Gynecologic Traumas
Tracey Maurer
Gynecologic trauma can result from a variety of situations. Included in this discussion are sexually related trauma, trauma associated with women’s sports or leisure activities, and trauma that occurs from pelvic fractures.
SEXUALLY RELATED TRAUMA
A substantial body of literature addresses trauma from rape, as well as trauma occurring during consensual coitus (1,2,3,4,5,6,7,8,9,10). The major forms of sexually related trauma dealt with in the literature result from unexpected trauma occurring between consenting adults. Even though sexual abuse and its related trauma may be seen in emergency departments (EDs), abused women without life-threatening injuries or hemorrhage are generally evaluated in a well-controlled setting established for rape victims (1,2,3) (Chapter 26). Nevertheless, the gynecologic injuries that can occur during consensual and forced coitus are similar.
Women who are seen for emergency evaluation associated with sexually related trauma not only are in pain but also harbor feelings of embarrassment and anguish. In such a setting, compassion is as important as diagnostic acumen.
Trauma resulting from oral-genital sex can present in many ways. One finding seen in the oral cavity is referred to as fellatio syndrome. Erythema, petechia, purpura, and ecchymoses of the soft palate are seen (4). These are due to hemorrhage, possibly from repetitive negative pressure in the oral cavity, combined with the action of the tensor and levator veli palatini muscles, or solely from thrusting against the highly vascular soft palate (4). The lesions are painless, nonulcerative, and nonblanching (4). A history of fellatio can deter an extensive diagnostic workup, but a differential diagnosis includes paroxysmal coughing, sneezing, vomiting, infection, tumors, blood dyscrasias, and capillary fragility (4). Cunnilingus syndrome results from oral-genital sex in which the tongue is used on the partner’s genital areas (4). The findings are pain of the ventral surfaces of the tongue and throat with abrasions and ulcerations of the lingual frenulum (4). Chronic irritation can result in a traumatic fibroma on the frenulum (4).
Two possible, but rare, occurrences can be seen in the female recipient of oral-genital sex. One is a pneumoperitoneum. This can result after air is blown into the vagina, traverses the cervical canal and endometrial cavity, and enters the abdomen through the fallopian tubes (4). Cases have been reported in patients with their uterus in situ (4). Posthysterectomy cases have also been encountered, with the supposition that the air entered through a small dehiscence in the vaginal cuff (4,5). These patients generally have lower abdominal pain, upper quadrant pain, or shoulder pain (4). Peritoneal signs tend to be absent, allowing for conservative management (5). The clinical course is benign, with the air being gradually absorbed spontaneously. Cuff defects should be repaired when encountered (4,5).
Air embolism is the second complication seen in the female recipient of oral-genital sex. It is uniformly fatal (4). Death occurs rapidly, and resuscitative measures are usually too late. This complication has been reported in
seven gravid women, all at >20 weeks of gestation (4). Whether or not oral genital-related air embolism can occur in nonpregnant women is not known.
seven gravid women, all at >20 weeks of gestation (4). Whether or not oral genital-related air embolism can occur in nonpregnant women is not known.
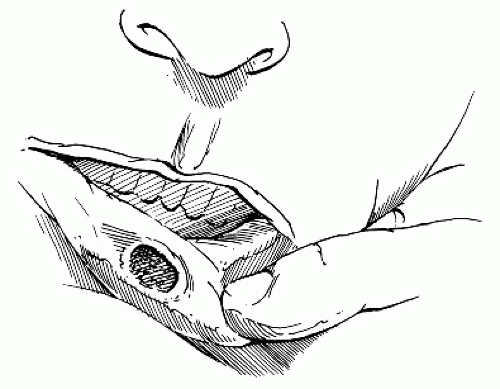 FIGURE 27.1 Chancre behind lip. |
Another possible, although rarely documented, complication of oral-genital sex is a vulvar hematoma from a human bite. One case report exists in the literature (11). Finally, oral-genital sex can lead to lesions of the oral cavity caused by sexually transmitted diseases. This should be kept in mind by the practitioner, so that information can be elicited from the patient (Fig. 27.1).
Trauma with coitus can range from hymenal tearing during initial intercourse to evisceration with hemorrhage. Small tears of the hymen are usually associated with minimal discomfort, but occasionally, profuse bleeding that requires repair can occur (4).
Vaginal lacerations and ruptures are rare, but when they are seen, it is usually in women of reproductive age who were having consensual intercourse (4,5,9). Metsala and Nieminen (9) found that approximately 88% of vaginal ruptures occurred during penile coital activity, with most of the remaining cases owing to other direct mechanical effects. The exact cause of the rupture often cannot be determined. Many predisposing factors have been suggested (4,7,9). In 1965, Purnell reported several cases of apparently spontaneous rupture of the vaginal vault (9). All of these cases were in postmenopausal women with vaginal atrophy. They occurred with sudden increases in intra-abdominal pressure during lifting, coughing, falling, or defecation. Purnell’s theory was that the sudden intra-abdominal pressure acted through the pouch of Douglas on a weakened posterior fornix to bring about a rupture. Women in both these situations generally had vaginal bleeding as the presenting symptom. Exsanguination has been reported (4,6,7). Sometimes, a history of sharp vaginal pain during intercourse is obtained (6,7). Surrounding structures may also be injured, and evisceration of abdominal contents has been seen (Fig. 27.2) (4,8).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


