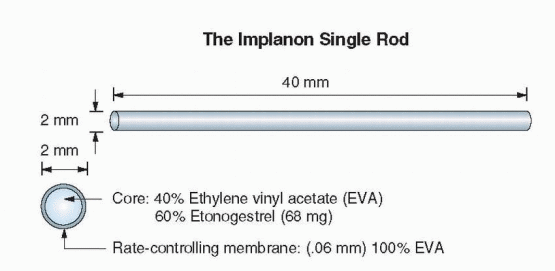
Implanon is a single flexible rod 4 cm long and 2 mm in diameter, that contains 68 mg of 3-keto desogestrel (etonogestrel, the active metabolite of desogestrel) dispersed in a core of ethylene vinyl acetate wrapped with a 0.6 mm thick membrane of the same material. There is no evidence that either ethylene vinyl acetate or silastic have toxic effects when implanted.8 The hormone is released at an initial rate of about 67 μg/day decreasing to 30 μg after 2 years; concentrations that inhibit ovulation are achieved within 8 h of insertion.9 A steady state is achieved after 4 months; after which there is a gradual decline.9 Implanon, placed subdermally with a disposable inserter, suppresses ovulation for 2.5 years, and provides effective contraception for at least 3 years. Side effects are similar to those with Norplant or Jadelle, except for less bleeding and a higher rate of amenorrhea with Implanon.10,11,12 and 13
Indications
Contraceptive implants are a good choice for women of reproductive age who are sexually active and desire long-term, continuous contraception. Implants should be considered for women who:
Want to delay the next pregnancy for at least 2-3 years.
Desire a highly effective, long-term method of contraception.
Experience serious or minor estrogen-related side effects with estrogen-progestin contraception.
Have difficulty remembering to take pills every day, have contraindications or difficulty using IUDs, or desire a non-coitus-related method of contraception.
Have completed their childbearing but are not yet ready to undergo permanent sterilization.
Have a history of anemia with heavy menstrual bleeding. Intend to breastfeed for a year or two.
Have chronic illnesses, in which health will be threatened by pregnancy.
Absolute Contraindications
Implant use is contraindicated in women who have:
ACTIVE thrombophlebitis or thromboembolic disease.
Undiagnosed genital bleeding.
ACUTE liver disease.
Benign or malignant liver tumors.
Known or suspected breast cancer.
Relative Contraindications
Based on clinical judgment and appropriate medical management, Implants MAY BE USED by women with a history of or current diagnosis of the following conditions:
Heavy cigarette smoking (15 or more daily) in women older than 35 years.
History of ectopic pregnancy.
Diabetes mellitus. Because multiple studies have failed to observe a significant impact on carbohydrate metabolism, Implants, in our view, are particularly well suited for diabetic women.
Hypercholesterolemia.
Hypertension.
History of cardiovascular disease, including myocardial infarction, cerebral vascular accident, coronary artery disease, angina, or a previous thromboembolic event. Patients with artificial heart valves.
Gallbladder disease.
Chronic disease, such as immunocompromised patients.
Implants are not contraindicated in the following situations, but other methods are preferable:
Severe acne.
Severe vascular or migraine headaches.
Severe depression.
Concomitant use of medications that induce microsomal liver enzymes:
Carbamazepine (Tegretol)
Felbamate
Lamotrigine
Nevirapine
Oxcarbazepine
Phenobarbital
Phenytoin (Dilantin)
Primidone (Mysoline)
Rifabutin
Rifampicin (Rifampin)
St. John’s wort
Topiramate
Vigabatrin
Possibly valproic acid, ethosuximide, griseofulvin, and troglitazone
We do not recommend the use of implants with any of the previously listed drugs because of a likely increased risk of pregnancy due to lower blood levels of the progestin.14,15
Mechanism of Action
The release rate of the contraceptive implants is determined by total surface area and the density of the implant in which the progestin is contained. The progestin diffuses from the implant into the surrounding tissues where it is absorbed by the circulatory system and distributed systemically, avoiding an initial high level in the circulation as with oral or injected steroids. Within 8 h after insertion of Implanon, plasma concentrations of etonogestrel are about 300 ng/mL, high enough to prevent ovulation.16 A study of cervical mucus changes with Norplant indicates that a backup method should be used for 3 days after insertion of Norplant or Jadelle; this is not necessary when Implanon is inserted as directed.17,18 Progestin concentrations are much more variable with Norplant and Jadelle than with Implanon.16
The Implanon rod releases 60 μg of etonogestrel per 24 h at 3 months of use. This rate declines gradually to 40-50 μg daily by 12 months and 30 μg/day by 2 years of use. The 85 mg of hormone released by Norplant or the 100 mg released by Jadelle during the first few months of use is about equivalent to the daily dose of levonorgestrel delivered by the progestin-only, minipill oral contraceptive, and 25-50% of the dose delivered by lowdose combined oral contraceptives. After 6 months of use, daily levonorgestrel concentrations are about 0.35 ng/mL; at 2.5 years, the levels decrease to 0.25-0.35 ng/mL. Until the 8-year mark, mean levels remain above 0.25 ng/mL.19 Mean plasma concentrations below 0.2 ng/mL are associated with increased pregnancy rates for Norplant (lower levels are more likely in heavier women).
Body weight affects the circulating levels of levonorgestrel; the greater the weight of the user, the lower the levonorgestrel concentrations at any time during Norplant or Jadelle use. The greatest decrease over time occurs in women weighing more than 70 kg (154 lb), but even for heavy women, the release rate is high enough to prevent pregnancy at least as reliably as oral contraceptives. In Implanon users, etonogestrel concentrations are affected very little by body weight, and failure rates did not increase with increasing body weight in the small numbers of overweight women in the clinical trials.20 Although the data with overweight women are limited, it is likely that Implanon is a good contraceptive choice for obese women.
Levonorgestrel levels can also be affected by the circulating levels of sex hormone-binding globulin (SHBG). Levonorgestrel has a higher affinity for SHBG than does etonogestrel. In the week after Norplant or Jadelle insertion, SHBG levels decline rapidly and then return to approximately half of preinsertion levels by 1 year of use. This effect on SHBG is not uniform and may account for some of the individual variations in circulating progestin concentrations.21
Implants are highly effective contraceptives. There are three probable modes of action, which are similar to those attributed to the contraceptive effect of the progestin-only minipills, but because daily dosing is not required, implants are more effective than oral methods.
The progestin suppresses, at both the hypothalamus and the pituitary, the luteinizing hormone (LH) surge necessary for ovulation. As determined by progesterone levels in many users over several years, approximately one-third of all cycles in Norplant users are ovulatory.19,22 During the first 2 years of use, only about 10% of women are ovulatory, but by 5 years of use, more than 50% are. In those cycles that are ovulatory, there is a high incidence of luteal insufficiency. Implanon inhibits ovulation throughout a 3-year period, accounting for almost all of the contraceptive effect.2 However, follicular development does occur, avoiding the problem of clinically significant hypoestrogenemia, and in the last 6 months of the 3-year period with Implanon, there is an occasional ovulation.16,23
The steady release of progestin has a prolonged effect on the cervical mucus. The mucus thickens and decreases in amount, forming a barrier to sperm penetration.17,23,24 and 25
The progestin suppresses the estradiol-induced cyclic maturation of the endometrium and eventually causes atrophy. These changes could prevent implantation should fertilization occur; however, no evidence of fertilization can be detected in Norplant users.26
Advantages
Implants are a safe, highly effective, continuous method of contraception that requires little user effort and, unlike long-acting injectable contraception, is rapidly reversible. Because this is a progestin-only method, it can be used by women who have contraindications for the use of estrogen-containing contraceptives. The sustained release of low doses of progestin avoids the high initial dose delivered by injectables and the daily hormone surge associated with oral contraceptives. Implants are an excellent choice for a breastfeeding woman and can be inserted immediately postpartum. There are no effects on breast milk quality or quantity, and infants grow normally.27,28,29 and 30 Another advantage of the implant method is that it allows women to plan their pregnancies precisely; return of fertility occurs within a few weeks, in contrast to the 6- to 18-month delay in ovulation that can follow depotmedroxyprogesterone acetate injections.16,31,32 and 33
One of the major advantages of sustained-release methods is the high degree of efficacy, nearly equivalent to the theoretical effectiveness. In couples for whom elective abortion is unacceptable in the event of an unplanned pregnancy, the high efficacy rate is especially important. There are no forgotten pills, broken condoms, lost diaphragms, or missed injections. For women who are at high risk of medical complications should they become pregnant, sustained-release implants present a significant safety advantage. Users should be reassured that implant use has not been associated with changes in carbohydrate or lipid metabolism, coagulation, liver or kidney function, or immunoglobulin levels. Because many women wanting implants will have had negative experiences with other contraceptives, it is important that the differences between this method and previous methods be explained.
Exposure of endometriosis to progestin-only contraceptive methods is an effective method to manage the pain associated with this condition. Implanon, depot-medroxyprogesterone acetate, and the levonorgestrel-containing intrauterine device have all been reported to reduce endometriosis pain.34,35,36,37 and 38
Disadvantages
There are some disadvantages associated with the use of the implant systems. Implants cause disruption of bleeding patterns, especially during the first year of use, and some women or their partners find these changes unacceptable.4 Endogenous estrogen is nearly normal, and unlike the estrogen-progestin contraceptives, progestin is not regularly withdrawn to allow endometrial sloughing. Consequently, the endometrium sheds at unpredictable intervals.
The implants must be inserted and removed in a surgical procedure performed by trained personnel. Women cannot initiate or discontinue the method without the assistance of a clinician. The incidence of complicated removals is approximately 5% for Norplant or Jadelle and lower for Implanon, an incidence that can be best minimized by good training and careful insertion.39,40 The implants can be visible under the skin. This sign of the use of contraception may be unacceptable for some women and for some partners.4
Implants do not provide protection against sexually transmitted infections (STIs) such as herpes, human papillomavirus, HIV, gonorrhea, or chlamydia. Although users may be less likely to use a second method because of the high contraceptive efficacy,41 users at risk for STIs must use condoms as a second method to prevent infection.
Because the insertion and removal of implants require minor surgical procedures, initiation and discontinuation costs are higher than with oral contraceptives or barrier methods. The cost of implants plus fees for insertion total an amount that may seem high to patients unless they compare it with the total cost of using other methods for up to 5 years.42 Nevertheless, short-term use is expensive compared with the relatively low initial costs of other reversible methods, and most women cannot be expected to use long-acting methods for their full duration of action.
Cultural factors can influence the acceptability of menstrual changes. Some cultures restrict a woman from participating in religious activity, household activities, or sexual intercourse while menstruating. All users must be aware of the possible menstrual changes. It is important to stress that all of the menstrual changes are expected, that they do not cause or represent illness, and that most women revert back to a more normal pattern with increasing duration of use.
Insertion and removal of implants will be a new experience for most women. As with any new experience, women will approach it with varying degrees of apprehension and anxiety. In reality, most patients are able to watch in comfort as implants are inserted or removed. Women should be told that the incisions used for the procedures are very small and heal quickly, leaving small scars that are usually difficult to see because of their location and size.
We encourage prospective users to see and touch implants. Women can be reassured that the implants will not be damaged or move if the skin above them is accidentally injured. Normal activity cannot damage or displace the implants. Most women become unaware of their presence. A few women report sensing the implants if they have been touched or manipulated for a prolonged period of time, or after vigorous exercise. The implants are more visible in slender women with good muscle tone. Darker-skinned users may notice further darkening of the skin directly over the implants; this resolves after removal.
Efficacy
Contraceptive implants provide highly effective birth control. In 2-year or 3-year studies in 11 international clinical trials of 942 women using Implanon, no pregnancies occurred.20 In studies of Norplant conducted in 11 countries, totaling 12,133 woman-years of use, the pregnancy rate was 0.2 pregnancies per 100 woman-years of use.15,31 All but one of the pregnancies that occurred during the Norplant evaluation were present at the time of implant insertion. If these luteal phase insertions are excluded from analysis, the first-year pregnancy rate was 0.01 per 100 woman-years. In adolescents, Norplant implants provide better protection against unwanted pregnancy, compared with oral contraceptives, and an important factor is the better continuation rate with Norplant.41,43,44
Failure Rates During the First Year of Use, United States3,45,46
Percent of Women with Pregnancy
Method
Lowest Expected
Typical
No method
85%
85%
Combination Pill
0.3%
8.7%
Progestin only
0.5%
3.0%
IUDs:
Levonorgestrel IUS
0.1%
0.1%
Copper T 380A
0.6%
1.0%
Implants:
Six levonorgestrel capsules (Norplant)
0.05%
0.2%
Two levonorgestrel rods (Jadelle)
0.06%
0.06
One etonogestrel rod (Implanon)
0.01%
0.01
Injectable
3-month
0.3
0.3%
1-month
0.05
3.0%
Patch
0.3
8.0%
Vaginal ring
0.3
8.0%
Female sterilization
0.5%
0.7%
Male sterilization
0.1%
0.2%
There are no weight restrictions for Norplant or Jadelle users, but heavier women (more than 70 kg) may experience slightly higher pregnancy rates in the later years of use compared with lighter women. Even in the later years, however, pregnancy rates for heavier women using Norplant are lower than with oral contraception. The differences in pregnancy rates by weight are probably due to the dilutional effect of larger body size on the low, sustained serum levels of levonorgestrel. Heavier women should not rely on Norplant or Jadelle beyond the 5-year limit. For slender women the duration of efficacy extends well past the fifth year of use. In some extended trials, no pregnancies have occurred into the seventh year. Data are not available regarding the effect of body weight on the efficacy of Implanon, but unlike Norplant and Jadelle, progestin levels are not significantly lower in heavier women.
The contraceptive efficacy of Implanon surpasses that of Norplant and sterilization.2 Only a rare pregnancy occurs, resulting in a Pearl Index of about 0.01.23,47 In over 70,000 cycles, no pregnancies were recorded because of total inhibition of ovulation until ovulations were observed in the last 6 months of the 3-year period.23,48 Post-marketing surveillance of pregnancies in Australia, where nearly one-quarter of contraceptors relied on Implanon in 2004, revealed that of 218 pregnancies, only 13 could possibly have been failures of the method.49 In Australia and the Netherlands, pregnancies commonly were the consequence of poor insertion technique, especially allowing the implant to fall unnoticed to the floor. Implants have an immediate contraceptive effect when inserted within the first 7 days of a menstrual cycle, but when insertion is after day 7, a backup method of contraception is necessary for at least 3 days.50
Ectopic Pregnancy
The ectopic pregnancy rate during Norplant use is 0.28 per 1,000 woman-years.15Although the risk of developing an ectopic pregnancy during use of Norplant is low, when pregnancy does occur, ectopic pregnancy should be suspected because approximately 30% of Norplant pregnancies are ectopic. Because Implanon is more effective in inhibiting ovulation, we would expect the risk of ectopic pregnancy to be considerably less than that associated with Norplant.
Ectopic Pregnancy Rates Per 1,000 Woman-Years15,51,52
Non-Contraceptive Users, all ages
3.0-4.5
Copper T-380 IUD
0.20
Norplant
0.28
Menstrual Effects
Menstrual bleeding patterns are highly variable among users of implant contraception. With levonorgestrel implants, some alteration of menstrual patterns will occur during the first year of use in approximately 80% of users, later decreasing to about 40%, and by the fifth year, to about 33%.53,54 The changes include alterations in the interval between bleeding, the duration and volume of menstrual flow, and spotting. Oligomenorrhea and amenorrhea also occur but are less common, less than 10% after the first year and diminishing thereafter. Irregular and prolonged bleeding usually occurs during the first year. Although bleeding problems occur much less frequently after the second year, they can occur at any time.54,55 Studies of the endometrium in Norplant users experiencing abnormal bleeding indicate the presence of enlarged venous sinusoids (fragile vessels) and a reduction in the expression of a protein factor (perivascular stromal cell tissue factor) involved in the initiation of hemostasis.56 Within weeks after insertion, the density of endometrial small blood vessels increases and the endometrium regresses to an atrophic state.57 It is believed that bleeding is a consequence of rapid endometrial regression and that the apparent increase in the number of blood vessels may reflect increased tortuosity accompanying the atrophic regression.
Implanon alters menstrual patterns, but amenorrhea occurs more often (21% of users in the first year, 30-40% after 1 year) than with Norplant.11,13 A single Implanon rod completely suppresses ovulation for 2.5 years, and, therefore, menses do not become more regular after the first 2 years as with Norplant. After 2 years, ovulation occurs in about half of the menstrual cycles. Bleeding is lighter and less frequent among Implanon users because more profound ovarian suppression results in less follicular estrogen production and less endometrial stimulation, nevertheless irregular bleeding continues to be a a major reason for discontinuation.13,58
Despite an increase in the number of spotting and bleeding days over preinsertion menstrual patterns, hemoglobin concentrations rise in Norplant users because of a decrease in the average amount of menstrual blood loss.59,60,61 and 62 Implanon likewise does not cause anemia.11
Implant users who can no longer tolerate prolonged bleeding will benefit from a short course of oral estrogen: conjugated estrogens, 1.25 mg, or estradiol, 2 mg, administered daily for 7 days.63 A therapeutic dose of one of the prostaglandin inhibitors given during the bleeding will help to diminish flow, but estrogen is the most effective treatment.64,65 Another approach is to administer an estrogen-progestin oral contraceptive for 1-3 months.66
Although implants are very effective, pregnancy must be considered in women reporting amenorrhea who had been ovulating previously, as evidenced by regular menses prior to an episode of amenorrhea. A sensitive urine pregnancy test should be obtained. Women who remain amenorrheic throughout their use of implants are unlikely to become pregnant.54 It is important to explain to patients the mechanism of the amenorrhea: the local progestational effect causing decidualization and atrophy.
Metabolic Effects
Exposure to the sustained, low doses of progestin delivered by the implants is not associated with significant metabolic changes. Studies of liver function,10,67,68 blood coagulation,10,69,70 and 71 immunoglobulin levels,72,73 serum cortisol levels,74 and blood chemistries68,72 have failed to detect changes outside of normal ranges in Norplant users.
No major impact on the lipoprotein profile can be demonstrated with Norplant.67,75,76 Minor changes are transient, and, with prolonged duration of use, lipoproteins return to preinsertion levels. Long-term exposure to the low dose of levonorgestrel released by Norplant is unlikely to affect users’ risk of atherogenesis, just as prolonged exposure to combined oral contraception has not. There are no clinically important effects on carbohydrate metabolism.72,7777,78 No effect on insulin sensitivity can be detected.79 In a cohort study of 5 years’ duration, no increase was observed in diabetes mellitus, depression, lupus erythematosus, cardiovascular diseases—in fact there was no increase in serious morbidity.80
There are no significant metabolic differences comparing Implanon and Norplant.81 Neither implant system has important clinical effects on the lipoprotein profile, carbohydrate metabolism, thyroid and adrenal function, liver function tests, or the clotting mechanism.10,58,82 Implant contraception is a good choice for a woman at risk for estrogen-associated thromboembolism. Because of the lower androgenic characteristic of etonogestrel, Implanon does not cause a decrease in the levels of sex hormone-binding globulin.82
Measurements of bone density in young women reveal that Implanon and Norplant do not affect the teenage gain in bone; similar gains in bone were recorded in implant users and control subjects.83,84 In older women, an increase in forearm, spine, and femur bone density has been documented after 6 and 12 months of Norplant use.85,86 An international crosssection study reported a small loss in bone density with Norplant that was rapidly regained after discontinuation.87
A slight increase in gallbladder disease has been noted in Norplant users.2,88 This is at best just a word of caution because the association is weak and may reflect preexisting disease, and there is no apparent biologic mechanism.
Effects on Future Fertility
Circulating levels of progestin become too low to measure within 48 h after removal of implants. Most women resume normal ovulatory cycles during the first month after removal. The pregnancy rates during the first year after removal are comparable with those of women not using contraceptive methods and trying to become pregnant. There are no long-term effects on future fertility nor are there any effects on sex ratios, rates of ectopic pregnancy, spontaneous miscarriage, stillbirth, or congenital malformations.15,31 The return of fertility after implant removal is prompt, and pregnancy outcomes are within normal limits. The rate and outcome of subsequent pregnancies are not influenced by duration of use.
For women who are spacing their pregnancies, the difference between implants and depot-medroxyprogesterone acetate in the timing of the return to fertility can be critical. Implants allow precise timing of pregnancy because the return of ovulation after removal is prompt. Etonogestrel serum levels are undetectable within one week after removal of Implanon, and ovulation can be expected in the first month after discontinuation.9 Depotmedroxyprogesterone acetate, on the other hand, can cause up to 18 months’ delay in return to fertility. By that time, 90% of users of either method will have ovulated, but in the first several months, the difference is dramatic. By 3 months after removal, half of implant users will have ovulated, but 10 months must elapse before half of depot-medroxyprogesterone acetate users are ovulatory.
Side Effects
The occurrence of serious side effects is very rare, no different in incidence than that observed in the general population. In addition to the menstrual changes, levonorgestrel implant users have reported the following side effects: headache, acne, weight change, mastalgia, hyperpigmentation over the implants, hirsutism, depression, mood changes, anxiety, nervousness, ovarian cyst formation, and galactorrhea.15,31,53,55,89
It is difficult, of course, to be certain which of these effects were actually caused by the levonorgestrel. For example, careful study fails to reveal a relationship between Norplant use and depressive symptoms.90 Although most of these side effects are minor in nature, they can cause patients to discontinue the method. Patients often find common side effects tolerable after assurance that they do not represent a health hazard.4 Many complaints respond to reassurance; others can be treated with simple therapies. The most common side effect experienced by users is headache (16% of Implanon users); approximately 20% of women who discontinue use do so because of headache.4,20,89
Stroke, thrombotic thrombocytopenic purpura, thrombocytopenia, and pseudotumor cerebri have been reported with Norplant.91 However, it is by no means established that the incidence of these problems is increased, and there is little reason to suspect a cause-andeffect relationship. In the follow-up study conducted by the World Health Organization in eight countries, no significant excess of cardiovascular events or malignant disease was observed.92
Weight Change
Women using levonorgestrel implants more frequently complain of weight gain than of weight loss, but findings are variable.88 In the Dominican Republic, 75% of those who changed weight lost weight, whereas in San Francisco, two-thirds gained weight. Assessment of weight change in Norplant users is confounded by changes in exercise, diet, and aging. Although an increase in appetite can be attributed to the androgenic activity of levonorgestrel, it is unlikely that the low levels with Norplant have any clinical impact. Counseling for weight changes focuses best on dietary review and dietary changes. Indeed, a 5-year follow-up of 75 women with Norplant implants could document no increase in the body mass index (nor was there a correlation between irregular bleeding and body weight).93 A similar experience has been documented with Implanon.12
Mastalgia
Bilateral mastalgia, often occurring premenstrually, is usually associated with complaints of fluid retention. After pregnancy has been ruled out, reassurance and therapy aimed at symptomatic relief are indicated. This symptom decreases with increasing duration of implant use, and occurs at a lower rate comparing Implanon (10% of users) with Norplant.12,20 The most effective treatments for mastalgia are the following: danazol (200 mg/ day), vitamin E (600 units/day), bromocriptine (2.5 mg/day), or tamoxifen (20 mg/day), but there are no studies of these treatments in implant users.
Galactorrhea
Galactorrhea is more common among women who have had insertion of the implants on discontinuation of lactation. Pregnancy and other possible causes should be ruled out by performing a pregnancy test and a thorough breast examination. Patients can be reassured that this is a common occurrence among implant and oral contraceptive users. Decreasing the amount of breast and nipple stimulation during sexual relations might alleviate the symptom, but if amenorrhea accompanies persistent galactorrhea, a prolactin level should be obtained.
Acne
Acne, with or without an increase in oil production, is the most common skin complaint among levonorgestrel implant users. The acne is caused by the androgenic activity of the levonorgestrel that produces a direct impact and also causes a decrease in sex hormonebinding globulin (SHBG) levels leading to an increase in free steroid levels (both levonorgestrel and testosterone).21 This is in contrast to combined oral contraceptives that contain levonorgestrel, in which the estrogen effect on SHBG (an increase) produces a decrease in unbound, free androgens. Etonogestrel implants are less commonly associated with acne because this progestin is less androgenic than levonorgestrel.12 Common therapies for complaints of acne include dietary change, practice of good skin hygiene with the use of soaps or skin cleansers, and application of topical antibiotics (e.g., 1% clindamycin solution or gel or topical erythromycin).
Ovarian Cysts
Unlike oral contraception, the low serum progestin levels maintained by implants do not suppress follicle-stimulating hormone (FSH), which continues to stimulate ovarian follicle growth in most users. The LH peak during the first 2 years of use, on the other hand, is usually abolished so that these follicles do not ovulate.22 However, some continue to grow and cause pain or they are palpated at the time of pelvic examination.94 Adnexal masses are approximately 8 times more frequent in Norplant users compared with normally cycling women. Because these are simple cysts (and most regress spontaneously within 1 month of detection), they need not be sonographically or laparoscopically evaluated.40 Further evaluation is indicated if they became large and painful or fail to regress. Regular ovulators are less likely to form cysts so the situation is likely to improve after 2 years of implant use. Etonogestrel implants suppress follicular development more profoundly; thus, ovarian cysts are less likely than with levonorgestrel implants.
Cancer
We can speculate on possible effects of implants based on our experience with oral contraceptives and depot-medroxyprogesterone acetate. The risk of endometrial cancer ought to be reduced. A study of the endometrial effects of Norplant failed to find any evidence of hyperplasia, even when levonorgestrel levels were low and endogenous estradiol production was normal.95 The risk of ovarian cancer is also probably reduced, and we would expect a greater effect with Implanon because it more effectively suppresses ovulation. Breast and cervical cancer effects will be difficult to assess because of confounding variables as they are with oral contraception and depot-medroxyprogesterone acetate. The low progestin dose of implants, however, would be unlikely to have effects different from other hormonal contraceptives. In a very large case-control study, neither depot medroxyprogesterone acetate nor implants were associated with an increase in the risk of breast cancer.96
Post-marketing Surveillance Study
A large 5-year follow-up study in developing countries confirmed the low pregnancy rates associated with Norplant, 0.23 per 100 woman-years for intrauterine pregnancy and 0.03 per 100 woman-years for ectopic pregnancy.92 When the women using Norplant were compared with women using nonhormonal methods of contraception and to the expected population rates, there was no excess of cancers, connective tissue diseases, or cardiovascular events. Importantly, the complaints of headache and mood disturbances (including anxiety and depression) were similar to those reported by women using oral contraceptives, although higher than for women using IUDs.
Insertion and Removal
The usual personal and family medical history and physical examination should concentrate on factors that might contraindicate use of the various contraceptive options. If a patient elects to use contraceptive implants, a detailed description of the method, including effectiveness, side effects, risks, benefits, as well as insertion and removal procedures, should be provided. Before insertion, the patient is asked to read and sign a written consent for the surgical placement of the implants. The consent reviews the potential complications of the procedure that include reaction to the local anesthetic, infection, expulsion of the implants, superficial phlebitis, bruising, and the possibility of a subsequent difficult removal.
Insertion can be performed at any time during the menstrual cycle as long as pregnancy can be ruled out. If the patient’s last menstrual period was abnormal, if she has recently had sexual intercourse without contraception, or if there are reasons to suspect pregnancy, a sensitive urine pregnancy test is a wise precaution. Based on cervical mucus changes, a backup method need be used no more than 3 days after insertion.18 Implants can be inserted immediately postpartum but certainly should be initiated no later than the third postpartum week in non-breastfeeding women and the third postpartum month in breastfeeding women. Acne and headache are less common in women who receive Norplant immediately postpartum, and there is no difference in postpregnancy weight loss compared with women who receive it 4-6 weeks later.97
Timing Summary
Insert anytime during the first 5 days of the menstrual cycle if hormonal contraception is not being used.
If hormonal contraception is being used, insert anytime during the hormone-free interval. If steroid contraception is used continuously, insert at anytime.
If progestin-only contraception is being used, insert on the same day the next progestin injection is due or an implant or intrauterine device is removed. With progestin-only oral contraception, insertion can be performed anytime.
Insert anytime within the first 5 days after an abortion or before the fourth week postpartum in nonbreastfeeding women.
Insert before the fourth postpartum month in breast-feeding women; however if access to contraception is limited, it is appropriate to insert an implant immediately postpartum.
No backup method is necessary if timing of insertion follows the above suggestions. If insertion occurs at other times, backup contraception is necessary for at least 4 days after insertion.
Patients should be questioned about allergies to local anesthetics, antiseptic solutions, and tape. A discussion about the technique of insertion and anticipated sensations is an important part of preparing the patient for the experience. All patients approach insertion with some degree of apprehension that can be decreased by detailed explanations and preparation.98,99
Selection of the site for placement of implants is based on both functional and aesthetic factors. Various sites (the upper leg, forearm, and upper arm) have been used in clinical trials. The nondominant, upper, inner arm is the best site. This area is easily accessible to the clinician with minimal exposure of the patient. It is well protected during most normal activities. It is not highly visible, and migration of the implants from this site has not been documented. The site of placement does not affect circulating progestin levels. Careful implant insertion is the key to trouble-free removal.
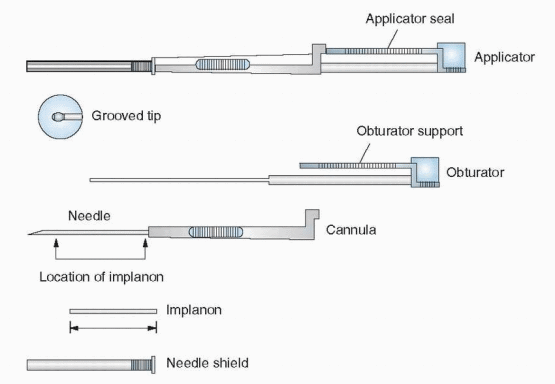
Implanon offers important insertion advantages compared with Norplant.100 Of course, only one rod simplifies and shortens both insertion and removal. In addition, a pre-loaded applicator is provided that facilitates placement. If necessary, Implanon can usually be visualized by ultrasonography.101 However, if a nonpalpable rod is not visible on ultrasonography, definitive localization is best achieved with magnetic resonance imaging (MRI).102 Removal of the Implanon rod uses the “fingers alone” technique with a 2 mm incision.103 Insertion complications (mainly deep insertions) are rare, and removal complications (difficulty finding the implant or a broken implant) occur at a far greater lower frequency compared with Norplant.1,100
Insertion Technique
Insertion is carried out under local anesthesia in the office or clinic by someone, usually a physician or nurse practitioner, trained in the technique described here.104 The procedure takes 5-10 min for a six implant system, and 2-3 min for a single implant.105
Required Equipment for Implanon Insertion
-2.5 mL syringe.
-0.5 inch, 25-gauge needle for injecting the anesthetic.
-1% chloroprocaine or lidocaine without epinephrine.
-Antiseptic solution.
-Adhesive strip for puncture closures.
-Elastic pressure bandage.
Positioning the Patient
The patient is placed in a supine position with the full length of her arm exposed. The upper inner arm is positioned by bending the elbow to 90 degrees and rotating the arm out, allowing full exposure of the insertion site at the crease between the biceps and triceps muscles. Adequate support under the arm should be provided to ensure comfort. To minimize the risk of infection, strict aseptic technique should be maintained throughout the procedure. An insertion site approximately 3-4 fingerbreadths (6-8 cm) superior and lateral to the medial epicondyle of the humerus is identified. A sterile drape is placed under the arm, and the insertion site on the arm is cleaned with an antiseptic such as povidone-iodine.
Anesthesia
Local anesthesia for the incision is obtained by raising a wheal of 1% chloroprocaine or lidocaine using a 25-gauge needle and injecting 1-2 mL under the skin along the track of the implant insertion needle.
Verify the presence of Implanon by looking carefully at the tip of the needle. If the implant (a white rod) is not visible, turn the applicator needle down and gently tap on a surface with the needle cover in place until the Implanon is seen, then tap the base of the applicator with the needle pointed up until the implant is no longer visible. Keep the applicator sterile.
Incision and Placement
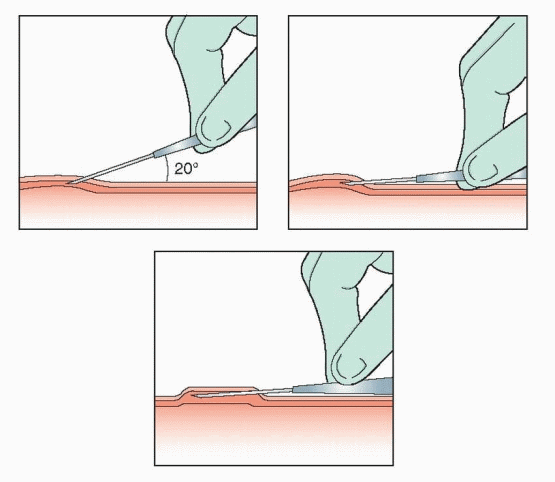
The insertion needle and its obturator can be pushed directly through the skin at no greater than a 20 degree angle without making an incision. The needle is advanced as superficially as possible under the skin by maintaining a slightly upward angle on the trocar. To minimize the chance of too deep an insertion, lift or tent the skin with the tip of the needle. If the skin dimples, the needle is too superficial. Pull the needle back and redirect. Advance the needle to its full length while applying counter traction to the skin at the insertion site.
Once the needle has been fully advanced, break the seal on the applicator by pressing the obturator support. Turn the obturator 90 degrees in either direction with respect to the cannula and fix the obturator with one hand. With the other hand, slowly pull the needle out of the arm, leaving the implant behind under the skin.
Immediately after insertion, palpate the implant to verify correct insertion (both ends should be palpable). Look for the grooved tip of the obturator visible inside the needle. If the implant is not palpable and not within the needle, it must be located before contraception can be assured. If placement is in doubt, another contraceptive method must be used. Ultrasonography is the easiest way to identify Implanon, which is not radio-opaque. If necessary, MRI can localize the implant.102
After the insertion, show the patient how to palpate the implant. Place an adhesive closure or bandage over the insertion site. Complete the patient chart label and the “User Card” that must be given to the patient.
Most women experience little pain during the insertion,98 but if it occurs the discomfort can be relieved with aspirin, acetaminophen, or a nonsteroidal anti-inflammatory agent. Infection or expulsion of the implants is rare (less than 1% with the Norplant system) and usually occurs when an implant is left pressing against the wound.106
The most commonly reported discomfort is a burning sensation during the injection of the local anesthetic. This effect of local anesthetic can be eliminated for most patients by adding 1 meq of sodium bicarbonate to each 10 mL of anesthetic (this shortens shelf life to 24 h).107 After the onset of anesthesia in 2-3 min, most women feel no more than a pressure sensation.
Complications of Insertion
Potential complications include infection, hematoma formation, local irritation or rash over the implants, expulsion of the implant, and allergic reactions to adhesives of the dressing. Implanon can migrate a short distance (less than 2 cm) over time.108 The incidence of complications is minimized by clinician training and experience, and the use of strict aseptic technique. Post-insertion pregnancies in Australia and the Netherlands were commonly due to a failure to insert the implant (allowing the implant to fall out prior to insertion). The clinician must make sure the implant is visualized in the trocar prior to insertion and after insertion is palpable under the skin.
Infection
The rate of infection varies among clinics and countries. The overall risk of infection after Norplant insertion is 0.8%.106 Infections usually occur within the first week after insertion, but can present as long as 4-5 months later. Infection can be treated either by the removal of the implant or the administration of oral antibiotics while the implant remains in place. One-third of insertion site infections treated with antibiotics are unresponsive to therapy and require removal.106 There have been no reports of infections leading to serious injury. Rarely, a superficial phlebitis develops. If it resolves over 1-2 weeks with heat and elevation of the arm, the implants need not be removed.
Expulsion
Expulsion of one or more of the implants occurs in 0.4% of Norplant users, usually within the first few months.106 The majority of expulsions are associated with concurrent infection at the insertion site. Another cause of expulsion is failure to advance the implants far enough from the incision, causing pressure on the incision by the distal tip of the implant.
Local Reactions
Although not common, hematomas can form. The use of a pressure dressing for 72 h will prevent enlargment. Application of an ice pack for 30 min immediately after insertion also helps. Local irritation, rash, pruritus, and pain occur in 4.7% of Norplant users, usually during the first month of use.106 Allergies to skin closure strip adhesives or to latex gloves account for some reactions.109 These problems resolve spontaneously, but itching can be relieved by topical corticoid steroids.
Removal Techniques
Although implant removal is an office procedure requiring only a small amount of local anesthesia and a few simple instruments, instruction and practice are necessary.107 Practicing on a model arm after viewing an instructional video makes first removals faster and less uncomfortable for both clinician and patient. A removal kit with a model arm, a manual, and compact disc illustrating the technique is available at no charge from Schering-Plough at 877-467-5266. As for insertion, the patient should read and sign an informed consent to be filed in her medical record. We recommend that the patient be given a copy.
Only gold members can continue reading. Log In or Register to continue