Varicella-Zoster Virus Infections
Sophie Hambleton
The human α-herpesvirus, varicella-zoster virus (VZV), is a highly successful pathogen that has coevolved with its human hosts over millennia. The majority of the world’s population has experienced primary VZV infection as varicella (“chickenpox”), with the acquisition of both lifelong immunity against reinfection and the risk of viral reactivation as zoster (“shingles”). In most children, chickenpox is a mild illness in which viral replication rapidly subsides. However, severe and complicated varicella does occur in previously healthy children and at much higher rates in certain risk groups (eg, immunocompromised persons, adults, newborns). A successful vaccination program against varicella is having profound effects on the epidemiology of VZV in the United States.
 EPIDEMIOLOGY
EPIDEMIOLOGY
Varicella is acquired through close contact with an infected individual. Natural varicella is the most communicable form of varicellazoster virus (VZV) disease: household attack rates approach 90%, and outbreaks occur readily within groups of susceptible children.1 A milder form of varicella, occurring in vaccinated individuals with partial immunity, is only one third as transmissible,2 whereas zoster represents the least contagious form of disease.
In unvaccinated populations in temperate climates, seasonal peaks of varicella occur in the spring. These epidemics occur on a background of endemic disease, and 84% of children acquire infection by age 15 years.3,4 In contrast, the incidence of varicella in the tropics does not vary by season and tends to be delayed until adolescence or adult life.3 At this age, morbidity and mortality from varicella are significantly greater than in childhood, for reasons that are poorly understood.
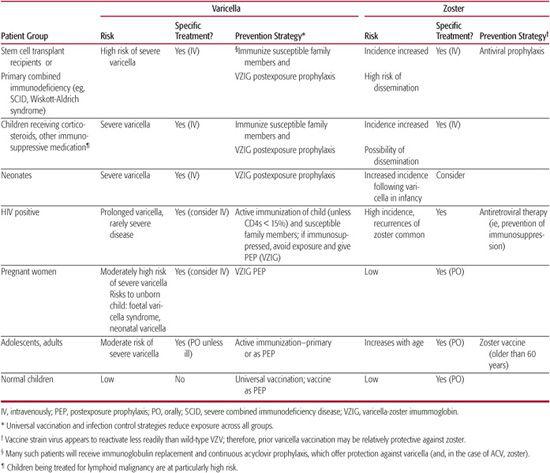
Aside from adult age, the greatest risks for severe/fatal varicella are cellular immunocompromise (congenital or acquired), infancy (particularly, the neonatal period), and pregnancy (Table 314-1). In the prevaccine era, varicella was associated with approximately 11,000 hospitalizations and in excess of 100 deaths annually in the United States.5,6 Much of this burden was borne by previously healthy children. The epidemiology of VZV has been transformed since the introduction of universal varicella vaccination in the mid-1990s. The incidence of varicella has been strikingly reduced across all age groups, with concomitant reductions in office visits, hospitalizations, and deaths from varicella.7-10
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Infectious virus is shed from the cutaneous lesions of varicella and zoster, and probably also from the respiratory tract 1 to 2 days prior to chickenpox. Thus, the infectious period extends from up to 48 hours before the appearance of rash until all skin lesions are crusted over, usually about 5 days in normal hosts. Following infectious contact, the incubation period for chickenpox is 10 to 21 days (median 14 days, up to 28 days following varicella-zoster immunoglobin [VZIG]). Varicella-zoster virus (VZV) viremia is well documented in both immunocompetent and immunocompromised children and predates the chickenpox rash by approximately 5 days.11-13 Virus can be detected in circulating lymphocytes and monocytes. These are believed to disseminate VZV to the skin, where local spread of virus produces the lesions characteristic of varicella. 
Table 314-1. Patients at High Risk to Develop Severe Varicella Zoster Virus Infections and Guidence to Therapy
In the immunocompetent host, VZV viremia and the appearance of new skin lesions are curtailed within a few days by a vigorous cellular immune response comprising both natural killer (NK) and antigen-specific (T-cell) components.17 Conversely, the failure to mount antigen-specific cellular responses is associated with progressive viral replication and dissemination, and a potentially fatal outcome.
A host humoral response is also detectable within 4 days of the onset of the exanthem and can confer passive immunity; thus, pooled immunoglobulin derived from VZV-immune donors can be used to protect VZV-exposed subjects at high risk of severe chickenpox.1 The presence of VZV-specific antibodies is also the best available correlate of protection against primary infection, but is irrelevant to the risk of secondary (reactivation) disease.
 CLINICAL FEATURES
CLINICAL FEATURES
Prodromal symptoms of low-grade fever, headache, and malaise usually precede the characteristic vesicular exanthem by 24 to 48 hours. The rash typically begins as “dew drops on rose petals,” appearing on the face, trunk, or scalp and eventually spreading to involve the entire body (Fig. 314-1). The total number of lesions may vary from 50 to 500. The vesicles appear in crops for the first 3 to 5 days of the illness. Lesions on the skin are usually intensely pruritic but not painful; however, lesions on mucous membranes become shallow ulcers, which may be painful. In the absence of secondary bacterial infection, healing occurs over 7 to 10 days without scar mformation, although discrete hypo- or hyperpigmented lesions may persist for several months.

FIGURE 314-1. Typical varicella lesions. Mulitple, very pruritic, erythematous papules, vesicles (“dewdrops on a rose petal”), and crusted papules on erythematous, edematous bases on the face and neck. (Source: Wolff K, Johnson RA. Fitzpatrick’s Color Atlas & Synopsis of Clinical Dermatology. 6th ed. New York: McGraw-Hill; 2009.)
Immunity following varicella is usually life long; however, primary infection in circumstances in which immune responses are incomplete may predispose to a second episode of varicella. “Breakthrough” varicella is the term applied to wild-type disease in an individual who has previously received the live-attenuated varicella vaccine. This is generally a highly modified illness in which skin lesions are few, systemic features such as fever are absent, and transmissibility is reduced by around two thirds compared with unmodified varicella.2,22 Not surprisingly, this may pose diagnostic difficulties.
Varicella in the normal host is generally a benign self-limited disease. The occurrence of significant fever beyond the first 48 hours of exanthema, as well as the progression of erythema or tenderness around crusting lesions, should raise suspicion for secondary bacterial infection. Likewise, hemorrhagic lesions, significant abdominal pain or vomiting, or altered mental status should alert clinicians to possible complications that require prompt intervention.
Immune Deficiency
Individuals with congenital or acquired immune deficiencies that affect their ability to mount a cellular immune response to varicella-zoster virus (VZV) are at risk for progressive disseminated varicella, whereas individuals with isolated humoral immune deficiency are not (Table 314-1). Children being treated for lymphoid malignancy are at particular risk of fatal varicella.34 Progressive disseminated varicella involves multiple organ systems. Its onset may be heralded by severe abdominal pain or back pain before the appearance of a rash. Fever reaching to 40°C to 41°C (104°F–105.8°F) may persist for several days. Severe hepatitis, pneumonitis, thrombocytopenia, coagulopathy, encephalitis, and other organ dysfunction may ensue. Mortality is significant, even with treatment and supportive care. Because their ability to terminate viral replication is diminished, immunocompromised individuals with varicella are contagious for an extended period. Individuals with acquired immunodeficiency due to infection with HIV do not appear to be at the same degree of risk for progressive disseminated varicella.35,36 Rather, varicella may persist for several weeks to months. The incidence of zoster is extremely high, and recurrent disease is common.
Congenital and Neonatal Disease
When maternal varicella occurs in the first 20 weeks of gestation, approximately 0.4% of fetuses may manifest findings associated with varicella embryopathy.40,41 Among the constellation of features of congenital varicella-zoster virus (VZV) are cutaneous defects; classic cicatricial skin scarring and limb atrophy; microcephaly; cortical atrophy; seizures; chorioretinitis; microphthalmia; and significant neurologic deficits. Autonomic nervous system involvement may manifest as difficulty with sphincter control, intestinal obstruction, Horner syndrome, or other cranial nerve neuropathies (Moebius syndrome). Infants born to mothers who develop varicella less than 5 days before delivery or 2 days after delivery are at risk of severe or lethal neonatal varicella.42
 DIAGNOSIS
DIAGNOSIS
The diagnosis of varicella is usually clinically apparent, although the child with few lesions may go undiagnosed or be misdiagnosed as having “insect bites.” 
In the face of diagnostic uncertainty and an ill patient, VZV can be identified by a variety of tests. The preferred method is immunofluorescent antibody staining (DFA) of cells scraped from the base of a lesion using VZV-specific antibodies. This provides a rapid and specific way to diagnose VZV infection. Culture is slow and insensitive. Polymerase chain reaction (PCR) techniques for VZV are not yet in general use but provide helpful additional information in reference laboratory and research settings. In particular, PCR typing methods can distinguish vaccine and wild-type strains of virus.
A variety of serologic tests for VZV have been used to determine preexisting infection, susceptibility to disease, and response to immunization; they are occasionally helpful in the context of varicella diagnosis.23 The fluorescent antibody–to–membrane antigen (FAMA) assay is the “gold standard” for determining biologically significant antibody; the technique, however, is cumbersome. Latex agglutination provides a convenient and rapid test, although negative sera should be retested at lower dilution to exclude a prozone effect. Commercially available VZVIgG enzyme-linked immunosorbent assays (ELISAs) are often used to identify susceptible individuals who may be at risk for severe disease, such as those requiring transplantation. These tests do not reliably identify vaccine-derived immunity.
 THERAPY
THERAPY
Children with risk factors for and/or symptoms of severe/complicated varicella must be identified promptly, and appropriate specialist care instituted. However, most children with varicella do not require specific therapy but rather general supportive measures, such as acetaminophen for fever, possibly a sedative antihistamine for pruritus at night, and advice on minimizing the risk of secondary infection and scarring (eg, keep nails short and skin clean, try to avoid scratching).
Oral acyclovir (ACV), begun within 24 hours of the appearance of rash, significantly decreases the number and duration of new lesions.24 ACV therapy should be considered in immunocompe-tent individuals at risk for more severe disease: for example, a second case in a household, adolescents, and adults.25,26 For maximum effectiveness, therapy should be initiated as soon as possible after the appearance of rash; after 24 hours, little benefit attaches to starting ACV in uncomplicated varicella. The suggested dose of oral ACV for the normal host is 20 mg/kg/dose (max 800 mg/dose) 4 times daily for 5 to 7 days.
Intravenous ACV is indicated for the treatment of the immunocompromised child with varicella or zoster because of the danger of dissemination. Suggested dosage of intravenous ACV for immunocompromised children ages 3 months to 12 years is 1500 mg/m2/day given in 3 divided doses. Outside this age range, dosing is calculated according to body weight (30–60 mg/kg/day up to 3 months and 30 mg/kg/day for immunocompromised children older than 12 years). The duration of therapy is usually 5 to 10 days or until lesions are crusted. The bio-availability of ACV following oral administration is limited and is unlikely to be adequate for these patients. The role of antiviral agents with better oral bioavailability, such as valaciclovir and famciclovir, has not been established for the treatment of varicella in children.
Intravenous ACV is also indicated for neonates who develop varicella from their mothers and should be considered for neonates who develop varicella following household exposure. The term infant should receive 10 to 20 mg/kg/dose given every 8 hours; in premature infants, the dosing interval should be decreased to every 12 hours.
 COMPLICATIONS
COMPLICATIONS
The rate of severe or complicated chickenpox is low among immunocompetent children, but such cases are numerically common in unvaccinated populations.27 The most frequent complication in the young is secondary bacterial infection of the skin. Many of the other complications of chickenpox reflect overwhelming viral infection and are more likely to occur in the context of defective cell-mediated immunity.
Secondary Bacterial Infection
Scratching of the intensely itchy skin lesions of chickenpox often leads to the introduction of bacteria, typically Staphylococcus aureus or Streptococcus pyogenes. Local skin infection in a well child can be treated with an oral antibiotic and kept under review. Progression of erythema around lesions, formation of bullae, or development of regional lymphadenitis should prompt consideration of intravenous antibiotic therapy. Recent varicella confers a significantly increased risk of invasive bacterial disease, particularly group A streptococcal (GAS) infections; these include necrotizing fasciitis, bacteremia, pneumonia, empyema, and toxic shock syndrome. It has been estimated that varicella directly precedes approximately 15% of invasive GAS infections.28 Pain in a muscle group, together with circumferential swelling of an extremity, may reflect necrotizing fasciitis despite the lack of significant overlying erythema. Urgent MRI or ultra-sonography can be useful in defining soft tissue involvement. These severe infectious complications require that if a child with chickenpox appears excessively ill, especially with a recurrence of fever, urgent hospital evaluation is required.
Varicella Pneumonia 
Asymptomatic radiographic changes are common in immunocompetent adults with chicken-pox, but varicella pneumonia affects only about 1:400.29 In contrast, pneumonia commonly accompanies chickenpox in immunocompromised children. Respiratory symptoms—dyspnea, tachypnea, chest tightness, cough—develop in the context of acute varicella (usually 1–6 days after the onset of the rash) and may progress rapidly to respiratory failure. The severity of clinical signs is a poor guide to prognosis; therefore, the patient with new respiratory symptoms in the context of varicella should be urgently evaluated. Intravenous antiviral therapy and improved intensive care have markedly improved survival of these patients over recent years, but deaths continue to occur.
Neurologic Complications
Chickenpox is classically associated with three neurologic pictures: (1) cerebellar ataxia, (2) encephalitis, and (3) Reye syndrome. Rarely, it has been associated with Guillain-Barré syndrome, stroke, transverse myelitis, and aseptic meningitis.30
Cerebellar ataxia complicates approximately 1 in 4000 cases of varicella31 and usually follows the onset of rash, making the diagnosis clear. Vomiting and headache often accompany the ataxia, whereas only one fourth of patients experience neck stiffness or nystagmus. The role of antiviral therapy is unclear because complete resolution of symptoms is the rule, but has been proposed for those patients with polymerase chain reaction evidence of VZV within the cerebrospinal fluid.30
Encephalitis has been reported to complicate 1 to 2 per 100,000 cases of varicella, and is marked by fever, altered level of consciousness, headache, photophobia, and seizures. Such patients require urgent diagnostic evaluation and therapy, including antiviral and supportive care. Varicella encephalitis is associated with a low but significant mortality rate; rarely, survivors suffer long-term sequelae.
Reye syndrome, once linked to chickenpox and influenza in children, has become exceedingly rare since the recognition of an epidemio-logic link to the use of aspirin.32 The syndrome consists of a progressive encephalopathy accompanied by hepatotoxicity and a 30% risk of death (see Chapter 421).
 PREVENTION
PREVENTION
There are three ways in which varicella can be prevented: (1) avoidance of exposure, (2) postexposure prophylaxis, and (3) primary prophylaxis. As part of their regular medical care, immunocompromised individuals at risk of severe chickenpox should be identified and counseled. If there is no clinical history of chicken-pox (or zoster), their varicella-zoster virus (VZV) immune status should be clarified by serologic testing. Many such individuals turn out to be VZV seropositive and, thus, are at very low risk of varicella. VZV-seronegative individuals at risk of severe varicella should try to avoid contact with infectious persons. This can be facilitated by actively immunizing susceptible family members and health care workers, and by excluding infectious individuals from schools and open hospital areas. Should exposure occur, high-risk susceptible patients should be encouraged to present as soon as possible for evaluation and postexposure immunoprophylaxis with varicella-zoster immune globulin (VZIG; VariZIG in the United States). This intramuscular preparation confers significant (but not 100%) protection if given within 96 hours of exposure.  However, it is an expensive blood product in relatively short supply; hence, clear and specific national guidance on its use should be followed. The criteria for use of VZIG include (1) high risk of severe varicella AND (2) significant exposure AND (3) current VZV seronegativity. High-risk groups include immunocompromised children and pregnant women without a prior history of varicella, newborn infants whose mothers developed varicella less than 5 days before or 2 days after delivery, premature infants more than 28 weeks’ gestation born to women with negative VZV histories, and premature infants less than 28 weeks’ gestation regardless of maternal history when a significant exposure has occurred. “Exposure” implies household contact, sharing a room for 15 minutes, or face-to-face contact with a case of varicella during the infectious period (from 2 days before the onset of rash until all lesions are crusted over). Zoster is only considered infectious if skin lesions are exposed (eg, face) or disseminated, or if the affected individual is immunosuppressed or in hospital. VZV seronegativity should be confirmed prior to VZIG administration, unless this would produce an unacceptable delay. Individuals receiving immunoglobulin replacement therapy generally achieve protective levels of VZV-specific immunity and do not require VZIG.
However, it is an expensive blood product in relatively short supply; hence, clear and specific national guidance on its use should be followed. The criteria for use of VZIG include (1) high risk of severe varicella AND (2) significant exposure AND (3) current VZV seronegativity. High-risk groups include immunocompromised children and pregnant women without a prior history of varicella, newborn infants whose mothers developed varicella less than 5 days before or 2 days after delivery, premature infants more than 28 weeks’ gestation born to women with negative VZV histories, and premature infants less than 28 weeks’ gestation regardless of maternal history when a significant exposure has occurred. “Exposure” implies household contact, sharing a room for 15 minutes, or face-to-face contact with a case of varicella during the infectious period (from 2 days before the onset of rash until all lesions are crusted over). Zoster is only considered infectious if skin lesions are exposed (eg, face) or disseminated, or if the affected individual is immunosuppressed or in hospital. VZV seronegativity should be confirmed prior to VZIG administration, unless this would produce an unacceptable delay. Individuals receiving immunoglobulin replacement therapy generally achieve protective levels of VZV-specific immunity and do not require VZIG.
When VZIG is in short supply, oral acyclovir is recommended for postexposure prophylaxis, despite the lack of an evidence base for this practice in immunocompromised persons. This represents an “off-label” use of acyclovir, and therapy should be undertaken in discussion with a specialist. As with all postexposure prophylaxis, recipients should be counseled to seek medical advice in the event that symptoms of chickenpox do develop. Both VZIG and acyclovir (ACV) can be associated with lengthening of the incubation period.
A highly effective live-attenuated vaccine against varicella has been in widespread use in the United States since 1995, and more recently, has been introduced to several European countries. The vaccine offers protection directly to both immunized individuals and the community as a whole through herd immunity. With few exceptions, the vaccine is contra-indicated in the immunocompromised, who therefore benefit from it only indirectly.38 Live vaccine is also effective as postexposure prophylaxis in the immunocompetent, making this a useful intervention in the outbreak setting. Two doses are given 4 to 8 weeks apart and are generally well tolerated, the main adverse reaction being a mild vaccine-associated rash.43
ZOSTER (SHINGLES)
Varicella-zoster virus (VZV) is not eliminated from the host when varicella-associated viremia subsides. Rather, the virus establishes latent infection within sensory neurons of the dorsal root and trigeminal ganglia. Zoster (shingles) is the recurrent disease that results from viral reactivation. The incidence of zoster increases with increasing age, believed to be in response to declining immunity to VZV.44 Other risk groups, most of whom have impairments of cellular immunity, are shown in Table 314-1. 
Zoster classically appears as a unilateral process involving a single or possibly two adjacent dermatomes. Thoracic dermatomes are most often involved, followed by cranial nerve and lumbosacral regions. The lesions often appear first as patches of erythema, which then develop groups of vesicles. The lesions progress over 3 to 5 days, and usually dry and crust within 2 weeks. Pain or paresthesia within the involved dermatome may precede the vesicular eruption. Persistent pain, known as postherpetic neuralgia (PHN), is relatively uncommon in children.30
Generalized or disseminated zoster may occur in immunocompromised hosts. Multiorgan involvement may precede or follow rash in the untreated immunocompromised host, as has been described for varicella in this high-risk population. Immunosuppressed patients are also at relatively higher risk for PHN.50
Zoster should in general prompt specific treatment because antiviral agents given within 72 hours of onset reduce the severity and duration of symptoms and PHN.51 Oral therapy is usually suitable for immunocompetent persons, but intravenous acyclovir should be considered in those at risk of severe disease. Pain relief and other supportive measures may be required. In addition, individuals with ophthalmic involvement require specific evaluation and management. Disseminated zoster is a severe systemic illness that may require intensive care, as for severe varicella.
REFERENCES
See references on DVD.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


