2South West Wales Cancer Institute, Singleton Hospital, Swansea, UK
Overview
- Locally advanced breast cancer has a much poorer outlook than operable breast cancer
- Specific types of breast cancer such as inflammatory breast cancer have a particularly poor outlook
- The cornerstone of treatment of locally advanced breast cancer is initial systemic therapy, trying to make the cancer operable followed by local surgery and/or radiotherapy
- Maintaining local control of breast cancer is an important goal in the treatment of locally advanced breast cancer
- Local recurrence after surgery in locally advanced breast cancers continues to be a problem
Locally advanced disease of the breast is characterised clinically by features suggesting infiltration of the skin or chest wall by tumour or matted involved axillary nodes. Large operable breast cancers and tumours fixed to muscle should not be considered as locally advanced.
Locally advanced breast cancer may arise because of:
- The position in the breast (for example peripheral or superficial).
- As a consequence of neglect (some patients do not present to hospital for months or years after they notice a mass). There is undoubtedly a major contribution from neglect, as many cases arise in elderly patients in whom the cancers behave in a rather indolent manner and are often well controlled by endocrine therapy alone if surgery is not feasible due to general frailty.
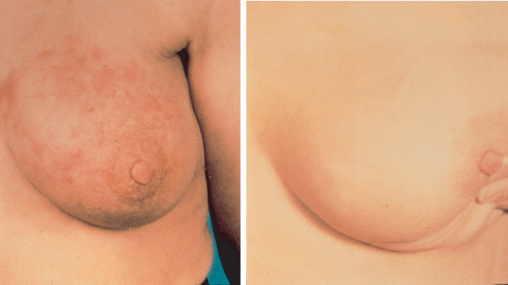
- Biological aggressiveness (this includes all inflammatory cancers and most with peau d’orange). Inflammatory carcinomas are uncommon and are characterised by brawny, oedematous, indurated and erythematous skin changes and have the worst prognosis of all locally advanced breast cancers (Figures 12.1 and 12.2).


Classification
Tumours involving chest wall muscles including not only the pectoralis major but underlying intercostal muscle and ribs are classified as T4a (Table 12.1). Cancers involving skin ulceration or with satellite nodules and peau d’orange are T4b. Tumours with both chest wall and skin involvement are T4c (Figures 12.3). Inflammatory breast cancers are classified as T4d.
Table 12.1 Clinical features of locally advanced breast cancer.
Skin
| Chest wall
|
Figure 12.3 (a) Locally advanced and ulcerated cancer right breast. (b) Ulcerated cancer with skin nodules.

Prognosis of Locally Advanced Breast Cancer
Recent data suggest that 5–10% of breast cancers present as locally advanced disease (Figure 12.4). Overall five-year survival is about 50%, but the prognosis relates to the biology of the underlying disease; indolent hormone-sensitive disease does much better than hormone-insensitive inflammatory breast cancer. Prognostic factors in locally advanced disease are similar to those in operable breast cancer: node status, tumour size, tumour biology including grade and proliferation rate, and response to treatment. A cancer that is locally advanced is much more likely than a cancer of the same size to have metastasised. For this reason patients with locally advanced breast cancer should have adequate staging investigations following diagnosis of invasive cancer.
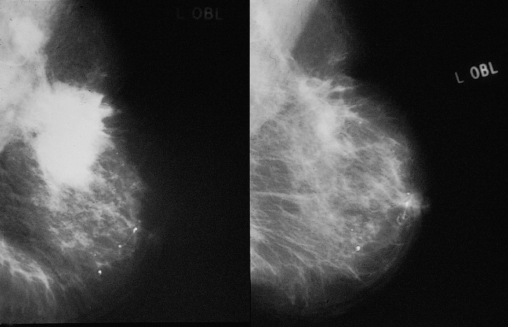
Figure 12.4 Mammogram of locally advanced breast tumour (left). Mammogram of the same breast (right) after hormone therapy showing substantial reduction in tumour volume (tumour was operable after treatment).
Treatment
Current treatments have increased the local control of disease and have reduced the rate of metastatic progression. Despite changes in treatment, local and regional relapse remains a major problem and affects up to half of patients.
Role of Systemic and Local Treatment
The mainstay of local treatment has been radiotherapy. This is because surgery, generally mastectomy, results in high rates of local recurrence. By contrast, though radiotherapy alone can produce high rates of local remission in both the breast and axilla, only 30% of patients remain free of locoregional disease at death. A sequence of appropriate systemic treatment and radiotherapy can increase the initial rate of local response to over 80% and has now superseded the use of radiotherapy alone.
The aim of systemic treatment in locally advanced breast cancer is to shrink the cancer and make it operable, thus improving local control and at the same time prolonging survival. Most randomised controlled trials in true locally advanced disease have been of exceedingly poor quality.
If patients are fit, systemic therapy is administered before local therapy with a view to reducing the extent of disease in the breast or axilla, or both (Figure 12.5). If the response is sufficient, surgery, mastectomy or breast-conserving surgery combined with axillary surgery should be performed. This should be followed by postmastectomy radiotherapy.
Choice of Systemic Treatment
Systemic treatment should be administered as part of a planned programme of combined systemic and local treatment (Tables 12.2 and 12.3). For frail patients treatment may initially be by endocrine therapy, with radiotherapy held in reserve for relapse.
Table 12.2 Factors affecting choice of systemic treatment for locally advanced breast cancer.
Hormonal treatment
| Chemotherapy
|
Table 12.3 Choice of systemic treatment for locally advanced breast cancer.
Hormonal treatment
| Chemotherapy
|
*Anastrozole and exemestane are other options.
**For example, doxorubicin and cyclophosphamide or epirubicin and cyclophosphamide and paclataxel or docetaxel.
Chemotherapy
Standard chemotherapy regimens have increased the initial rates of control. Studies of intensifying drug doses given in a fixed period either by giving smaller doses more frequently or by combining higher doses with factors to encourage regeneration of bone marrow does not produce survival benefits. Taxanes are being used increasingly in locally advanced breast cancer.
Results have shown significantly higher rates of clinical response and pathological complete remission with the addition of docetaxel to adriamycin and cyclophosphamide (Figures 12.6–12.8). Two studies have shown that patients responding to four courses of anthracycline-based chemotherapy and subsequently randomised to four further courses of docetaxel had a higher overall rate of response and pathological remission than those receiving four further cycles of the same chemotherapy.
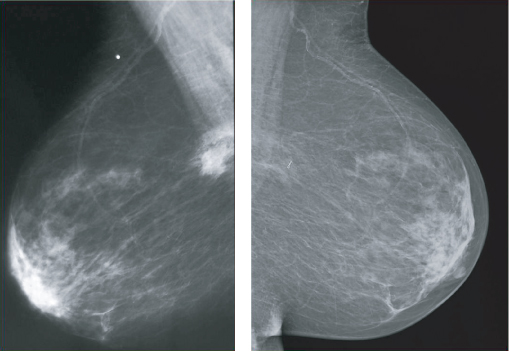
Figure 12.6 Locally advanced breast cancer (left) with complete clinical response after chemotherapy (right).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


