Chapter 38 Uterovaginal displacements, damage and prolapse
UTERINE DISPLACEMENTS
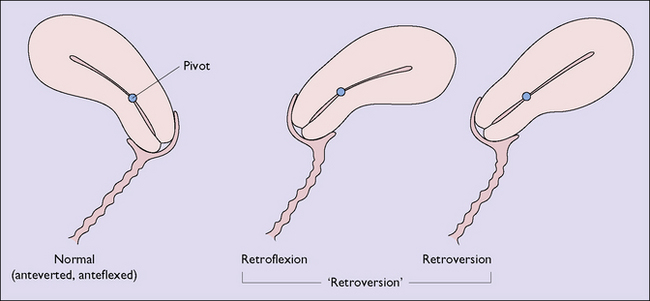
The uterus is an organ that normally pivots about an axis formed by the cardinal ligaments at the level of the internal cervical os. In 90% of women the uterus is anteflexed and anteverted, lying on the urinary bladder and moving backwards as the bladder fills. In 10% of women the uterus is retroflexed and may be retroverted (Fig. 38.1). This is a developmental occurrence. The uterus is mobile and can be moved by inserting a finger in the posterior vaginal fornix. In spite of anecdotal statements, a mobile retroverted uterus is not a cause of infertility, abortion or backache.
Diagnosis
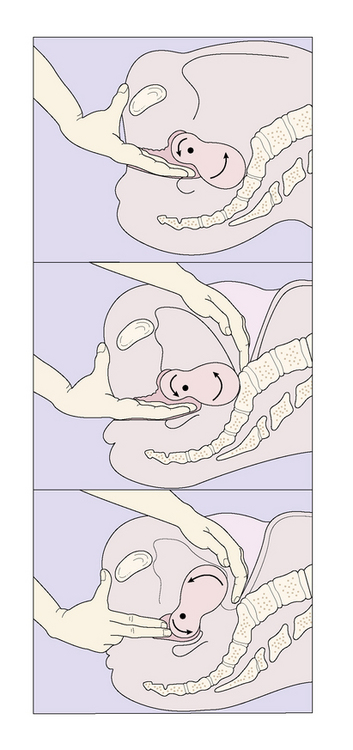
A clinical finding that the uterus is retroverted and is accompanied by symptoms should alert the medical practitioner to determine whether the retroversion can be corrected by manipulation (Fig. 38.2). If it can, it is not the cause of the symptoms. If it cannot be manipulated it may be the cause of the symptoms.
UTEROVAGINAL DAMAGE AND INJURIES
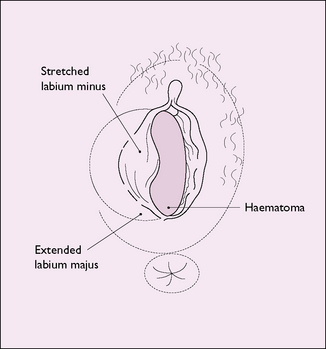
Injury to the vulvovaginal area may occur, for example if a girl or woman falls astride some object or is kicked. The vagina may be damaged or a haematoma may form in the vulva (Fig. 38.3). Injury may also occur if a young girl or a postmenopausal woman is sexually assaulted.
Injury resulting from childbirth is discussed on page 81. Occasionally a vaginal tear is not sutured immediately, and the woman attends a medical practitioner some time later. On inspection the vaginal entrance is seen to gape and the perineal muscles are separated (Fig. 38.4
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


