As societies become more affluent, fertility decreases. This decrease is a response to the use of contraception and induced abortion. During her reproductive lifespan, the average !Kung woman, a member of an African tribe of hunter-gatherers, experienced 15 years of lactational amenorrhea, 4 years of pregnancy, and only 48 menstrual cycles.1 In contrast, a modern urban woman will experience 420 menstrual cycles. Contemporary women undergo earlier menarche and start having sexual intercourse earlier in their lives than in the past. Even though breastfeeding has increased in recent years, its duration is relatively brief, and its contribution to contraception in the developed world is trivial. Therefore, it is more difficult today to limit the size of a family unless some method of contraception is used.
Contraception is not new, but its widespread development and application are new. The era of modern contraception dates from 1960 when intrauterine devices were reintroduced and oral contraception was first approved by the U.S. Food and Drug Administration. For the first time, contraception did not have to be a part of the act of coitus. However, national family planning services and research were not funded by the U.S. Congress until 1970, and the last U.S. law prohibiting contraception was not reversed until 1973.
Today, more women younger than age 25 in the U.S. become pregnant than do their contemporaries in other Western countries.2,3 and 4 The U.S. teenage pregnancy rates are twice as high as those in England, Wales, and Canada, and 8 times as high as those of the Netherlands and Japan. The differences disappear almost completely after age 25. This is largely because American men and women after age 25 utilize surgical sterilization at a great rate.
It is not true that young American women want to have these higher pregnancy rates. About 82% of all pregnancies among American teenagers are unintended.5 Increasing effective contraceptive use among young Americans began to have an impact in 1991. In the 1990s, the teenage pregnancy rate reached the lowest rate since estimates began in 1976, a 21% decline from 1991 to 1997 for teenagers 15-17 years and a 13% decline for older teenagers.6 Overall, there was a 17% decline in teenage birth rates and a 12.8% decline in teenage induced abortions from 1991 through 1999. From 1995 to 2002,14% of the decline in teen pregnancy was a consequence of decreased sexual activity among U.S. teenagers; however, 86% of the decline was attributed to an increase in the use of effective contraception.7 In 2004, the proportion of induced abortions in the U.S. obtained by teens reached a low of 17%.8
After a 14-year 34% decline, birth rates for teenagers began to increase in 2005, the first increase since 1991. The rate increased 5% between 2005 and 2008.9 There is appropriate concern that this increase reflects difficulties in contraceptive access, affordability, and correct use. In addition, in recent years, fewer teens have received instruction regarding contraception.10 The evidence overwhelmingly indicates that abstinence programs have not had a positive impact on teen sexual behavior, including the delay of the initiation of sex or the number of sexual partners.11 In contrast, comprehensive sex education programs that include contraception are effective and do not increase the frequency of sex or hasten the initiation.12
Nearly half of all pregnancies (49%) in the U.S. are unplanned, and about 40% of these are aborted.5,13 American teenagers abort nearly half of their pregnancies, and this proportion is similar to that seen in other countries.13 But older American women, aged 20-34, have the highest proportion of pregnancies aborted compared with other countries, indicating an unappreciated, but real, problem of unintended pregnancy existing beyond the teenage years. In fact, American women older than age 40 have had for the last two decades a high ratio of abortions per live births, a ratio very similar to that of teenagers.8
Delaying marriage prolongs the period in which women are exposed to the risk of unintended pregnancy. This, however, cannot be documented as a major reason for the large differential between young adults in Europe and the U.S. The available evidence also indicates that a difference in sexual activity is not an important explanation. The major difference between American women and European women is that American women under age 25 are less likely to use any form of contraception. Significantly, the use of oral contraceptives (the main choice of younger women) is lower in the U.S. than in other countries.
Why are Americans different? The cultures in areas such as the U.K. and the Scandinavian countries are certainly very similar with similar rates of sexual experience. A major difference must be attributed to the availability of contraception. In the rest of the world, contraceptive services can be obtained from more accessible resources and relatively inexpensively. Major American problems are the enormous diversity of people and the unequal distribution of income in the U.S. These factors influence the ability of our society to effectively provide education regarding sex and contraception and to effectively make contraception services available.
Efficacy of Contraception
A clinician’s anecdotal experience with contraceptive methods is truly insufficient to provide the accurate information necessary for patient counseling. The clinician must be aware of the definitions and measurements used in assessing contraceptive efficacy and must draw on the talents of appropriate experts in this area to summarize the accurate and comparative failure rates for the various methods of contraception. The publications by Trussell et al., summarized below, accomplish these purposes and are highly recommended.14,15,16,17 and 18
Definitio and Measurement
Contraceptive efficacy is generally assessed by measuring the number of unplanned pregnancies that occur during a specified period of exposure and use of a contraceptive method. The two methods that have been used to measure contraceptive efficacy are the Pearl index and life-table analysis.
The Pearl Index
The Pearl index, created by Raymond Pearl in 1933, is defined as the number of failures per 100 woman-years of exposure.19 The denominator is the total months or cycles of exposure from the onset of a method until completion of the study, an unintended pregnancy, or discontinuation of the method. The quotient is multiplied by 1,200 if the denominator consists of months or by 1,300 if the denominator consists of cycles.
With most methods of contraception, failure rates decline with duration of use. The Pearl index is usually based on a lengthy exposure (usually 1 year) and, therefore, fails to accurately compare methods at various durations of exposure. This limitation is overcome by using the method of life-table analysis.
Life-Table Analysis
Life-table analysis calculates a failure rate for each month of use. A cumulative failure rate can then compare methods for any specific length of exposure. Women who leave a study for any reason other than unintended pregnancy are removed from the analysis, contributing their exposure until the time of the exit.
Contraceptive Failures
Contraceptive failures do occur and for many reasons. Thus, “method effectiveness” and “use effectiveness” have been used to designate efficacy with correct and incorrect use of a method. It is less confusing to simply compare the very best performance (the lowest expected failure rate) with the usual experience (typical failure rate) as noted in the table of failure rates during the first year of use. The lowest expected failure rates are determined in clinical trials, in which the combination of highly motivated subjects and frequent support from the study personnel yields the best results. Contraceptive typical failure rates have been estimated using the data from the 1995 and 2002 U.S. National Survey of Family Growth, correcting for the underreporting of induced abortion.17,18,20
The 2002 estimates of failure were not significantly different compared with the previous estimates from the 1995 national survey. Women over the age of 30 were less likely to experience failure than young women; teens were more than twice as likely to experience a failure than older women. Hispanic women and even more so, black women, experienced higher failure rates. Groups that were less likely to experience contraceptive failure were women who did not intend to have a subsequent birth and women who had no previous births. Married women experienced the lowest failure rates and cohabiting women the highest. The most important determinants of pill failure, therefore, were: age, intention toward a future birth, parity, and marital status. Interestingly, once these factors were accounted for, duration of use, race, ethnicity, and poverty status no longer affected the risk of pill failure. The same factors influence condom use, but when corrected for these factors, race, ethnicity, and poverty affected the risk of condom failure.
This is a subject of great interest because the rate of unintended pregnancies in the U.S. continues to be high. About one-half (over 3 million) of all pregnancies in the U.S. are unintended, and in 2002 about 53% of those occurred in women using a method of contraception.5,13,21 Here is a more striking statistic: one of every two American women aged 15-44 has experienced an unintended pregnancy.13
Failure Rates During the First Year of Use, United States17,18,20
Percent of women with pregnancy
Method
Lowest Expected
Typical
No method
85%
85%
Combination Pill
0.3%
8.7%
Progestin only
0.5%
3.0%
IUDs:
Levonorgestrel IUD
0.1%
0.1%
Copper T 380A
0.6%
1.0%
Implant
0.05%
1.0%
Injectable
3-month
0.3
0.3%
1-month
0.05
3.0%
Patch
0.3
8.0%
Vaginal ring
0.3
8.0%
Female sterilization
0.5%
0.7%
Male sterilization
0.1%
0.2%
Spermicides
18.0%
29.0%
Periodic abstinence
25.3%
Calendar
9.0%
Ovulation method
3.0%
Symptothermal
2.0%
Post-ovulation
1.0%
Withdrawal
4.0%
18.4%
Cervical cap
Parous women
26.0%
32.0%
Nulliparous women
9.0%
16.0%
Sponge:
Parous women
20.0%
32.0%
Nulliparous women
9.0%
16.0%
Diaphragm and spermicides
6.0%
16.0%
Condom
Male
2.0%
17.4%
Female
5.0%
27.0%
Contraceptive Use in the United States
The National Survey of Family Growth is conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention. Data are available from 1972, 1976, 1982, 1988, 1995, and 2002.21,22,23,24,25 and 26 The samples are very large; therefore, the estimates are very accurate.
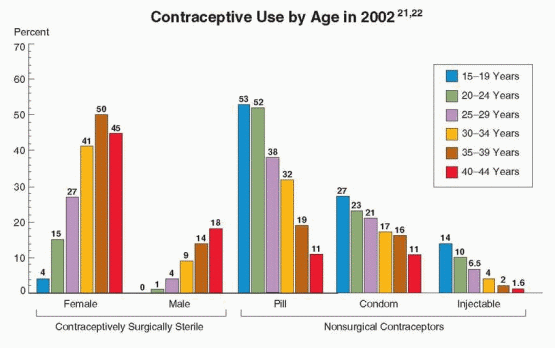
Pregnancy rates in the 1990s declined for women younger than age 30 years and increased in older women. From 1990 to 1997, the decrease in women in their early twenties was 8%, and the increase in women in their early thirties was 3%. The percent of married couples using sterilization as a method of contraception more than doubled from 1972 to 1988, and has remained stable since then. The use of oral contraception reached a high in 1992, slightly decreased in 1995, especially among Hispanic and black Americans, and returned to 31% of contracepting women in 2002. Approximately 10.7 million American women used oral contraceptives in 1988, and 11.6 million in 2002. Among never married women and women under age 25, oral contraception is the leading method of birth control. About 53% of contracepting women under age 25 were using oral contraception in 2002. From 1988 to 2002, oral contraception rose among women aged 30-44 to 32% of contraceptors aged 30-34, and 11% aged 40-44. About 5.3% of contraceptors in 2002 were using the 3-month injectable method, and 1.2% transdermal, vaginal ring, and implant methods.
In the 1990s, there was an increase in condom use by never married and formerly married women, women younger than 25, black women, and Hispanic women. These changes reflected the concern regarding sexually transmitted infections, including human immunodeficiency virus (HIV). But in 2002, the use of condoms alone returned to the level observed in the 1980s, probably because of the use of transdermal, vaginal ring, implant, and injectable methods. About one-third of condom users in 2002 were using more than one method, especially younger and never married women, including use of an oral contraceptive and a condom in 14% at first intercourse! Most importantly, the percentage of women who used a contraceptive method at their first premarital intercourse increased from 43% before 1980 to 79% in 2002. Condom use at first intercourse increased from 22% before 1980 to 67% in 2002.
In 1982, 56% of U.S. women, 15-44 years of age, were using contraception, and this has increased to 62% (about 40 million women). In 2002, contraceptive sterilization (male and female) was utilized by 36% of these women (the next leading method was oral contraception, 31%). The number of reproductive-aged women using the intrauterine device (IUD) decreased by two-thirds from 1982 to 1988 and further decreased in 1995, from 7.1% to 2% to 0.8%, respectively, but rose to 5% in 2008. IUD use is concentrated in the U.S. in married women older than age 35. In 1982 more than 2 million women (about 8% of contraceptors) used the diaphragm, but use of the diaphragm has nearly disappeared in the U.S. (0.3% of contracepting women in 2002).
The oral contraceptive (53%) and condoms (27%) are the most popular methods among teenagers. However, studies have repeatedly documented that the use of the implant and injectable methods is associated with lower discontinuation rates and a lower rate of repeat pregnancies following delivery.27,28 This warrants continuing efforts to extend the use of these methods.
In 2002, 62% of all women 15-44 years of age were using some method of contraception, whereas 38% of women of reproductive age were not using a method of contraception for the following reasons:
18.1%
—
Not sexually active.
9.5%
—
Pregnant or trying to get pregnant.
1.6%
—
Male and female sterility.
1.5%
—
Sterilized for medical reasons.
7.4%
—
At risk for an unintended pregnancy.
The women at risk for an unintended pregnancy increased by 1.43 million women (2.2%) from 1995 to 2002, and the increase was in all age groups. These women accounted for more than half of unintended pregnancies in the U.S.; of the rest, about 43% are a consequence of incorrect contraceptive use; only 5% can be attributed to method failure.13,18 This increase alone in women at risk and not using contraception, therefore, would amount to about 500,000 unintended pregnancies and 270,000 induced abortions in 2002. In our view, these numbers reflect problems of contraceptive access, affordability, and correct use in the U.S. The number of unintended pregnancies is highest among low-income women, women who have not completed high school, women aged 18 to 24, unmarried, especially cohabiting, women, and members of racial or ethnic minority groups.5
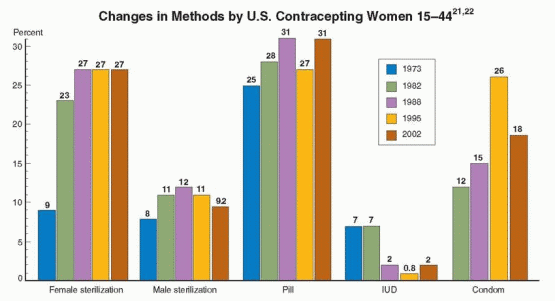
U.S. couples have made up for the lack of contraceptive effective use and availability by greater reliance on voluntary sterilization. Between 1973 and 1982, oral contraception and sterilization changed places as the most popular contraceptive method among women over the age of 30. Approximately one-half of American couples choose sterilization within 15 to 20 years of their last wanted birth. During the years of maximal fertility, oral contraceptives are the most common method peaking at age 20-24. The use of condoms is the second most widely used method of reversible contraception, rising from about 9% in the mid-1980s to approximately 26% of contracepting women in 1995, decreasing to 18% in 2002.21,22
Overall use of contraception among women at risk of unintended pregnancy decreased from 92.5% in 1995 to 89.3% in 2002.18 The use of contraception among poor women at risk of pregnancy decreased from 92.1% in 1995 to 86.3% in 2002. For various reasons, American women have had increasing difficulty in obtaining effective contraception.
Women at each end of the economic spectrum, the poorest and the wealthiest, experienced a decrease in failure rates from 1995 to 2002, although the poorest women continued to have a higher failure rate than did the better-off women. Also, although the difference in overall failure rate was not statistically significant comparing 1995 and 2002, there was about a 2.5% improvement; this missed mathematical significance but it may reflect a meaningful change in our population. This change is probably due to an increase in pill and injectable methods and a decrease in condom use during this period of time. Women living in poverty who must rely on condoms or withdrawal (male-dependent methods) have about a 2-fold increase in failure rates, but if they can use the pill, their failure rates are the same as betteroff women. The message is clear: we need to make the more effective methods available for poor women.
What do women have to do to achieve good contraceptive efficacy, and if they are already using a method, to switch to a more effective one? Choices must be available for various methods. The technique of using a method must be compatible with an individual and her lifestyle. Some methods require partner cooperation. Once chosen and obtained, the individual must exert dedication to its use. The failure to substantially improve contraceptive failure rates from 1995 to 2002 indicates that we are not making enough progress with each of these variables.
It is not enough to say the obvious—that we need greater education—but we need to learn where and when education is most effective, where is money best spent, and how to maximize the choices available for all women. This isn’t a task just for professional health care providers; it is a widespread social problem that requires policy and budgeting decisions. The problems are more sociologic, such as cost and insurance coverage (and the ridiculous insurance practice of providing pills only one month at a time). These are reasons why other countries have lower percentages of women at risk for unintended pregnancies.
The pattern of contraceptive use in Canada is similar to that of the U.S., with a similar percentage of oral contraceptive use (about 43% of women 15-44 years of age) and a slightly lower use of sterilization.29,30 Canada, too, has seen an increase in condom use and a decrease in use of the IUD. In England, the primary method of contraception is oral contraception (28%) followed by condoms (24%), the IUD (4%), and injectable methods (3%); 7% of the reproductive-aged women and 10% of the men have been sterilized.31 In France, 49% of reproductive-aged women use oral contraceptives, and although IUD use has slightly decreased (only among younger women), French women use the IUD at a rate that is more than 16-fold greater compared with North American women.32,33 Most French women use oral contraceptives when young and then turn to the IUD in their older years (only 4.1% of French women relied on sterilization; male sterilization is virtually nonexistent).
The Impact of the Worldwide Use of Contraception
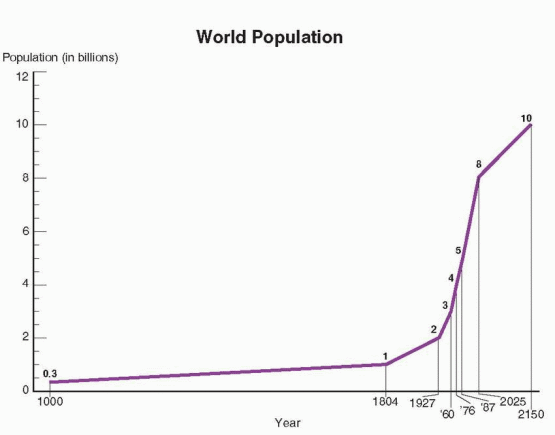
The world population is expected to stabilize at above 10 billion after 2180, with a fertility rate of 2.1 children per woman.34 Approximately 96% of the population growth now occurs in developing countries, so that by 2050, 10% of the population will live in developed countries, a decrease from the current 25%. Today, the fertility rate is about 1.6 children per women in China, Eastern and Western Europe, North America, Japan, Australia, and New Zealand.34 Some time after 2020, all of the growth in global population will occur in developing countries.
WORLD POPULATION
billion — achieved in 1804
billion — achieved in 1927
billion — achieved in 1960
billion — achieved in 1974
billion — achieved in 1987
billion — achieved in 1999
billion — in 2025
billion — in 2050
Throughout the world, 45% of married women of reproductive age practice contraception. However, there is significant variation from area to area; e.g., more than 70% in the U.S. and China but only 6% in Nigeria.35 About 71 million married women living in developing countries are at risk of an unplanned pregnancy.36 Less than 15% of women of reproductive age in the world are using oral contraceptives, and more than half live in the U.S., Brazil, France, and Germany.
The 76% of the world’s population living in developing countries account for:
85% of all births,
95% of all infant and childhood deaths,
99% of all maternal deaths.
The problem in the developing world is self-evident. The ability to regulate fertility has a significant impact on infant, child, and maternal mortality and morbidity. A pregnant woman has a 200 times greater chance of dying if she lives in a developing country rather than in a developed country.37 The health risks associated with pregnancy and childbirth in the developing world are far, far greater than risks secondary to the use of modern contraception.38 To meet the projected growth in the world’s population, the number of women using family planning will need to increase substantially from 1998 to 2025; for example, 40 million more women in India will need to use some method of contraception!35 In the developing world, about 140 million women who don’t want to get pregnant are not using contraception.
In recent years, there has been an appropriate shift from a narrow focus on contraception to a broader view that encompasses the impact of poverty, emphasizes overall well-being and the rights of individuals, endorses gender equality, and examines the interactions among these issues.39 It is not enough to simply limit fertility; contraception is only one component of reproductive health.
The Impact of Use and Nonuse
Inadequate access to contraception is associated with a high induced abortion rate. Effective contraceptive use largely, although not totally, replaces the resort to abortion. The combination of restrictive abortion laws and the lack of safe abortion services continues to make unsafe abortion a major cause of morbidity and mortality throughout the world, especially in many developing countries where abortion services are illegal.40 Both safe and unsafe abortions can be minimized by maximizing contraceptive services. However, the need for safe abortion services will persist because contraceptive failures account for about half of the 1.2 million annual induced abortions in the U.S.41
In the U.S., money spent on public funding for family planning saves money spent on medical, welfare, and nutritional services.42 States with higher family planning expenditures have fewer induced abortions, low-birth weight newborns, and premature births.43 The investment in family planning leads to short-term reductions in expenditures on maternal and child health services and, after 5 years, a reduction in costs for education budgets. Cutting back on publicly funded family planning services largely affects poor women, increasing the number of unintended births and abortions.
Sexually Transmitted Infections and Contraception
The interaction between clinician and patient for the purpose of contraception provides an opportunity to control sexually transmitted infections (STIs). The modification of unsafe sexual practices reduces the risk of unplanned pregnancy and the risk of infections of the reproductive tract. A patient visit for contraception is an excellent time for STI screening; if an infection is symptomatic, it should be diagnosed and treated during the same visit in which contraception is requested. A positive history for STIs should trigger both screening for asymptomatic infections and counseling for safer sexual practices. Attention should be given to the contraceptive methods that have the greatest influence on the risk of STIs.
Global Warming and Contraception
In the midst of politics and philosophy heavily promoting a “green” effort to limit global warming, a very important point is being ignored. Even small increases in population have a major impact on the global environment, including excessive consumption of resources in affluent societies.
Thomas Robert Malthus, an English clergyman, mathematician, and political economist, published six editions of his famous book, An Essay on the Principle of Population, between the years 1798 and 1826. The Malthusian Hypothesis can be expressed very simply: the human population will outgrow the world’s resources needed for its support. Malthus argued that population could be controlled only by a high death rate or a low birth rate. But because he didn’t approve of birth control, he concluded that a high death rate would be necessary, caused by misery, in the form of wars, famine, and disease, and vice (contraception was in this category, along with murder). Without misery and vice, overpopulation, therefore, would lead to poverty, an animalistic competition for food, and a general loss of civilization.
The Malthusian Hypothesis has been resurrected in recent times. There is a growing awareness that our planet is running out of clean air, potable water, and specific agricultural and mineral commodities. Optimists look to the power of technology and human creativity to solve this Malthusian problem, but the acute need for effective contraception cannot be ignored, as it is by most economists. Effective family planning programs not only benefit individuals, but also national economies and the global environment. The need and demand for family planning are extant in every part of our world, although greatest in the developing countries. Lacking is the required political and financial commitment. An appreciation for the impact on global warming can provide added motivation.
Contraception and Litigation
Clinicians are concerned about the prospect of bad outcomes associated with contraceptive use leading to litigation. Multimillion dollar verdicts and settlements in favor of plaintiffs who have used products as innocent as spermicides capture national attention. Actually, these events are very unusual compared with the widespread use of contraception.
The best way to avoid litigation is good patient communication. Patients who sue usually claim there were contraindications or risks that were not conveyed by the clinician. The best way to influence litigation is to keep good records. Good clinician’s records are the most formidable weapon for the defense. Documentation is vital, but it is useless without thorough history taking. Good records and good history taking put the responsibility on the patient’s honesty in response to the clinician.
Document that the risks and benefits of all methods were discussed.
Document a plan for follow-up.
Document all interactions with the patient, including phone calls.
The Future
From 1970 to 1986, the number of births in women older than 30 quadrupled; from 1990 to 2005, the fertility rate among women older than 30 remained relatively stable, but in 2005 and 2006, the birth rates for women over 30 and for women over 40 increased.9,44,45 As couples deferred pregnancy until later in life, the use of sterilization under age 35 declined, and the need for reversible contraception increased.
Until 2005, the highest number of births in the U.S. occurred between 1947 and 1965— the post-World War II baby boom (a demographic phenomenon shared by all parts of the developed world). The entire cohort of women born in this period will have reached their 45th birthday around 2010. We have experienced, therefore, an unprecedented number of women in the later childbearing years. This group of women not only increased in number but changed its fertility pattern.
The deferment of marriage is a significant change in our society. However, only a small percentage of the decline in the total fertility rate is accounted for by the increase in the average age at first marriage. Most of the decline in total fertility rate is accounted for by changes in marital fertility rates. In other words, postponement of pregnancy in marriage is the more significant change. This combination of increasing numbers, deferment of marriage, and postponement of pregnancy in marriage is responsible for the fact that we are seeing more and more older women who need reversible contraception. In short, there will continue to be longer duration of contraceptive use in younger women and greater use in older women, a pattern that began in 1990.
Fortunately, clinicians and patients recognized that low-dose steroid contraception is very safe for healthy, nonsmoking, older women. Between 1988 and 1995, the use of oral contaceptives doubled among women aged 35-39, and increased 6-fold in women older than age 40.26 However, as the previously mentioned statistics indicate, its use is still not sufficient to meet the need. In addition to fulfilling a need, this population of women has a series of benefits to be derived from steroid contraception that tilt the risk/benefit ratio to the positive side (Chapter 22).
The growing need for reversible contraception would also be served by increased use of the IUD. The decline in IUD use in the U.S. was in direct contrast to the experience in the rest of the world, a complicated response to publicity and litigation. An increased risk of pelvic infection with contemporary IUDs in use is limited to the act of insertion and the transportation of pathogens to the upper genital tract. This risk is effectively minimized by careful screening with preinsertion cultures and the use of good technique. A return to IUD use by American couples is both warranted and desirable.
A major problem in the U.S. is the prevalence of misconceptions. More than half of women, even well-educated women, are not accurately aware of the efficacy or the benefits and side effects associated with contraception.47,48 and 49 Unfortunately, a significant percentage of women still do not know that there are many health benefits with the use of steroid contraception. Misconceptions regarding contraception have, in many instances, achieved the stature of myths. Myths are an obstacle to good utilization and can only be dispelled by accurate and effective educational efforts.
Contraceptive advice is a component of good preventive health care. The clinician’s approach is a key. This is an era of informed choice by the patient. Patients deserve to know the facts and need help in dealing with the state of the art and the uncertainty. But there is no doubt that patients, especially young patients, are influenced in their choice by their clinicians’ advice and attitude. Although the role of a clinician is to provide the education necessary for the patient to make proper choices, one should not lose sight of the powerful influence exerted by the clinician in the choices ultimately made. In the 1970s, we approached the patient with great emphasis on risk. In the 1990s, studies effectively documented the risks and benefits of contraception. In the new century, the approach should be different, highlighting the benefits and the greater safety of appropriate contraception. If one attempts to sum the impact of the benefits of contraception on public health, as some have done with models focusing on hospital admissions, there is no doubt that the benefits outweigh the risks. The impact can be measured in terms of both morbidity and mortality. However, the impact on public health is of little concern during the clinician-patient interchange in the medical office. Here personal risk is paramount, and compliance with effective contraception requires accurate information presented in a positive, effective fashion.
Sterilization
Contraceptive methods today are very safe and effective; however, we remain decades away from a perfect method of contraception for either women or men. Because reversible contraceptive methods are not perfect, more than a third of American couples use sterilization instead, and sterilization is now the predominant method of contraception in the world.
Over the past 20 years, over 1 million Americans each year have undergone a sterilization operation, and recently, more women than men. Currently 39% of reproductive-aged American women rely on contraceptive sterilization: 27% undergo tubal occlusion (11 million women), and 11% depend on their partners’ vasectomies (4 million men).26 This same trend has occurred in Great Britain, where by age 40, more than 20% of men and women have had a sterilization procedure.50 In Spain and Italy, sterilization rates are very low, but the use of oral contraceptives and the IUD is very high.51
History
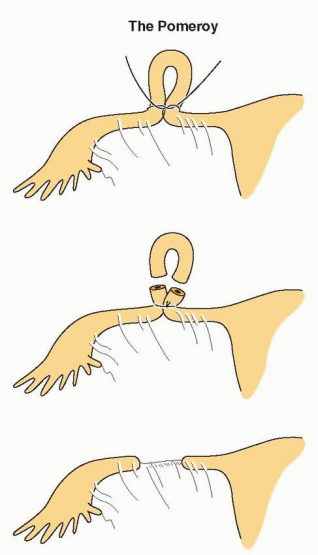
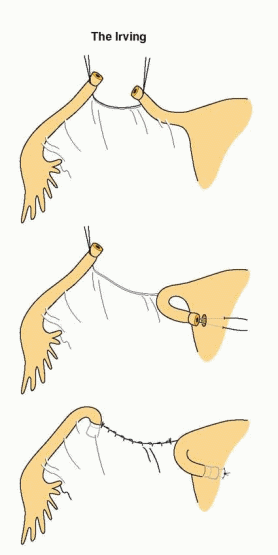
James Blundell proposed in 1823, in lectures at Guy’s Hospital in London, that tubectomy ought to be performed at cesarean section to avoid the need for repeat sections.52 He also proposed a technique for sterilization, which he later described so precisely that he must actually have performed the operation, although he never wrote about it. The first report was published in 1881 by Samuel Lungren of Toledo, Ohio, who ligated the tubes at the time of cesarean section, as Blundell had suggested 58 years earlier.53 The Madlener procedure was devised in Germany in 1910 and reported in 1919. Because of many failures, the Madlener technique was supplanted in the U.S. by the method of Ralph Pomeroy, a prominent physician in Brooklyn, New York. This method, still popular today, was not described to the medical profession by Pomeroy’s associates until 1929, 4 years after Pomeroy’s death. Frederick Irving of the Harvard Medical School described his technique in 1924, and the Uchida method was not reported until 1946.
Few sterilizations were performed until the 1930s when “family planning” was first suggested as an indication for surgical sterilization by Baird in Aberdeen. He required women to be older than 40 and to have had eight or more children. Mathematical formulas of this kind persisted through the 1960s. In 1965, Sir Dugald Baird delivered a remarkable lecture, entitled “The Fifth Freedom,” calling attention to the need to alleviate the fear of unwanted pregnancies and the important role of sterilization.54 By the end of the 1960s, sterilization was a popular procedure.
Laparoscopic methods were introduced in the early 1970s. The annual number of vasectomies began to decline, and the number of tubal occlusion operations increased rapidly. By 1973, more sterilization operations were performed for women than for men. This is accurately attributed to dramatic decreases in costs, hospital time, and pain because of the introduction of laparoscopy and minilaparotomy methods. The use of laparoscopy for tubal occlusion increased from only 0.6% of sterilizations in 1970 to more than 35% by 1975.55 Since 1975, minilaparotomy, a technique popular in the less developed world, has been increasingly performed in the U.S. These methods have allowed women to undergo sterilization operations at times other than immediately after childbirth or during major surgery.
Laparoscopy and minilaparotomy have led to a profound change in the convenience and cost of sterilization operations for women. In 1970, the average woman stayed in the hospital 6.5 days for a tubal sterilization. By 1975, this had declined to 3 days, and today, women rarely remain in the hospital overnight. The shorter length of stay achieved from 1970 to 1975 represented a savings of more than $200 million yearly in health care costs and a tremendous increase in convenience for women eager to return to work and their families.56 Unlike some advances in technology, laparoscopy and minilaparotomy sterilization are technical innovations that have resulted in large savings in medical care costs.
The great majority of sterilization procedures are accomplished in hospitals by physicians in private practice, but a rapidly increasing proportion is performed outside of hospitals in ambulatory surgical settings, including physicians’ offices. In either hospital or outpatient settings, female sterilization is a very safe operation. Deaths specifically attributed to sterilization now account for a fatality rate of only 1.5 per 100,000 procedures, a mortality rate that is lower than that for childbearing (about 8 per 100,000 births in the U.S.).57,58 When the risk of pregnancy from contraceptive method failure is taken into account, sterilization is the safest of all contraceptive methods.
Vasectomy has long been more popular in the U.S. than anywhere else in the world, but why don’t more men use it? One explanation is that women have chosen laparoscopic sterilization in increasing numbers. Another is that men have been frightened by reports, often from animal data, of associations with autoimmune diseases, atherosclerosis, and, most recently, prostatic cancer. Large epidemiologic studies have failed to confirm any definite adverse consequences.59 When patients consider sterilization, we can assure them that vasectomy has not been demonstrated to have any harmful effects on men’s health.60 In addition, vasectomy is less expensive than tubal sterilization, morbidity is less, and mortality is essentially zero.
Efficacy of Sterilization
Laparoscopic and minilaparotomy sterilizations are not only convenient, they are almost as effective at preventing pregnancy as were the older, more complex operations. Vasectomy is also highly effective once the supply of remaining sperm in the vas deferens is exhausted. Approximately 50% of men will reach azoospermia at 8 weeks, but the time to achieve azoospermia is highly variable, reaching only about 60% to 80% after 12 weeks.61,62
Failure Rates During the First Year of Use, United States17,18,20
Percent of women with pregnancy
Method
Lowest Expected (%)
Typical (%)
Female sterilization
0.5
0.7
Male sterilization
0.1
0.2
In addition to the specific operation used, the skill of the operator and characteristics of the patient make important contributions to the efficacy of female sterilization. Up to 50% of failures are due to technical errors. The methods using complicated equipment, such as spring-loaded clips and silastic rings, fail for technical reasons more commonly than do simpler procedures such as the Pomeroy tubal ligation.63 Minilaparotomy failures, therefore, occur much less frequently from technical errors.
It is hardly surprising that more complicated techniques of tubal occlusion have higher technical failure rates. What is surprising is the finding that characteristics of the patient influence the likelihood of failure even when technical problems are controlled for in analytical adjustments. In a careful study of this issue, two patient characteristics, age and lactation, demonstrated a significant impact.64 Patients younger than 35 years were 1.7 times more likely to become pregnant, and women who were not breastfeeding following sterilization were 5 times more likely to become pregnant. These findings probably reflect the greater fecundity of younger women and the contraceptive contribution of lactation.
Significant numbers of pregnancies after tubal occlusion are present before the procedure. For this reason, some clinicians routinely perform a uterine evacuation or curettage prior to tubal occlusion. It seems more reasonable (and cost-effective) to exclude pregnancy by careful history taking, physical examination, and an appropriate pregnancy test prior to the sterilization procedure.65
Because method, operator, and patient characteristics all influence sterilization failures, it is difficult to predict which individual will experience a pregnancy after undergoing a tubal occlusion. Therefore, during the course of counseling, all patients should be made aware of the possibility of failure as well as the intent to cause permanent, irreversible sterility. It is important to avoid giving patients the impression that the tubal occlusion procedure is foolproof or guaranteed. Individual clinicians must be cautious judging their own success in accomplishing sterilization because failure is infrequent and many patients who become pregnant after sterilization never reveal the failure to the original surgeon.
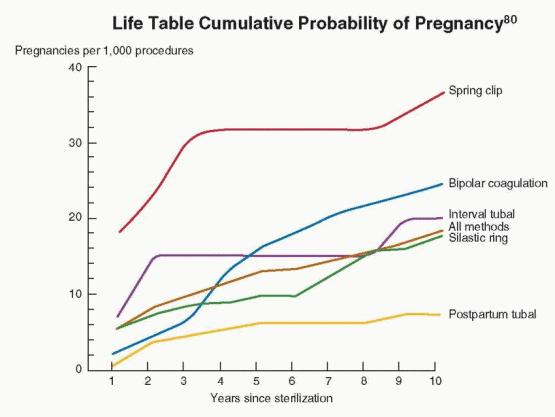
Ectopic pregnancies can occur following tubal occlusion, and the incidence is much higher with some types of tubal occlusion.66,67 and 68 Bipolar tubal coagulation is more likely to result in ectopic pregnancy than is mechanical occlusion.63,69,70 The probable explanation is that microscopic fistulae in the coagulated segment connecting to the peritoneal cavity permit sperm to reach the ovum. Ectopic pregnancies following tubal ligation are more likely to occur 3 or more years after sterilization, rather than immediately after. The proportion of ectopic pregnancies is 3 times as high in the fourth through the tenth years after sterilization as in the first 3 years.70 For laparoscopic methods, the cumulative rate of ectopic pregnancy continues to increase for at least 10 years after surgery, reaching 17 per 1,000 for bipolar coagulation.70 Overall, however, the risk of an ectopic pregnancy in sterilized women is lower than if they had not been sterilized. Nevertheless, approximately one-third of the pregnancies that occur after tubal sterilization are ectopic.70
Vaginal procedures have higher failure rates than laparoscopy or minilaparotomy, but the principal disadvantage is a higher rate of infection. Intraperitoneal infection is a rare complication of minilaparotomy or laparoscopic techniques, but in vaginal procedures, abscess formation approaches 1%.71 This risk can be reduced by the use of prophylactic antibiotics administered intraoperatively, but open laparoscopy is usually easier and safer than vaginal sterilization even in obese women.
Sterilization and Ovarian Cancer—A Benefit of Sterilization
Serous ovarian cancer, the most common ovarian cancer, originates in the fimbriae of the fallopian tubes.72,73 and 74 Evidence consistently indicates that tubal sterilization is associated with a major reduction in the risk of ovarian cancer.75,76,77,78 and 79 Evidence from the Nurses’ Health Study indicated that tubal sterilization was associated with a 67% reduced risk of ovarian cancer.75 In the prospective mortality study conducted by the American Cancer Society, women who had undergone tubal sterilization experienced about a 30% reduction in the risk of fatal ovarian cancer.76
Female Sterilization Techniques
Because laparoscopy permits direct visualization and manipulation of the abdominal and pelvic organs with minimal abdominal disruption, it offers many advantages. Hospitalization is not required; most patients return home within a few hours, and the majority return to full activity within 24 h. Discomfort is minimal, the incision scars are barely visible, and sexual activity need not be restricted. In addition, the surgeon has an opportunity to inspect the pelvic and abdominal organs for abnormalities. The disadvantages of laparoscopic sterilization include the cost; the expensive, fragile equipment; the special training required; and the risks of inadvertent bowel or vessel injury.
Laparoscopic sterilization can be achieved with any of these methods:
Occlusion and partial resection by unipolar electrosurgery.
Occlusion and transection by unipolar electrosurgery.
Occlusion by bipolar electrocoagulation.
Occlusion by mechanical means (clips or silastic rings).
All of these methods can use an operating laparoscope alone, the diagnostic laparoscope with operating instruments passed through a second trocar, or both the operating laparoscope and secondary puncture equipment. All can be used with the “open” laparoscopic technique in which the laparoscopic instrument is placed into the abdominal cavity under direct vision to avoid the risk of bowel or blood vessel puncture on blind entry. Patient acceptance and recovery are approximately the same with all methods.
It is now apparent that the long-term failure rates for all methods are higher than previous estimates; overall, 1.85% of sterilized American women experience a failure within 10 years.80As much as one-third of these failures are ectopic pregnancies.70 The higher failure rates with silastic rings, the Hulka-Clemens clip, and bipolar coagulation reflect the greater degree of skill required for these methods. Because of the effect of declining fecundity with increasing age, younger sterilized women are more likely to have a failure, including ectopic pregnancy, compared with older women. For these reasons, younger women seeking sterilization should consider the use of the IUD or implants, reversible methods that offer very low failure rates.
If electrons from an electrosurgical generator are concentrated in one location, heat within the tissue increases sharply and desiccates the tissue until resistance is so high that no more current can pass. Unipolar methods of sterilization create a dense area of current under the grasping forceps of the unipolar electrode. To complete the circuit, however, these electrons must spread through the body and be returned to the generator via a return electrode (the ground plate) that has a broad surface to minimize the density of the current to avoid burns as the electrons leave the body. “Unipolar” refers to the method that requires the patient ground plate.
Unipolar electrosurgery can create a unique electrical “capacitance” problem. A capacitor is any device that can hold an electric charge and can exist wherever an insulated material separates two conductors that have different potentials. This property of capacitance explains some of the inadvertent bowel burns that occurred with laparoscopic sterilization.82 The operating laparoscope is a hollow metal tube surrounding an active electrode, the forceps used to grasp and coagulate the tubes. When current passes through the active electrode, the laparoscope itself becomes a capacitor. Up to 70% of the current passed through the active electrode can be induced into the laparoscope. If bowel or other structures touch a laparoscope, which is insulated from the abdominal incision (e.g., by a plastic cannula), the stored electrons will be discharged at high density directly into the vital organ. This potential hazard is eliminated by using a metal trocar sleeve rather than a nonconductive sleeve. Because there is little pressure behind the electrons from a low-voltage generator, not enough heat is generated to burn the skin as the capacitance current leaks out into the patient’s body through the metal sleeve. Even if the active electrode comes in direct contact with the laparoscope, as when a two-incision technique is used, the current will leak harmlessly through the metal trocar sleeve. The risk of inadvertent coagulation of bowel or other organs cannot be completely eliminated because all body surfaces offer a path back to the ground plate.
The unipolar electrosurgical technique is straightforward. The isthmic portion of the fallopian tube is grasped and elevated away from the surrounding structures, and the electrical energy is applied until the tissue blanches, swells, and then collapses. The tube is then grasped, moving toward the uterus, recoagulated, and the steps repeated until 2-3 cm of tube have been coagulated. Some surgeons advise against cornual coagulation for fear it may increase the risk of ectopic pregnancy due to fistula formation.
The coagulation and transection technique is performed in a similar fashion with the same instruments. In order to transect the tube, however, an instrument designed to cut tissue must be used. The transection of tissue increases the risk of possible bleeding and does not, by itself, reduce the failure rate over coagulation alone. The specimens obtained by this method are usually coagulated beyond microscopic recognition and, therefore, will not provide pathologic evidence of successful sterilization.
The bipolar method of sterilization eliminates the ground plate required for unipolar electrosurgery and uses a specially designed forceps. One jaw of the forceps is the active electrode, and the other jaw is the ground electrode. Current density is great at the point of forceps contact with tissue, and the use of a low-voltage, high-frequency current prevents the spread of electrons. By eliminating the return electrode, the chance of an aberrant pathway through bowel or other structures is greatly reduced. There is, however, a disadvantage with this technique. Because electron spread is decreased, more applications of the grasping forceps are necessary to coagulate the same length of tube than with unipolar coagulation. As desiccation occurs at the point of high current density, tissue resistance increases, and the coagulated area eventually provides resistance to flow of the low-voltage current. Should the resistance increase beyond the voltage’s capability to push electrons through the tissue, incomplete coagulation of the endosalpinx can result.83Bipolar coagulation is very effective only if three or more sites are coagulated on each tube.84
Bipolar cautery is safer than unipolar cautery with regard to burns of abdominal organs, but most studies indicate higher failure rates. Although the bipolar forceps will not burn tissues that are not actually grasped, care must be taken to avoid coagulating structures adherent to the tubes. For example, the ureter can be damaged when the tube is adherent to the pelvic side wall.
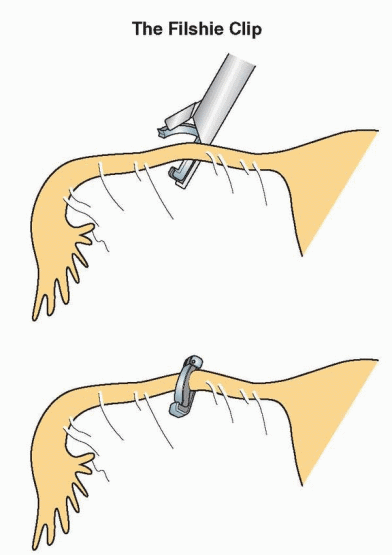
Tubal Occlusion with Clips and Rings
Female sterilization by mechanical occlusion eliminates the safety concerns with electrosurgery. However, mechanical devices are subject to flaws in material, defects in manufacturing, and errors in design, all of which can alter efficacy. Three mechanical devices have been widely used and have low failure rates with long-term follow-up: the Hulka-Clemens (spring) clip, the Filshie Clip, and the silastic (Falope or Yoon) ring. Each of the three requires an understanding of its mechanical function, a working knowledge of the intricate applicator necessary to apply the device, meticulous attention to maintenance of the applicators, and skillful tubal placement. These devices are less effective when used immediately postpartum on dilated tubes.
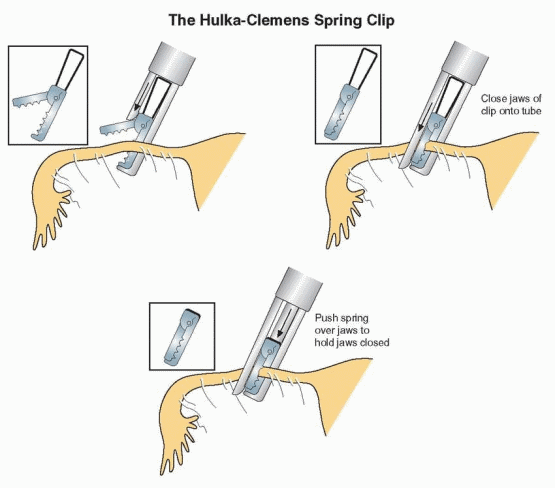
Hulka-Clemens Spring Clip
The spring clip consists of two plastic jaws made of Lexan, hinged by a small metal pin 2 mm from one end. Each jaw has teeth on the opposed surface, and a stainless steel spring is pushed over the jaws to hold them closed over the tube. A special laparoscope for one-incision application is most commonly used, although the spring clip can also be used in a two-incision procedure. The spring clip is applied at a 90-degree angle to include some mesosalpinx at the proximal isthmus of a stretched fallopian tube. The spring clip destroys 3 mm of tube and has 1-year pregnancy rates of 2 per 1,000 women but the highest 10-year cumulative failure rate.63,80
Complications unique to spring clip sterilization result from mechanical difficulties. If the clip is dislodged or dropped into the abdomen during the procedure, it should be retrieved. Usually, it can be removed laparoscopically, but sometimes laparotomy is necessary. Should incomplete occlusion or incorrect alignment of the clip occur, a second clip can be applied without hazard. This clip offers a good chance for reanastomosis, better than electrosurgical methods that destroy more tube.
Filshie Clip
The Filshie clip is made of titanium lined with silicone rubber. The hinged clip is locked over the tube using a special applicator through a second incision or operating laparoscope. The rubber lining of the clip expands on compression to keep the tube blocked. Only 4 mm of the tube are destroyed. Failure rates 1 year after the procedure approximate 1 per 1,000 women.68 A 15-year follow-up study in Quebec reported a cumulative failure rate of 9 per 1,000 women, whereas the 10-year failure rate in the U.K. was 5.6 per 1,000 woman.81,85 Because the Filshie clip is longer, it is reported to occlude dilated tubes more readily than does the spring clip. Both the spring clip and the Filshie clip provide good chances for tubal reanastomosis.
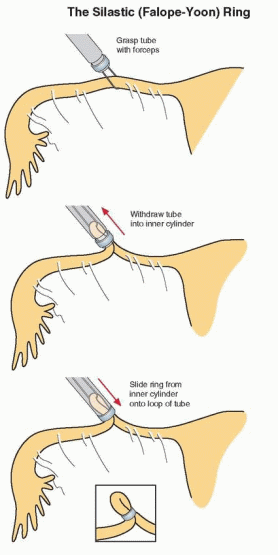
Silastic (Falope or Yoon) Ring
This nonreactive silastic rubber band has an elastic memory of 100% if stretched to no more than 6 mm for a brief time (a few minutes at most). A special applicator, 6 mm in diameter, can be placed through a second cannula or through a standard offset operating laparoscope. The applicator is designed to grasp a knuckle of tube and release the silastic band onto a 2.5 cm loop of tube. The avascular loop of tube can be resected with biopsy forceps to provide a pathology specimen, but this is rarely performed (it does not increase efficacy). Ten percent to 15% of patients experience severe postoperative pelvic cramping from the tight bands (which can be alleviated by the application of a local anesthetic to the tube before or after banding).
As with application of clips, the ring should be placed at the junction of the proximal and middle third of each fallopian tube. Necrosis occurs promptly and a 2-3 cm segment of the tube is destroyed. Failure rates are about 1% after 2 years, and the 10-year cumulative rate is better only with unipolar coagulation, postpartum tubal excision, and the Filshie clip.80
Mesosalpingeal bleeding is the most common complication of silastic ring application. It usually occurs when the forceps grabs not only the tube but also a vascular fold of mesosalpinx. The mesosalpinx can also be torn on the edge of the stainless steel cylinder as the tube is drawn into the applicator. If bleeding is noted, application of the silastic band often controls it. If the placement of additional bands or electrocoagulation fails to stop bleeding, laparotomy may be required.
Silastic rings are occasionally placed on structures other than the tube. If this mistake is recognized, the band can usually be removed from the round ligament or mesosalpingeal folds by grasping the band with the tongs of the applicator and applying gradual, increasing traction. If a gentle attempt fails, removal is not necessary. If rings are inadvertently discharged into the peritoneal cavity, they can safely be left behind.
Patients should be prepared for the use of electrosurgical instruments in case bands or clips cannot be applied (because of adhesions or bleeding).
Minilaparotomy
Tubal ligation, accomplished through a small suprapubic incision, minilaparotomy, is the most frequent method of interval female sterilization around the world. In the U.S. and most of the developed world, laparoscopy is more popular, but minilaparotomy is gaining in favor because of its safety, simplicity, and adaptability to ambulatory surgical settings (particularly when local anesthesia is used).86,87
The fallopian tubes can be occluded through the minilaparotomy incision with bands or clips, but a simple Pomeroy tubal ligation is the method most commonly used. Patient characteristics, such as obesity, previous pelvic infection, or previous surgery, are the principal determinants of complications.88
Minilaparotomy is accomplished through an incision that usually measures 2-4 cm in length. Tubal ligation through a suprapubic incision can be accomplished for obese patients, but the incision will necessarily exceed the usual length. Forceful retraction increases the pain associated with the procedure and the time of recovery. For these reasons, we believe that minilaparotomy for ambulatory tubal occlusion should be limited to patients who are not obese (usually less than 150-160 lb, 70 kg).
Tubal occlusion is difficult to accomplish through a minilaparotomy if the uterus is immobile. Laparoscopic tubal occlusion, on the other hand, does not require extreme uterine elevation or rotation and is a better choice for a patient with a uterus fixed in position.
Only gold members can continue reading. Log In or Register to continue