2Princess Anne Hospital, Southampton, UK
Overview
- Approximately 40% of all breast cancers occur in women over the age of 70 years
- Older patients should be treated to the same standard as younger patients
- As most elderly patients’ cancers are oestrogen receptor positive, endocrine therapy can be used either to shrink the cancer prior to surgery or as adjuvant therapy after surgery
- Paget’s disease of the nipple is uncommon, but is often diagnosed late and needs to be considered in patients with nipple ulceration
- There is no evidence that pregnancy after treatment for breast cancer has an influence on patient survival
- Male breast cancer is rare and is not treated significantly different to female breast cancer
Approximately 40% of all breast cancers occur in women aged over 70 (Figure 10.1); this percentage will increase over the next decade. Overall, breast cancers that develop in older women are biologically less aggressive compared with those seen in younger patients, although survival rates for older women have been poorer in this age group, mainly because of undertreatment. The average life expectancy of a 70-year-old woman is in excess of 15 years and is over 9 years for a woman aged 80. Elderly women with breast cancer should be treated in a similar way to younger patients. Few patients are truly unfit for surgery because wide local excision or even mastectomy can, if necessary, be performed under local anaesthesia with sedation, although with modern anaesthetic techniques this is not required very often. There is no evidence to suggest that elderly patients tolerate radiotherapy less well than younger patients and when radiotherapy is given it should be in a radical dose.

Operable Tumours Suitable for Breast Conservation
Options for small operable breast cancers ≤ 4 cm are breast-conservation surgery (wide local excision and radiotherapy) or mastectomy with or without radiotherapy, combined with sentinel node biopsy or axillary clearance as appropriate (Table 10.1). Many older women are unhappy about losing a breast and choose breast conservation. Morbidity is much less after this procedure. Although the detection rate of sentinel nodes using blue dye and isotope has been reported to decrease with age, this technique is of particular value in older women to limit extensive axillary dissection to those who need it.
Table 10.1 Management of elderly patients with breast cancer.
| Tumour stage and size | Treatment options |
| T1 or T2 ≤ 4 cm, N0−1, M0 | Wide local excision, axillary surgery and radiotherapy or mastectomy, if contraindications to breast conservation or patient choice |
| T2>4 cm or T3, N0−1, M0 | |
| Oestrogen receptor positive | Mastectomy, or neoadjuvant letrozole and then if tumour regresses wide local excision, axillary surgery and radiotherapy |
| Oestrogen receptor negative or no response to letrozole | Mastectomy, and adjuvant tamoxifen |
| T4 or N2, M0 | |
| Oestrogen receptor positive | Letrozole%* |
| Oestrogen receptor negative or no response to letrozole | Radical radiotherapy or in selected patients and in those responding to letrozole, mastectomy and radiotherapy; neoadjuvant chemotherapy also an option |
| Any T, any N, M1 | |
| Oestrogen receptor positive | Letrozole and symptomatic treatment |
| Oestrogen receptor negative | Symptomatic treatment and consider chemotherapy |
| Very elderly or infirm patients | Letrozole if oestrogen receptor positive. Palliation if oestrogen receptor negative |
*Anastrozole and exemestane are alternatives to letrozole and should be followed by surgery and/or radiotherapy depending on response.
Operable Tumours Suitable for Mastectomy
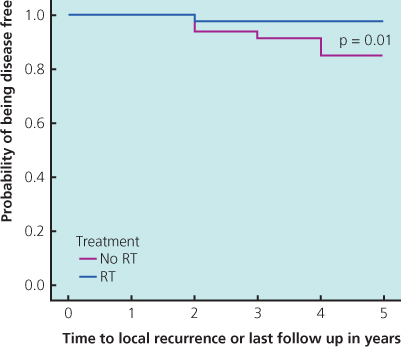
For larger tumours that are operable, options include mastectomy combined with sentinel node biopsy or axillary node clearance as appropriate or, if the tumour is ER rich on core biopsy (Figures 10.2 and 10.3), neoadjuvant endocrine therapy with an initial three-month course of an aromatase inhibitor is an option. Randomised studies have demonstrated that aromatase inhibitors are superior to tamoxifen in this setting (Figure 10.4). There are data using letrozole, anastrozole and exemestane. The data are most impressive for letrozole. This is the only aromatase inhibitor that has a product licence for use in the neoadjuvant setting. During treatment the tumour should be monitored clinically and by imaging (Figure 10.5): two-thirds of appropriately selected women will get a significant response to an aromatase inhibitor and over half of patients with ER-rich cancers become eligible for breast-conserving treatment within three months. Response is higher in patients with higher ER levels. Prolongation of therapy improves response rates and the optimal duration is probably between 9 and 10 months. Studies show that local control rates in patients converted to breast-conserving surgery are low providing that radiotherapy is given in a standard dose (Figure 10.6).
Figure 10.2 Breast cancer stained for oestrogen receptor: nuclei that stain brown indicate cells are receptor positive.
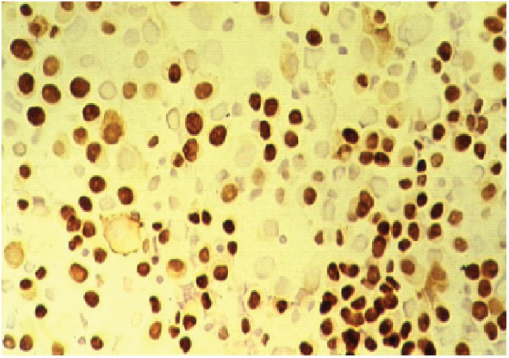
Figure 10.3 Response in the 024 randomised trial of letrozole v tamoxifen related degree of expression of oestrogen receptor as assessed by Allred score.
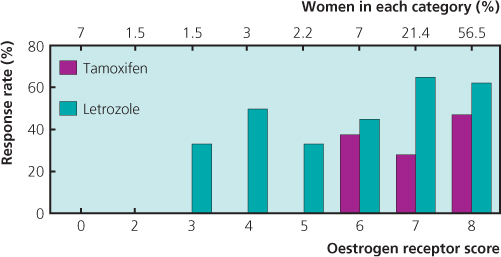
Figure 10.4 Breast-conserving surgery rates: Summary and meta-analysis of randomised trials comparing tamoxifen with the aromatase inhibitors letrozole, anastrozole and exemestane.
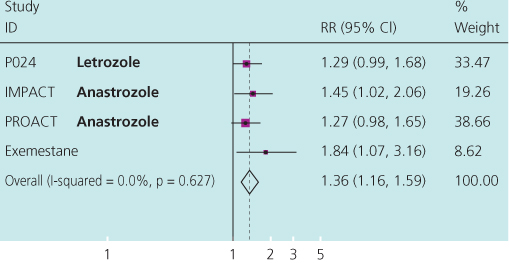
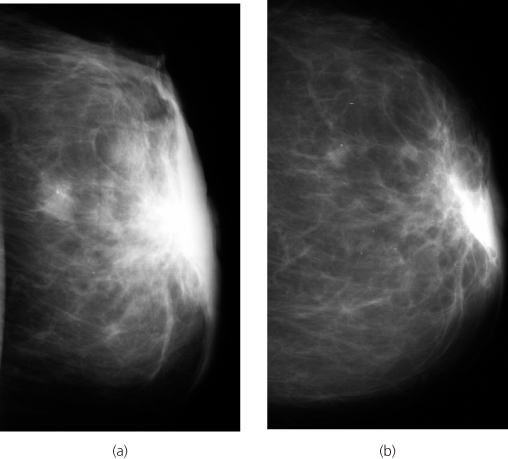
Figure 10.5 Serial ultrasound scans of breast tumour (a) before and (b) after 3 months treatment with letrozole 2.5mg: tumour significantly reduced in volume.
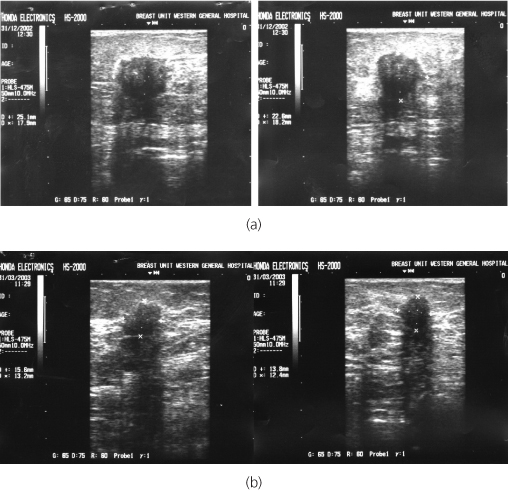
Figure 10.6 Local recurrence in patients after neoadjuvant endocrine therapy and breast conservation surgery with or without radiotherapy.
Locally Advanced Breast Cancer
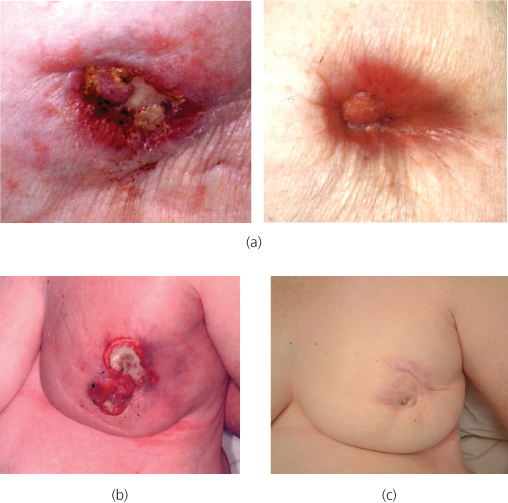
Patients with ER-positive disease should be considered for neoadjuvant treatment with an aromatase inhibitor. More than half of patients with ER-positive tumours treated by letrozole will have regression of disease to an extent that some form of local surgery is appropriate (Figure 10.7); response rates are highest in ER-rich tumours (Figures 10.3 and 10.8). ER-rich inflammatory cancers also respond to these agents. Patients with ER-positive tumours that show no response by three months should receive adequate locoregional treatment. Fit elderly patients with locally advanced ER-negative tumours can be treated by neoadjuvant chemotherapy or with radiotherapy with or without surgery. Regimens more suitable for use in an older population, such as weekly paclitaxel, are tailored to the patient’s general fitness. Patients who respond to primary chemotherapy may subsequently become suitable for surgical treatment and even breast-conserving surgery.
Figure 10.7 Locally advanced breast cancer—2 examples of before and after letrozole with re-epithelialisation of ulcerated cancer (previous 9.4 (i) and 9.4 (ii)).
Radiotherapy
Radiotherapy is delivered in a radical dose to the breast, chest wall and axillary nodes with full dose to skin. Selected patients with locally advanced breast cancer due to a direct skin involvement are suitable for an initial mastectomy or wide local excision with radiotherapy. Adjuvant systemic therapy after surgery should be based on the patient’s general condition, her wishes, oestrogen receptor status, the risk of recurrence and the absolute benefit for the individual accruing from treatment (Figure 10.6).
Adjuvant Systemic Therapy
All patients with tumours expressing any ER should be given adjuvant hormone therapy with or without chemotherapy. For patients with higher-risk ER-negative disease, adjuvant systemic chemotherapy is tailored to the patient’s fitness and risk of recurrence. Trastuzumab is licensed for use only with chemotherapy, but can be delivered safely to older patients with standard or modified chemotherapy regimens.
Metastatic Disease
Patients with ER-positive tumours should be treated with an aromatase inhibitor unless they have already received this as part of their adjuvant therapy. All three aromatase inhibitors have been shown to be more effective than tamoxifen in this group of patients, but the data are most impressive for letrozole. Bisphosphonates should be considered in patients with bony disease, to reduce fracture and improve pain. Patients with ER-negative tumours should be treated symptomatically. Palliative chemotherapy may provide a worthwhile response without appreciable toxicity in suitable patients. Palliative radiotherapy to local disease or painful bony metastases should be considered in symptomatic patients.
Very Elderly or Infirm Patients
An extremely small group of very elderly or infirm patients are unfit for treatments other than hormonal agents such as an aromatase inhibitor. It is only in those infirm patients with ER-positive breast cancer that hormonal agents should be considered as a sole treatment. Even in these patients, if aromatase agents do not establish disease control, limited surgery under local anaesthesia is possible and can improve any local symptoms.
Paget’s Disease of the Nipple
Paget’s disease is an eczematoid change of the nipple associated with an underlying malignancy and is present in 1–2% of patients with breast cancer (Figure 10.9 and Table 10.2). In half of these patients there is an underlying mass lesion and 90% of such patients have an invasive carcinoma. In those without a mass lesion, 30% have an invasive carcinoma and the remainder have in situ disease alone.
Table 10.2 Paget’s disease of the nipple.
|
*Sentinel node biopsy or axillary clearance as appropriate.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


