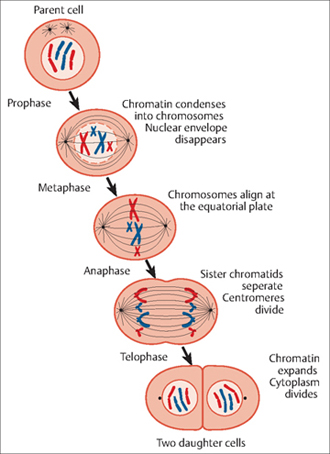
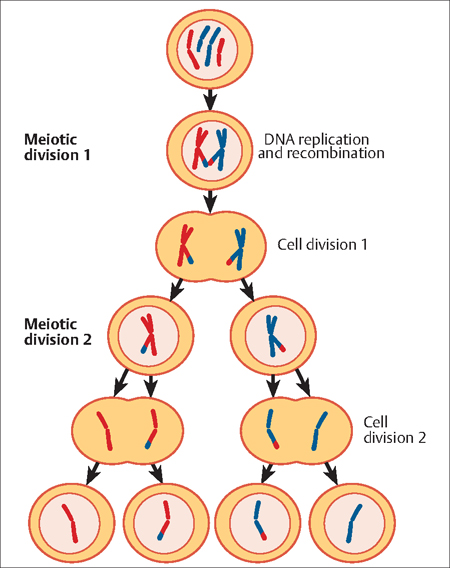
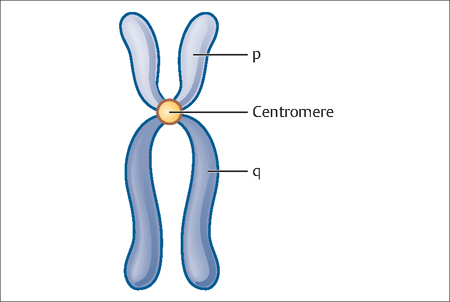
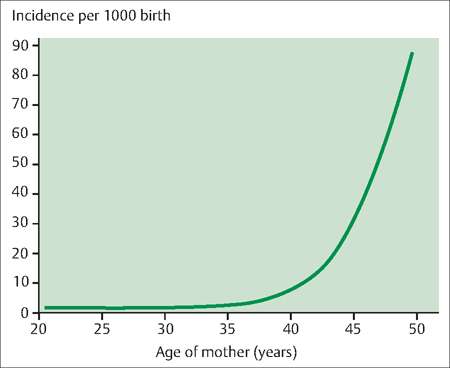
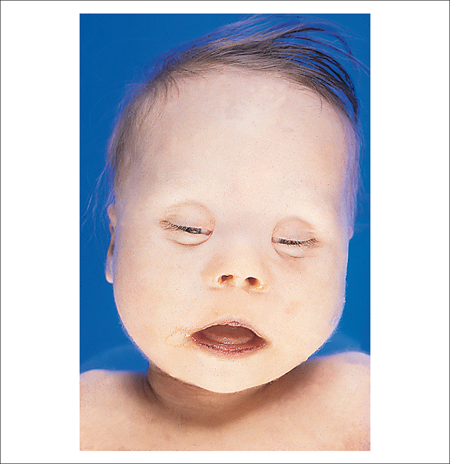
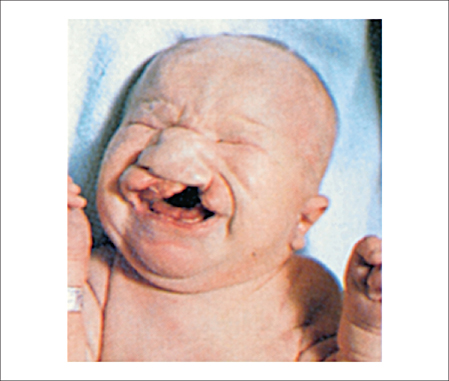
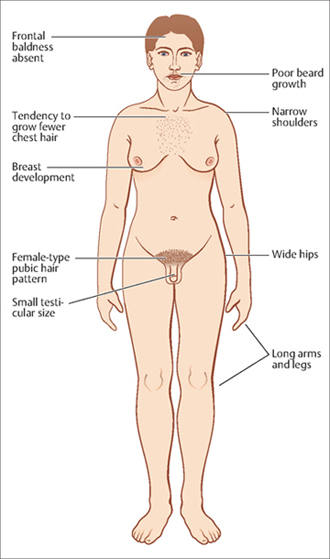
5 Genetics and Genomic Applications in OB/GYN Practice Arie Koifman and Arnon Wiznitzer The fundamentals of classic genetics were established by Gregor Johann Mendel (1822–1884), who elucidated the process of single-gene inheritance. Traditionally, “Mendelian” genetics was thus studied through relatively rare, single-gene diseases. However, a steadily growing body of evidence has suggested that multiple genes are involved in the vast majority of medical abnormalities. In fact, if neoplastic diseases are included, up to 90% of the general population will be affected during their lifetime by a disease with a multigene component. Traditionally, clinical geneticists have dealt with three main areas: 1) the diagnosis and management of pediatric patient abnormalities (including dysmorphology, chromosomal abnormalities, mendelian disorders, and other rare diseases); 2) prenatal genetic diagnosis and prenatal counseling; and 3) adult genetics (mainly the genetics of cancer). However, with recent advances in clinical knowledge—based on the enormous achievements in molecular genetics, genomics, and many other related disciplines— the field of clinical genetics is expanding rapidly. Furthermore, clinical geneticists must interact with an increasing diversity of other medical specialties, making a basic understanding of genetic and genomic concepts an essential tool for routine clinical practice. Autosome: This term refers to any paired chromosome that is alike in the cell of males and females, as distinguished from the two sex chromosomes X and Y. Humans have 22 pairs of autosomes. Cell nucleus: This is a membrane-enclosed structure found in most eukaryotic cells that contains most of the cell’s genetic material, which is organized as multiple, long, linear DNA molecules incomplexes with a large variety of proteins, such as histones, to form chromosomes. The genes within these chromosomes are the cell’s nuclear genome. The function of the nucleus is to maintain the integrity of these genes and to control the activities of the cell by regulating gene expression. Conceptus: This refers to all structures that develop from the zygote, both embryonic and extra-embryonic. It includes the embryo as well as the embryonic part of the placenta and its associated membranes: amnion, chorionic (gestational sac), and yolk sac. Chromosomes: These are the organized structures composed of DNA and proteins that are found in cells. A chromosome is a singular piece of DNA, which contains many genes, regulatory elements and other nucleotide sequences. Chromosomes also contain DNA-bound proteins, which serve to package the DNA and control its functions. Cytoplasm: This gelatinous, semitransparent fluid fills much of the volume of a cell. Eukaryotic cells contain organelles, such as mitochondria, that are filled with liquid which is kept separate from the cytoplasm by cell membranes. DNA: Deoxyribonucleic acid (DNA) is a complex molecule that contains the genetic instructions used in the development and functioning of all known living organisms and some viruses. The main role of DNA molecules is the long-term storage of information so that cells can make copies of themselves. Gamete: This describes a cell that fuses with another cell (gamete) during fertilization (conception) in organisms that reproduce sexually. In species that produce two morphologically distinct types of gametes, and in which each individual produces only one type, a female is any individual that produces the larger type of gamete—called an ovum (or egg)—and a male produces the smaller tadpolelike type—called a sperm. Gene: The functional and physical unit of heredity that passes from parent to offspring is called a gene. Genes are pieces of DNA, and most genes contain the information for making a specific protein. Gene expression: This is the process by which inheritable information from a gene, such as its DNA sequence, is converted into a functional gene product, such as a protein or ribonucleic acid (RNA). Genome: The complete package of genetic material of a living organism, organized in chromosomes, is known as the genome. A complete copy of the genome is found in most cells. Genotype: This defines the genetic constitution of a cell, an organism, or an individual. Haploid: This term refers to a set of chromosomes containing only one member of each chromosome pair. Human sperm and egg are haploid and have 23 chromosomes compared to a somatic cell, which is diploid and has 46. Karyotype: This is a pictorial representation of the chromosomes in a cell, which is used to check for abnormalities. A karyotype is created by staining the chromosomes with dye and photographing them through a microscope. The photograph is then cut up and rearranged so that the chromosomes are lined up into corresponding pairs. Mosaicism: This term describes the presence of two populations of cells with different genotypes in one individual, who has developed from a single fertilized egg. Pedigree: A pedigree is a diagram of family relationships that uses symbols to represent people and lines to represent genetic relationships. These diagrams make it easier to visualize relationships within families, particularly large extended families. Pedigree analyses are often used to determine the mode of inheritance (dominant, recessive, etc.) of genetic diseases. Phenotype: This term refers to any observable characteristic of an organism, such as its shape, development, biochemical or physiological properties, or behavior. Phenotypes are influenced by a combination of genetic and environmental factors. Sex chromosome: In females, the sex chromosomes are the XX chromosomes. Males have one X chromosome and one Y chromosome. The presence of the Y chromosome is decisive for unleashing the developmental program that leads to a baby boy. Translocation: This is a process by which chromosomes break and the fragments rejoin to other chromosomes, resulting in chromosomal abnormalities. Genetics has a profound impact on all different fields of OB/GYN patient care. Obstetricians must deal with genetic issues on a daily basis, such as in counseling women before pregnancy on how to prevent neural tube defects (NTDs), during pregnancy regarding screening tests for aneuploidy, ultrasonographic findings, and after pregnancy for risk assessment of future pregnancies Similarly, gynecologists routinely face genetic issues when seeking the etiology of recurrent miscarriages, the management of hydatidiform moles, and so on. Clinicians practicing reproductive medicine also deal with genetics in their daily medical practice, such as in managing infertility, delineating the etiology of infertility (e. g., chromosomal abnormalities, Turner syndrome, Klinefelter syndrome) as well as in preimplantation genetic diagnoses during in vitro fertilization. A basic knowledge of mitosis and meiosis is essential for the understanding genetics. The two processes are described briefy below. Mitosis is the process by which all the chromosomes in the nucleus duplicate themselves in order to generate two, identical, daughter nuclei. It is generally followed immediately by cytokinesis, which divides the nuclei, cytoplasm, organelles, and cell membrane into two daughter cells, each with the genetic equivalent of the parent cell (Fig. 5.1). Meiosis is a process of reduction division in which the number of chromosomes per cell is cut in half. In humans, meiosis always results in the formation of gametes and is essential for sexual reproduction. During meiosis, the genome of a diploid germ cell undergoes DNA replication followed by two rounds of division, resulting in four haploid cells. Each of these cells contains one complete set of chromosomes, or half of the genetic content of the original cell. Because the chromosomes of each parent undergo genetic recombination between homologous chromosomes during meiosis (Fig. 5.2), each gamete, will have a unique genetic blueprint encoded in its DNA. The genetic information in cells is arranged in several structural levels, from the basic DNA sequence to the chromosomes which are visible by light microscopy after staining. Basic chromosome structure consists of a short arm (p), long arm (q), and a centromere in between (Fig. 5.3). In 1985, a standard nomenclature for chromosomes was developed and named the International System for Human Cytogenetic Nomenclature (ISCN). In this ISCN nomenclature, each arm of a chromosome is divided into one to four major regions, depending on chromosomal length; each band, positively or negatively stained, is given a number, which rises as the distance from the centromere increases. Fig. 5.1 Mitosis consists of four distinct phases—prophase, metaphase, anaphase, and telophase—which result in the production of two genetically identical daughter cells Fig. 5.2 The process of meiosis in humans involves the halving of a cell’s chromosomes to form gametes for sexual reproduction Fig. 5.3 General structure of a chromosome showing the short arm (p), long arm (q) and the centromere which divides the two Chromosomes are grouped according to their size and the location of the centromere. Of a special interest are the acrocentric chromosomes (chromosomes 13, 14, 15, 21, 22), in which the short arm (p) is absent and there exists only a stalk in its place containing satellite DNA (i. e., highly repetitive, noncoding sequence). Translocations involving these chromosomes are called “robertsonian translocations” and are important in inheritance mechanism of chromosomal rearrangements (see below). There are several types of common genetic abnormalities, each resulting from a different mechanism. These include numerical abnormalities. Numerical abnormalities can be divided into two main categories: 1) aneuploidy—meaning a loss or addition of one (or in very rare occasions two) chromosome(s); and 2) polyploidy—meaning an addition of one or more set of chromosomes. The diseases in this group are quite common, and are well recognized and described. The aneuploidy group can be categorized into trisomies (meaning that cells have an extra copy of one of the chromosomes giving them three copies overall instead of two) and monosomies (a missing copy of one of the chromosomes). Trisomies can occur for each of the autosomes (i. e., chromosomes 1–22) or for each of the sex chromosomes (X or Y). All monosomies of autosomes are lethal and result in death before birth or immediately afterward. The only monosomy compatible with life is Turner syndrome, in which women are missing an X chromosome (see below). A normal female karyotype is labeled 46,XX; individuals with Turner syndrome are 45,X. In Turner syndrome, female sexual characteristics are present but generally underdeveloped (see below). The main reason 45,X females are able to survive the loss of one of an X chromosomes in each cell is that one of the two X chromosomes in each somatic cell of a female is typically inactivated early in the life of the embryo. This inactivated X chromosome is referred to as the “Barr body.” Recent genetic studies have demonstrated that although not all genes on the Barr body are inactivated, most are. Thus, X chromosome abnormalities are relatively benign compared with autosomal chromosomal abnormalities. An exception to this “rule of thumb” is the case of autosome/sex chromosome translocations, in which the translocated chromosome stays activated. Trisomy 21 (Down syndrome): Individuals who have all or part of an extra copy of chromosome 21 (i. e., trisomy 21) have significant physical and mental developmental problems. The condition is widely known as Down Syndrome. It is named after John Langdon Down, the British doctor who first described the syndrome in 1866. The overall incidence of Down syndrome among live births is about 1 in 800, but there is a marked variability depending on maternal age (Fig. 5.4). The vast majority (95%) of trisomy 21 is derived from an extra whole chromosome 21, which in most cases is due to maternal non-disjunction during meiosis. Other etiologies includes mainly “robertsonian” translocations (see below) between two acrocentric chromosomes and mosaicism (when two different cell types are present in a person). The Down syndrome phenotype includes marked hypotonia (low muscle tone), a protruding tongue, a small head with fattened occiput (back of the head), fat nasal bridge, and epicanthal folds with up-slanting palpebral fissures (separation between upper and lower eyelids) (Fig. 5.5). There is frequently loose skin at the nape of the neck, short fingers, a single palmar crease, and absence or hypoplasia of the middle phalanx, causing clinodactyly (inward curving) of the fifth finger, and the “sandal toe” gap. Fig. 5.4 The incidence of Down syndrome increases as the age of the mother increases and is nearly 10% by age 50 years Fig. 5.5 Babies with Down syndrome typically have a fattened nasal bridge and protruding tongue, among many other facial and physical abnormalities From: Riede UN, Werner M Color Atlas of Pathology Stuttgart: Thieme; 2004 Associated major abnormalities include heart defects (particularly endocardial cushion defects) in 30–40% of cases and gastrointestinal malformations. These children also have a high incidence of neonatal or childhood leukemia and thyroid disease. The intelligence quotient (IQ) ranges from 25 to 50, with a few individuals testing higher. Most affected children have social skills averaging 3–4 years ahead of their mental age. Life expectancy is decreased because of heart disease and susceptibility to acute leukemia. Most affected persons survive to adulthood, but the aging process seems to be accelerated, with death often occurring in the fifth or sixth decade. Fig. 5.6 A child with trisomy 13 showing the characteristic cleft lip Passarge E Color Atlas of Genetics, 3rd ed Stuttgart: Thieme; 2007 Trisomy 13 (Patau syndrome): Trisomies of chromosome 13 occur in about 1 in every 10 000 live births; about 80% of cases are complete trisomy 13 (i. e., they have a full extra chromosome). There is an increased risk of this condition with advanced maternal age. Characteristic symptoms in babies with trisomy 13 include midline anomalies, such as gross anatomical defects of the brain, especially holoprosencephaly; cleft lip and palate (Fig. 5.6), microphthalmi, colobomas (fissures) of the iris, and retinal dysplasia. Additionally, the supraorbital ridges (bony ridges above the eye) are shallow and the palpebral fissures usually are slanted. The ears are abnormally shaped and usually low-set. Deafness also is common. Infants with trisomy 13 tend to be small for gestational age. Simian crease, polydactyly, and hyperconvex narrow fingernails are common. About 80% of cases have severe congenital cardiovascular anomalies and dextrocardia (i.e, the heart is situated on the right side of the body) is common. Other midline defects include scalp defects and dermal sinuses. Loose folds of skin are often present over the posterior aspect of the neck. The genitalia are frequently abnormal in both sexes; cryptorchidism and an abnormal scrotum occur in the male, and a bicornuate uterus occurs in the female. Apneic spells in early infancy are frequent. Mental retardation is severe. Most patients (70%) do not survive more than 6 months, and less than 10% survive longer than 1 year. Trisomy 18 (Edwards syndrome): Trisomy 18 occurs in 1 in every 6000 live births. More than 95% of affected children have complete trisomy 18. Advanced maternal age increases the risk. The incidence is significantly higher in girls (75% vs. 25% for boys). Newborns with trisomy 18 are markedly small for their gestational age, with hypotonia and severe hypoplasia of skeletal muscle and subcutaneous fat. Their crying is weak, and they have a decreased response to sounds. The orbital ridges are hypoplastic, the palpebral fissures short, and the mouth and jaw small—all of which give the face a pinched appearance (Fig. 5.7). Microcephaly, prominent occiput, low-set malformed ears, and a short sternum are common. A peculiar clenched fist with the index finger overlapping the third and fourth fingers usually occurs. The distal crease on the fifth finger is absent, and there is a low-arch dermal ridge pattern on the fingertips. The fingernails are hypoplastic, and the big toe is shortened and frequently dorsifexed. Clubfeet and rocker-bottom feet are common. Severe congenital heart disease and anomalies of lungs, diaphragm, abdominal wall, kidneys, and ureters also are common, as are hernias and/or diastasis recti, cryptorchidism, and redundant skinfolds (particularly over the posterior aspect of the neck). Association with single umbilical artery is present. Survival for more than a few months is rare; less than 10% of such individuals are still alive at 1 year of age. Those who do survive have marked developmental delay and disability. 47,XXY (Klinefelter syndrome): Klinefelter syndrome is a sex chromosome abnormality that occurs in about 1 in 800–1000 of male live births. It involves the inheritance of two or more X chromosomes and one Y (i. e., 47,XXY), resulting in a male with female physical features. The extra X chromosome is maternal in origin in 60% of cases. Affected persons tend to be tall, with disproportionately long arms and legs (Fig. 5.8). They often have small, firm testes, and up to 30% develop gynecomastia. Puberty usually occurs at the normal age, but often facial hair growth is light. There is a predisposition for learning difficulties, and many have deficits in verbal IQ, auditory processing, and reading. Fig. 5.7 A baby with trisomy 18 displaying the characteristic pinched face From Passarge E Color Atlas of Genetics, 3rd ed Stuttgart: Thieme; 2007 Fig. 5.8 Individuals with Klinefelter syndrome often appear male but have many female features due to their inheritance of multiple X chromosomes and a single Y chromosome
Definitions
Impact of Genetics and Genomics on OB/GYN Practice
Basic Concepts of Genetics
Types and Mechanisms of Genetic Abnormalities
Numerical Abnormalities
Aneuploidies
Polyploidies

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


