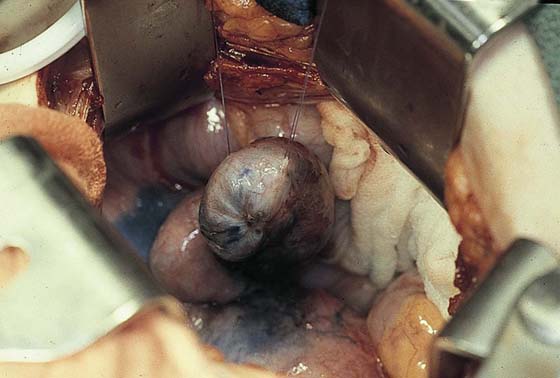
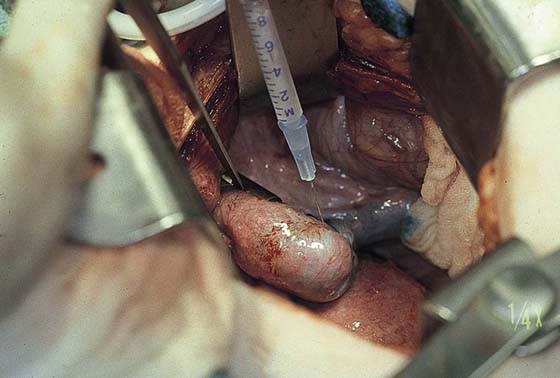
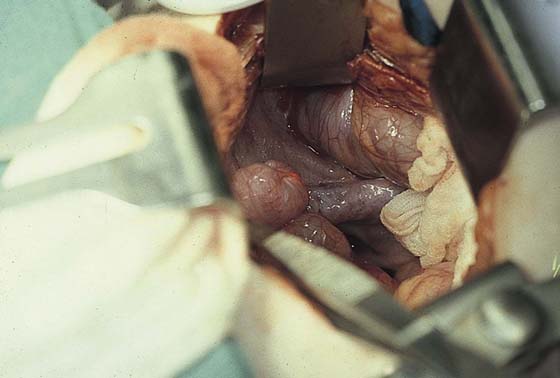
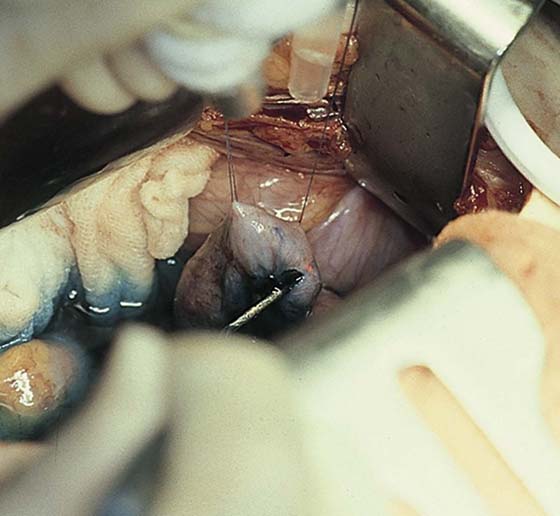
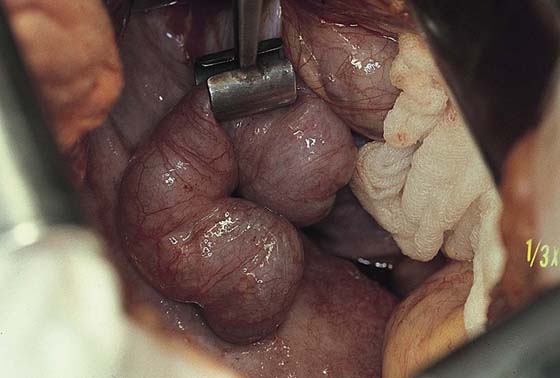
CHAPTER 29 The oviducts may be obstructed principally at three locations: (1) at the cornua; (2) at the fimbriated end; and (3) at any point between these two locations. The causes of oviductal obstruction are myriad and include infection, ectopic pregnancy, endometriosis, intentional tubal ligation, and partial salpingectomy. Before surgery is performed, a thorough diagnostic survey should be done, including laparoscopy, chromotubation, and hysterosalpingography. Several of the techniques described here can be performed by laparoscopy, laparotomy, or microsurgery. Similarly, the incisional portions of these procedures may be performed with conventional mechanical devices, superpulsed carbon dioxide (CO2) lasers, or electrosurgical tools. The author prefers to utilize a variety of instruments, basing selection on the circumstances of the pathology and the relative advantages of a particular device for a specific circumstance. These surgical techniques use fine instruments, gentle tissue manipulation, small-gauge suture material, and needles. Compulsive hemostasis is required for successful outcomes. A hydrosalpinx connotes a damaged tube (Fig. 29–1). Methylene blue dye should be injected transcervically to determine whether the tube fills. If the tube distends with the dye, then a fimbrioplasty may be attempted (Fig. 29–2). Traction sutures of 4-0 Vicryl are placed to permit gentle tissue manipulation and to obtain good stability of the oviduct during surgery (Fig. 29–3). A CO2 superpulsed laser (Lumenis, Santa Clara, California) set at 12 W at 300 pulses/sec is focused to deliver a 1-mm-diameter spot (Fig. 29–4). A hole is drilled into the central point of the fimbrial adhesion (Fig. 29–5). Blue dye spews forth as the oviductal canal is entered. A lacrimal probe is inserted into the opening. Four radial cuts are made from the central point and are carried into the tubal lumen (Fig. 29–6). These may range from 3 to 10 mm in length. The edges of each radial cut are then sutured back to the tubal serosa or are laser brushed to create a cuff (Fig. 29–7). The preferred suture material is 5-0 polydioxanone (PDS)/Vicryl. The cuff exposes to the ovary a large surface area of tubal ciliated cells. Patency is again checked by retrograde injection of methylene blue dye (Fig. 29–8). FIGURE 29–1 The distended oviduct is secured for inspection with a tube clamp. This figure demonstrates a classic hydrosalpinx. FIGURE 29–2 The oviduct is filled with methylene blue injected retrogradely through a transcervical Cohen-Eder cannula. FIGURE 29–3 A 1 : 200 solution of vasopressin is injected into the planned operative site with a 25-gauge needle. FIGURE 29–4 The helium-neon aiming beam of a carbon dioxide (CO2) superpulsed laser is aimed at the dimple in the fimbriated end of the hydrosalpinx. This represents the site of central agglutination of the fimbria. FIGURE 29–5 Entry into the tubal lumen is signified by the leakage of methylene blue–tinged fluid. A metal probe is inserted into the lumen.
Tuboplasty
Fimbrioplasty (Hydrosalpinx)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


