Background
Health disparities begin early in life and persist across the life course. Despite current efforts, black women exhibit greater risk for pregnancy complications and negative perinatal outcomes compared with white women. The placenta, which is a complex multi-tissue organ, serves as the primary transducer of bidirectional information between the mother and fetus. Altered placental function is linked to multiple racially disparate pregnancy complications; however, little is known about racial differences in molecular factors within the placenta. Several pregnancy complications, which include preeclampsia and fetal growth restriction, exhibit racial disparities and are associated with shorter placental telomere length, which is an indicator of cellular stress and aging. Cellular senescence and telomere dynamics are linked to the molecular mechanisms that are associated with the onset of labor and parturition. Further, racial differences in telomere length are found in a range of different peripheral tissues. Together these factors suggest that exploration of racial differences in telomere length of the placenta may provide novel mechanistic insight into racial disparities in birth outcomes.
Objective
This study examined whether telomere length measured in 4 distinct fetally derived tissues were significantly different between black and white women. The study had 2 hypotheses: (1) that telomere length that is measured in different placental tissue types would be correlated and (2) that across all sampled tissues telomere length would differ by race.
Study Design
In a prospective study, placental tissue samples were collected from the amnion, chorion, villus, and umbilical cord from black and white singleton pregnancies (N=46). Telomere length was determined with the use of monochrome multiplex quantitative real-time polymerase chain reaction in each placental tissue. Demographic and pregnancy-related data were also collected. Descriptive statistics characterized the sample overall and among black and white women separately. The overall impact of race was assessed by multilevel mixed-effects linear regression models that included empirically relevant covariates.
Results
Telomere length was correlated significantly across all placental tissues. Pairwise analyses of placental tissue telomere length revealed significantly longer telomere length in the amnion compared with the chorion (t=–2.06; P =.043). Overall telomere length measured in placenta samples from black mothers were significantly shorter than those from white mothers (β=–0.09; P =.04). Controlling for relevant maternal and infant characteristics strengthened the significance of the observed racial differences (β=–0.12; P =.02). Within tissue analyses revealed that the greatest difference by race was found in chorionic telomere length (t=–2.81; P =.007).
Conclusion
These findings provide the first evidence of racial differences in placental telomere length. Telomere length was significantly shorter in placental samples from black mothers compared with white mothers. Given previous studies that have reported that telomere length, cellular senescence, and telomere dynamics are molecular factors that contribute to the rupture of the amniotic sac, onset of labor, and parturition, our findings of shorter telomere length in placentas from black mothers suggest that accelerated cellular aging across placental tissues may be relevant to the increased risk of preterm delivery in black pregnancies. Our results suggest that racial differences in cellular aging in the placenta contribute to the earliest roots of health disparities.
Health disparities are well documented, beginning early in life and persisting over the life course. Non-Hispanic black women have higher rates of preterm delivery, low birthweight infants, and infant mortality relative to non-Hispanic white women. In addition, racial differences in pregnancy complications that include preeclampsia, gestational diabetes mellitus (GDM), and fetal growth restriction (FGR) also exist, which likely contributes to other infant health disparities across the first year of life. Despite substantial efforts and heightened awareness, these disparities persist. Increased understanding of the underlying mechanisms and how they contribute to perinatal outcomes are needed.
The placenta is a critical organ at the interface between the fetus and mother because it coordinates maternal physiology and fetal development. The human placenta is comprised of maternally and fetally derived tissues with interdigitated vascular flow. The fetal portion includes 4 anatomically distinct tissues: amnion, chorion, villus, and umbilical cord, all of which exhibit unique gene expression profiles and different time points of differentiation during fetal development. The vascularized villus is the main site of oxygen and nutrient exchange; the umbilical cord enables fetoplacental circulation. The amnion and chorion protect the developing fetus and facilitate nutrient and hormone transfer between the mother and fetus. Pregnancy complications that exhibit racial disparities, which include preeclampsia, GDM, preterm birth, and premature rupture of membranes are all associated with altered placental physiologic condition, metabolism, and function. As such, exploration of racial differences in placental function may provide insight into the mechanisms underlying early health disparities.
One biologic marker that is associated with altered placental function and these pregnancy complications is telomere length (TL). Telomeres are nucleoprotein complexes that cap chromosomes in eukaryotic cells, that are essential for cell survival and chromosome stability, and that influence cellular differentiation, senescence, and apoptosis. Shortening of TL has been associated with cellular aging; TL is influenced by DNA repair mechanisms, oxidative stress, and inflammation. TL tends to be highly correlated across tissues at birth, but this correlation lessens as an individual ages. Shorter placental TL has been associated with racially disparate pregnancy complications such as FGR, GDM, and preeclampsia. Correlations among placental TL and gestational age, socioeconomic status, and parity have also been reported. To date no previous studies have addressed racial differences in placental TL. Previous studies of placental TL have used DNA that was extracted from an array of sites, with inconsistent attention to confounding maternal tissue, inclusion of multiple cell tissue types, or failure to define the specific sampling site altogether. Given the complexity of placenta, these methodologic variations curtail their generalizability and warrant further investigation.
Racial differences in TL have also been observed, for which black newborn infants and adolescents exhibit longer TL than white infants. Longer TL and associated greater TL attrition across the life course has been reported in black adults, although some debate exists. Longer initial TL is a predictor of increased TL attrition over time and, consistent with this, an aged cohort of black infants displayed shorter TLs than white infants. From an aging and health disparities perspective, the placenta represents a unique opportunity to examine racial differences in cellular aging, given its definitive lifespan and the molecular evidence pointing to a role of cellular aging and telomeres in parturition.
To better understand how placental factors may contribute to persistent racial disparities in perinatal outcomes, this study examined both the correlation of TL across fetally derived tissues and racial differences.
Materials and Methods
Subjects
Subjects were a subset of mothers (n=46) who were recruited January 2015 from a larger longitudinal study in New Orleans, LA, and who consented to placental collection. Recruitment of pregnant women, aged 18-41 years, took place in prenatal and Women, Infant, and Children clinics and from other ongoing studies that involved pregnant women at Tulane University. The women were at least 18 years of age, English-speaking, and pregnant with a singleton fetus. They provided information via a face-to-face interview-assisted computer survey (Questionnaire Development System; Nova Research, Bethesda, MD) that was conducted by trained interviewers. This study was approved by the Tulane University Institutional Review Board.
Demographic (eg, maternal and infant characteristics) and pregnancy-related data were collected by maternal report and medical record abstraction. Data that were collected by maternal report included maternal age at conception, race, and education level. Data collected from medical records included gestational age, infant birthweight, infant sex, delivery mode, parity, and pregnancy complications. Pregnancy complications included preeclampsia, FGR, GDM, gestational hypertension, and eclampsia/preeclampsia. Given the low prevalence of individual pregnancy complications in the sample, a composite categoric variable (yes/no) was created.
Placental tissue sample collection
Placenta collection and dissection occurred within approximately 1 hour of delivery. The reflected fetal membranes (eg, amnion and chorion) were separated manually, isolated, and excised >4 cm from the fusion to the placental disk. For fetal villus tissue sampling, the chorionic plate was removed, and approximately 2 cm of fetal villus tissue was excised within approximately 4 cm of the umbilical cord insertion site. Fetal villus samples were collected just below the chorionic plate to avoid sampling maternal villi, and visible vasculature was excised. Umbilical cord samples were collected within approximately 4 cm of the insertion site after removal of any fused membranes. Tissues were washed thoroughly in 1 mol/L phosphate-buffered saline solution to minimize contamination from blood or atrophied villi. Samples were flash frozen in liquid nitrogen and stored at –80°C. DNA was extracted from placental tissues with the use of QIAamp DNA mini kit protocol for tissues (Qiagen, Valencia, CA). Samples were evaluated for double-stranded DNA integrity and concentration by Qubit dsDNA BR assay kit (Invitrogen, Carlsbad, CA) and for purity by NanoDrop-2000 (Thermo Fisher Scientific, Waltham, MA). DNA was stored at –35°C.
Telomere length measurement
The average relative TL, as represented by the T/S ratio, was determined by monochrome multiplex quantitative real-time polymerase chain reaction and standard methods in our laboratory. All tissue samples from each individual placenta were run on the sample duplicate plates; all samples were run with the same control purchased genomic placental DNA from a single donor (BioChain Institute Inc, Newark, CA). Coefficient of variance (CV) for the whole sample was 2.12% for all plates. Samples (n=4) with unacceptably high CV were repeated.
Statistical analysis
Descriptive statistics characterized the sample overall and among black and white women with chi-square and t -tests. One black infant birthweight exceeded 3 standard deviations above the mean and was winsorized for analyses. The duration between delivery and sample collection was missing for 4 deliveries, and the mean duration by delivery type was imputed. Spearman correlation coefficients compared crude relationships between TL across the 4 placental tissue types. The normality of TL was examined with the use of visual inspection of plots, skewness, and kurtosis. TL was distributed normally.
Multilevel analysis with mixed-effects linear regression models was used to produce intraclass correlation coefficients (ICC) to estimate the degree of within individual correlation of TL across the 4 tissue types. First, we examined an empty model (regressing TL without covariates) to determine the degree of association among TLs within individuals and to allow for decomposition of the variation in TL into between- and within-individual variation (Model 1). Next, we added maternal race and a tissue type indicator variable in a model with randomly distributed individual-specific intercepts (Model 2). We tested for heterogeneity in the relationship between tissue type and TL among individuals by fitting this model with tissue type as a random effect in addition to the random intercept. Because of statistical power considerations, clustering TL at both the level of the individual and tissue type was not feasible. The study hypotheses explored differences between race at the level individual above tissue type and therefore clustered TL within an individual. Model 2 was used to test for an interaction between race and tissue type to determine whether the relationship between TLs across tissues differed between racial groups. Finally, we fit a model that included empirically relevant covariates with a fixed slope value for each predictor variable and random individual-specific intercepts (Model 3). We used this fully adjusted model to test for an interaction between race and tissue type to determine whether the relationship between TL across tissues differed between racial groups.
In a sensitivity analysis, we repeated the modeling after excluding the chorion (the tissue type with the largest racial difference in TL) to assess the degree to which the chorion drove the race effect. All analyses were conducted with the use of SAS software (version 9.4; SAS Institute, Inc, Cary, NC).
Results
Placental tissue TL was available from 46 pregnancies (black, 34; white,12). Mean age at conception was 27 years, and 63% of women attained at least some college education ( Table 1 ). Most deliveries were vaginal (56.5%), and all infants were born at term. Collection of placental tissue samples occurred on average 45 minutes after delivery.
| Variable | Total (N=46) | Black (n=34) | White (n=12) | P value |
|---|---|---|---|---|
| Descriptive outcome, mean±SD | ||||
| Maternal conception age, y | 26.94±6.73 | 26.50±6.94 | 28.17±6.19 | .467 |
| Gestational age, wk | 38.94±1.14 | 38.76±1.23 | 39.42±0.67 | .029 |
| Infant birthweight, kg | 3.28±0.56 | 3.21±0.54 | 3.49±0.58 | .140 |
| Duration to sample collection, min | 44.52±29.56 | 44.78±29.24 | 43.77±31.76 | .920 |
| Parity | 1.11±1.35 | 1.21±1.50 | 0.83±0.84 | .293 |
| Infant sex, % (n) | .883 | |||
| Male | 56.5 (26) | 55.9 (19) | 58.3 (7) | |
| Female | 43.5 (20) | 44.1 (15) | 41.7 (5) | |
| Delivery mode, % (n) | .410 | |||
| Vaginal | 56.5 (26) | 52.9 (18) | 66.7 (8) | |
| Cesarean section | 43.5 (20) | 47.1 (16) | 33.3 (4) | |
| Maternal education level, % (n) | .001 | |||
| <High school | 37.0 (17) | 44.1 (15) | 16.7 (2) | |
| <Some college | 32.6 (15) | 41.2 (14) | 8.3 (1) | |
| ≥College degree | 30.4 (14) | 14.7 (5) | 75.0 (9) | |
| Pregnancy complications, % (n) | .300 | |||
| No | 73.9 (34) | 67.7 (23) | 83.3 (10) | |
| Yes | 26.1 (12) | 32.4 (11) | 16.7 (2) |
There were no racial differences in maternal age at conception, delivery mode, duration between delivery and sample collection, infant birthweight, composite maternal pregnancy complications, parity, or infant sex ( Table 1 ). A greater proportion of white women attained a college degree or higher ( P =.001); infants born to black women had earlier gestational age ( P =.029).
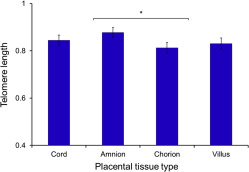
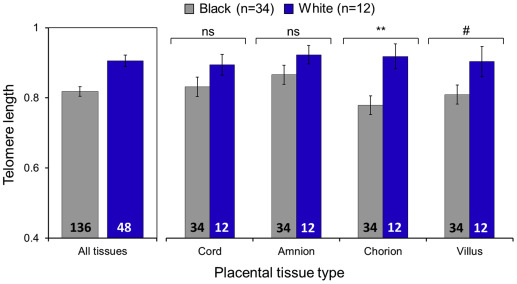
The rank order of placental tissue TLs from longest to shortest was amnion, which exhibited the longest TL with a mean of 0.877±0.15 T/S (black = 0.862±0.16 T/S; white = 0.919±0.09 T/S), cord with a mean of 0.845±0.15 T/S (black = 0.829±0.16 T/S; white = 0.891±0.10 T/S), and villus with a mean of 0.831±0.16 T/S (black = 0.806±0.16 T/S; white = 0.900±0.15 T/S); the shortest was the chorion with a mean of 0.812±0.16 T/S (black = 0.776±0.15 T/S; white = 0.912±0.12 T/S). Chorionic TL was significantly shorter than TL from the amnion (t=–2.06; P =.043); no other pairwise comparisons between tissues were significant ( Figure 1 ). Crude racial differences were observed in chorionic TL (t=–2.81; P =.007); villus TL approached significance (t=–1.80; P =.079), where placentas from black pregnancies exhibited shorter TL relative to white pregnancies ( Figure 2 ).
TL was correlated positively across placental tissues ( Table 2 ). Correlation coefficients between placental tissue types ranged from 0.67–0.53. A high degree of correlation across placental tissue types from within the same individual was evident in the mixed effects empty model (Model 1; ICC, 60.6%), which indicated that most of the variance was accounted for by differences between individuals ( Table 3 ).
| Outcome | Telomere length | Duration to sample collection, min | Gestational age, wk | |||
|---|---|---|---|---|---|---|
| Cord | Amnion | Chorion | Villus | |||
| Telomere length | ||||||
| Cord | 1 | |||||
| Amnion | 0.640 a | 1 | ||||
| Chorion | 0.543 | 0.613 a | 1 | |||
| Villus | 0.665 | 0.526 b | 0.540 b | 1 | ||
| Duration to sample collection, min | 0.343 c | 0.233 | 0.190 | 0.094 | 1 | |
| Gestational age, wk | –0.016 | –0.017 | –0.011 | –0.018 | –0.108 | 1 |
| Maternal conception age, y | –0.011 | –0.018 | 0.067 | 0.112 | 0.138 | –0.165 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


