Number
Author; year; place
Number of patients
Years of study
Ethnicity
Age range at recruitment (years)
M:F
Morphology of lesions (%)
Oral mucosal involvement (%)
Nail involvement (%)
Scalp involvement (%)
1
Kanwar et al. [9]; 1991; India
17
1.5
Indian
8 months to 12 years
1.1:1
Classic (76), hypertrophic (12), eruptive (5.9)
5.9
5.9
11.8
2
Kumar et al. [2]; 1993; India
25
3
Indian
3–14
1.4:1
Classic (61), linear (14)
4
4
–
3
Sharma et al. [10]; 1999; India
50
3
Indian
7 monthsto 14 years
2:1
Classic (60), hypertrophic (26), linear (8), eruptive (4), annular (2), actinic (2)
30
–
–
4
Nanda et al. [1]; 2001; Kuwait
23
7
Kuwaiti 57 %, Bedouin 22 %, Egyptian 9 %, Saudi/Iraqi/Indian 4 % each
2.5–12
1.1:1
Classic (70), eruptive (13), linear (9), pigmented (4), actinic (4)
39
–
9
5
Handa et al. [11]; 2002; India
87
12.5
Indian
8 months to 12 years
1.1:1
Classic (60.9), actinic (11.5), hypertrophic (9.2), linear (9.2), eruptive (6.9), planopilaris (3.5), atrophic (1.1), bullous (1.1)
13.8
2.9
–
6
Luis-Montoya et al. [19]; 2005; Mexico
24
22.5
Mexican
3–15
1:1.2
Classic (43.5), linear (30.4), pigmented (13), actinic (4.3)
4.2
8.7
–
7
Nnoruka et al. [18]; 2007; Nigeria
13
4
African
3–15
1.5:1
Classic (61.5), hypertrophic (23.1), linear (15.4), eruptive (15.4)
23.1
7.7
–
8
Balasubramaniam et al. [6]; 2008; UK
26
11
Indian 80.8 %, Caucasian 15.4 %, Afro-Caribbean 3.8 %
3–16
1.6:1
Classic (84.6), linear (19.2), hypertrophic (7.7)
15.4
3.8
–
9
Kanwar et al. [3]; 2009; India
100
7.5
Indian
2–18
1.5:1
Classic (42), eruptive (19), linear (12), hypertrophic (8), actinic (5), pigmented (2), bullous (1)
17
19
–
10
Walton et al. [7]; 2010; USA
36
18
African-American 72 %, Caucasian 13.9 %, Hispanic 8.3 %, East Indian 2.6 %
4–18
1:2
Classic (67), hypertrophic (19), atrophic (8), linear (8), bullous (5.6), pigmented (2.8)
22
–
2.8
11
Pandhi et al. [4]; 2012; India
316
14.5
Indian
2–14
1.1:1
Classic (53.8), eruptive (16.5), hypertrophic (8.2), linear (6.9)
18
13.9
8.2
In the classic form of cutaneous LP, patients often complain of moderate to severe itch. This is the form that affects the overwhelming majority of children [3, 4]. The flexural aspects of the limbs are the most commonly affected sites. Individual lesions are polygonal, shiny, violaceous and flat-topped papules, and may be grouped together to form plaques (Figs. 32.1 and 32.2). Small delicate white streaks forming a network over the surface of these lesions, called Wickham’s striae, may also be seen. LP is a condition that demonstrates the Koebner phenomenon, whereby new lesions can appear on lines of trauma.


Fig. 32.1
Typical lichen planus lesions on the dorsal aspect of a patient’s wrist and hand
Fig. 32.2
Hypertrophic lichen planus lesions on a patient’s lower limb
Mucosal involvement in childhood LP is much less common than the 60 to 70 % incidence in adults [7, 9, 11, 19]. Previous case series have reported rates ranging between 4 and 39 % [1, 2]. All mucosal surfaces including the respiratory tract, gastrointestinal tract and genitalia can potentially be affected. Oral LP is subdivided into the following types: reticular, atrophic, bullous and erosive [20]. The reticular form is the most common type, and usually presents with painless white keratotic lesions with Wickham’s striae on the buccal mucosae bilaterally (Fig. 32.3). Less commonly, lesions may be found on the palate, tongue and lips [21]. On the other hand, atrophic, bullous and erosive type lesions cause burning sensations and pain. The atrophic form causes atrophic changes with erythema of the oral mucosa, while the bullous form manifests as fluid-filled vesicles and/or bullae. Erosive LP can result in painful ulcerated areas that may be complicated by secondary infection and scarring.
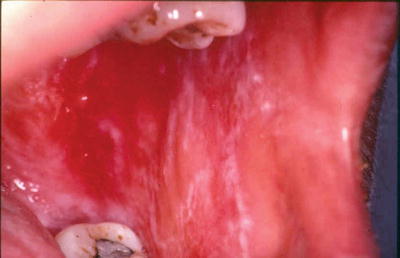
Fig. 32.3
Mucosal lichen planus with Wickham’s striae involving the buccal mucosa
Nail involvement occurs in up to 10 % of adult patients with LP, but is less common in the pediatric age group. Most prior studies have reported rates varying from 0 to 9 % [1, 7, 9–11, 13, 19]. However, more recent studies have found a higher incidence of nail LP in children (13.9 and 19 %) [3, 4]. Concomitant cutaneous or mucosal LP may not be present, and biopsy of the nail matrix is sometimes required to confirm the diagnosis [22]. In a major study on pediatric nail LP, Tosti et al. classified nail LP into three categories: typical nail LP, trachyonychia and idiopathic nail atrophy [23]. Typical nail LP can present in various ways: irregular longitudinal ridging and grooving of the nail plate, thinning of the nail plate, splitting or nicking of the nail margin, pterygium formation, onycholysis, subungual hyperkeratosis and red or brown discoloration. Trachyonychia is also called twenty-nail dystrophy, in which all nails are affected and show ridging and/or pitting, lack of lustre, splitting and roughening likened to sandpaper [24]. Idiopathic nail atrophy is seen only in children and refers to the rapid and diffuse destruction of nails over a few months [23].
Scalp LP is also known as follicular LP or lichen planopilaris. Keratotic plugs surrounded by violaceous erythema are seen on the scalp in this condition, and if untreated, can lead to scarring alopecia (Fig. 32.4) [1, 9].

Fig. 32.4
Scarring alopecia as a result of lichen planopilaris
Although LP is classically considered to be a papulosquamous eruption, there are many different variants. These include the actinic, annular, atrophic, bullous, erosive or ulcerative, eruptive, hypertrophic, linear and pigmented forms (Table 32.2). The eruptive, hypertrophic and linear types are the most common variants in children of color [3, 4]. Actinic LP and pigmented LP are more commonly seen in tropical countries such as India, possibly due to greater ultraviolet radiation exposure [6, 11, 13]. Another notable variant of LP is an entity termed lichen planus pemphigoides (LPP). This is a rare autoimmune condition in which patients have antibodies to type XVII collagen/bullous pemphigoid 180 antigen. While bullous LP is characterised by blister formation on pre-existing LP lesions, LPP is marked by the development of bullae on both lesional and normal skin [25–27]. Occasionally, LP can occur with other conditions and features of both disorders are present concurrently. Some examples include the lichen planus-lupus erythematosus and lichen planus-lichen sclerosus overlap syndromes [28, 29]. Lesions prominent in sun-exposed areas merit lupus screening.
Table 32.2
Variants of lichen planus
Variant | Characteristics |
|---|---|
Actinic | This presents as well-defined bluish-brown macules, patches or papules affecting sun-exposed surfaces, often with an annular configuration. Most cases occur in children and young adults, and have been reported from Africa, India, Italy and the Middle East. |
Annular | Annular LP usually occurs on the trunk and penis, and can be scattered amongst typical LP lesions. It is distinguished by a ring-like configuration of typical LP papules with a clear or slightly atrophic center. |
Atrophic | This variant could represent a resolving phase of LP, in which plaques demonstrate a central depression.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|