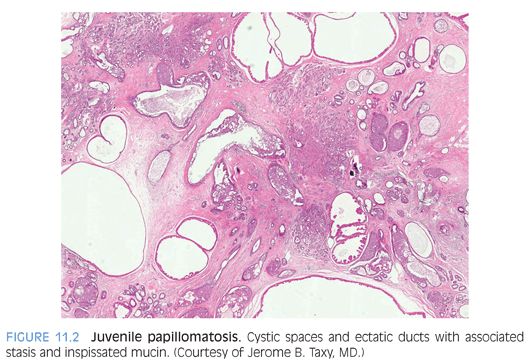
Papillary duct hyperplasia is an uncommon epithelial proliferation that occurs in adolescents and young women. It presents as a mass lesion and can be associated with nipple discharge. Grossly, multiple cystic spaces with papillary excrescences are present. Histologically, papillary duct hyperplasia shows papillomas with or without sclerosis, and papillomatosis composed of fibrovascular cores surfaced by a single or multiple epithelial cell layers. Myoepithelial hyperplasia and atypical ductal hyperplasia can also be associated with this lesion. In contrast to juvenile papillomatosis, cyst formation and duct stasis are absent. Excisional biopsy is recommended.
Reactive and Inflammatory Lesions
Reactive or infectious lesions of the breast can occur at any age and may be associated with trauma or foreign bodies.
Fat necrosis is commonly observed in association with trauma and presents as a localized, occasionally tender breast mass. On mammographic and clinical examination, such lesions may resemble carcinoma. On histologic examination of early lesions, lipid-laden macrophages, cystic spaces, foreign body giant cells, and acute inflammatory changes are seen. Fibrosis and collagen deposition, scant chronic inflammatory cells, and dystrophic calcifications are common features of older lesions. Fat necrosis is a self-limiting process and does not require therapy.
Idiopathic granulomatous lobular mastitis is a term reserved for instances where no inciting agent or causative microorganism is identified.5 It typically presents in late adolescence as a unilateral, painful breast mass or swelling and is associated with parity.6 Lesions range in size from 1 to 8 cm and are characterized by lobulocentric granulomatous inflammation accompanied by an acute and chronic inflammatory infiltrate. Fat necrosis, abscess formation, and fibrosis may also be present.6
Diabetic mastopathy is often seen as uni- or bilateral firm breast masses in young women with type 1 diabetes. However, patients with various autoimmune diseases can also exhibit a similar histology. Diabetic mastopathy is characterized by perilobular, periductal, and perivascular lymphocytic infiltrates; dense keloidal fibrosis; and the presence of epithelioid myofibroblasts in the stroma. Diabetic mastopathy likely represents an autoimmune response and frequently recurs.
Fibroepithelial and Stromal Lesions
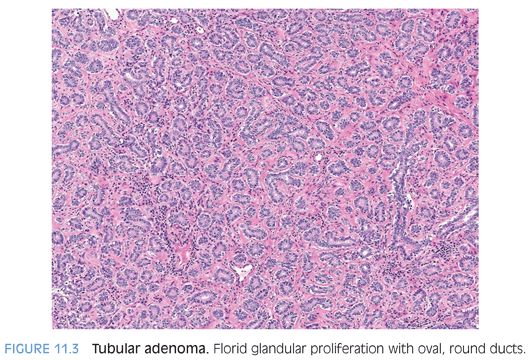
Fibroadenoma is the most common breast tumor observed clinically in adolescents and young women. A fibroadenoma typically presents as a 2- to 5-cm firm, freely mobile, well-circumscribed, and nontender mass with a rubbery, bulging, or myxoid cut surface. The two recognized histologic patterns, intracanalicular and pericanalicular, have no clinical or prognostic significance and may occur together in the same specimen. The intracanalicular pattern is characterized by slit-like, anastomosing channels compressed by the surrounding stroma, whereas the pericanalicular pattern resembles normal breast parenchyma and is characterized by open glandular structures. Usual ductal hyperplasia may occur in either pattern, and stromal mitoses are uncommon. Tubular adenoma is a variant of the pericanalicular pattern and is characterized by florid glandular proliferation with oval-to-round ducts (Fig. 11.3). Myxoid fibroadenomas can be associated with Carney complex.7
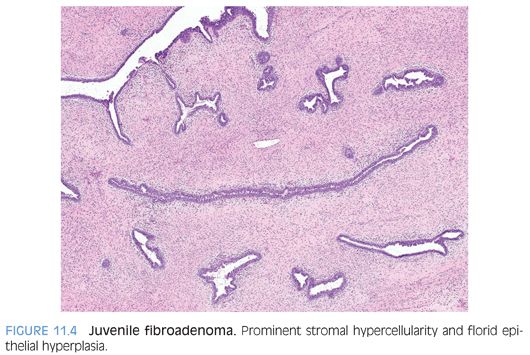
Juvenile fibroadenomas present in the second decade of life as well-circumscribed, rapidly enlarging masses that can reach significant size and cause deformities of the breast. Histologically, they are characterized by increased stromal cellularity and florid epithelial hyperplasia, which is in contrast to fibroadenoma (Fig. 11.4). Stromal atypia and mitoses are rare.8
A phyllodes tumor is an extremely rare biphasic lesion in the pediatric population, with gross and histologic features similar to fibroadenoma. Based on stromal cellularity, nuclear pleomorphism, stromal mitoses, tumor margin, and the presence of stromal overgrowth, they are graded as benign, borderline, or malignant. Most phyllodes tumors are benign and may represent a variant of fibroadenoma with leaflike areas. Phyllodes tumors often recur locally and have malignant potential. However, distant metastases are uncommon.
Pseudoangiomatous stromal hyperplasia (PASH) is occasionally seen in pediatric breast specimens from both genders and often resembles gynecomastia.9 PASH presents as a palpable, firm, mobile, and painless mass but can be multinodular or diffuse. Microscopic examination reveals slit-like anastomosing spaces lined by flattened stromal cells that can be plump, pleomorphic, and multinucleated and resemble a collection of vascular channels. The stromal lining cells are immunohistochemically positive for vimentin, CD34, and progesterone receptors and negative for factor VIII, distinguishing PASH from angiosarcoma.10,11
A granular cell tumor is an uncommon, benign lesion that affects both boys and girls and likely derives from peripheral nerve Schwann cells. The clinical and pathologic presentation may be indistinguishable from carcinoma. On biopsy, polygonal cells arranged in sheets or nests with granular eosinophilic cytoplasm and small hyperchromatic nuclei characterize the lesion. Immunohistochemical staining reveals positivity for S100, CD68, periodic acid–Schiff (PAS), and neuron-specific enolase (NSE). Complete surgical resection is curative.12–14
A mammary hamartoma is a benign lesion composed of architecturally disorganized mature breast structures. It typically presents in the pediatric population in females aged 11 to 17 years as a nontender, palpable mass with disorganized ducts and lobules surrounded by a collagenous stroma. The ducts and lobules vary in size and may be fused. A mammary hamartoma may recur if not completely excised.15
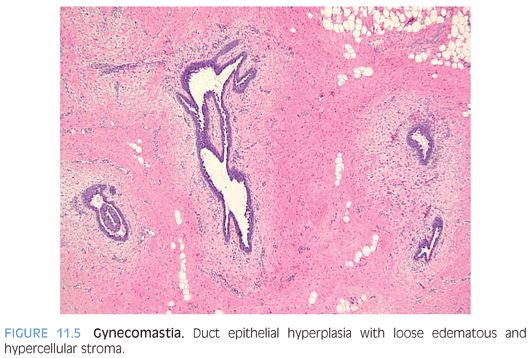
Gynecomastia is the most common abnormality of the male breast. Typically, a peripubertal boy presents with breast enlargement and a palpable, firm, and rubbery mass. There are two histologic types of gynecomastia that may occur together in the same specimen. The florid type is characterized by prominent duct epithelial hyperplasia with cribriforming or tufting; loose, edematous stroma; and increased cellularity (Fig. 11.5). Fibrous type gynecomastia is characterized by a mildly proliferative to atrophic epithelium and is accompanied by hyalinized fibrotic stroma. Carcinoma arising in gynecomastia is very rare.16
Breast Carcinoma
Primary breast carcinoma comprises less than 1% of pediatric malignant neoplasms17 and may affect both males and females.
Secretory carcinoma is the most common type seen in children. Typically, it presents as a well-circumscribed, nontender mass, with a subareolar predilection. Histologically, the epithelial component may be solid, papillary, cystic, or tubular. The tumor cells have a pale- to clear-staining cytoplasm with vacuolization, ovoid nuclei, and inconspicuous nucleoli. Prominent intra- and extracellular eosinophilic, PAS-positive secretion is present throughout the tumor. Some tumors express a t(12;15)–associated gene fusion product, ETV6-NTRK, which is also found in other pediatric mesenchymal neoplasms.18,19 Secretory carcinomas are mostly estrogen receptor positive and have a favorable prognosis.
Other Lesions
Vascular tumors including hemangiomas, angiomatosis, and hemangiopericytomas have been described in the pediatric population. Angiosarcoma in children is incredibly rare. Rhabdomyosarcoma (RMS), leukemia, and lymphoma are known to metastasize to the breast.
THE FEMALE REPRODUCTIVE TRACT
Vagina and Cervix
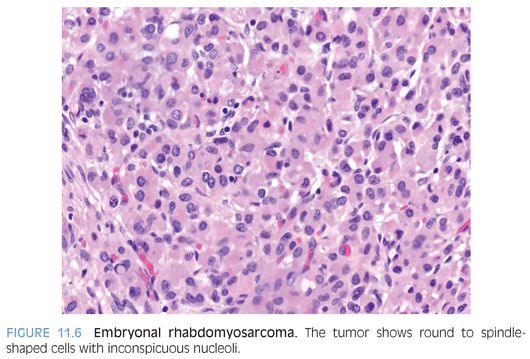
Embryonal RMS is the most common malignant tumor of the vagina and typically occurs in children younger than 5 years of age. Frequent presentations include bloody vaginal discharge20 or a protruding “grapelike” anterior vaginal mass. The botryoid embryonal subtype (sarcoma botryoides) is the predominant type seen in the vagina and forms a subepithelial cambium layer with condensation of polyhedral rhabdomyoblasts that are scattered in a loose, fibromyxomatous, or collagenous stroma. The tumor cells are round to spindle shaped, have inconspicuous nucleoli, and cytoplasmic cross-striations may be present (Fig. 11.6). Embryonal RMS expresses muscle-specific antibodies, such as myoglobin, myogenin, and desmin (Fig. 11.7). Combined multiagent chemotherapy, surgery, and radiation therapy have improved its clinical outcome, with patients with sarcoma botryoides having a survival rate of more than 90%.