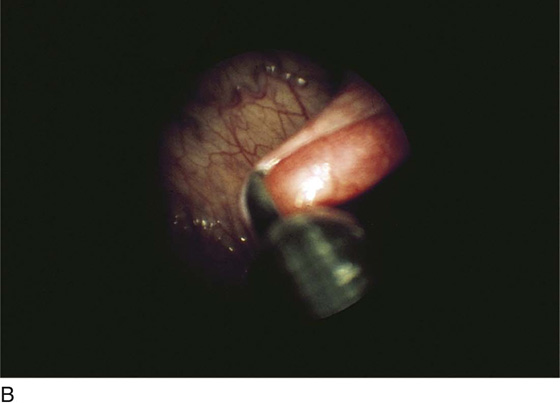
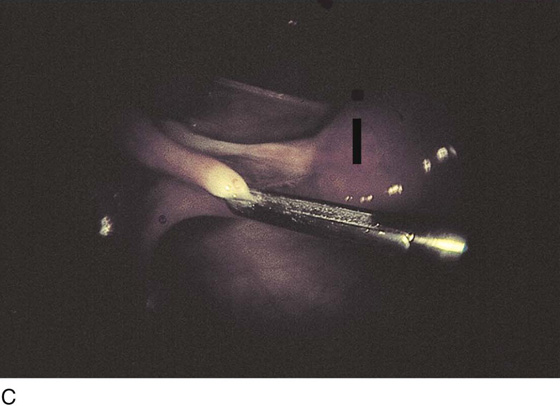
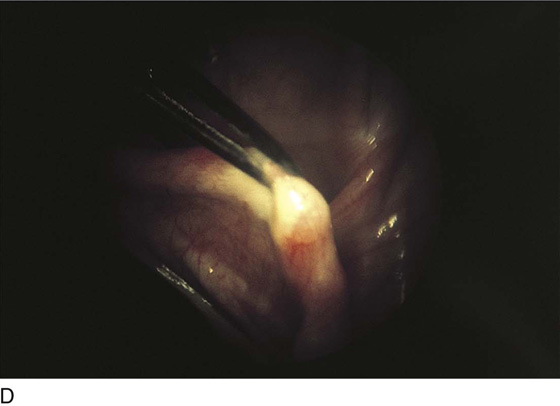
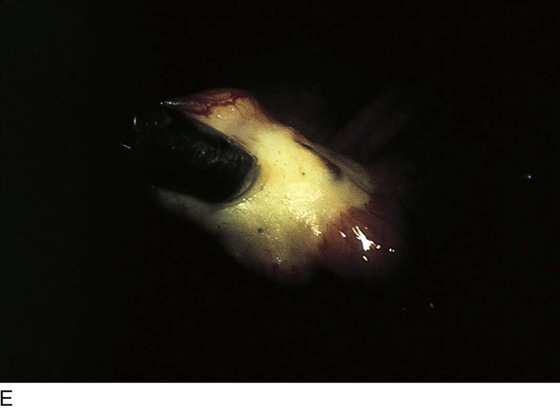
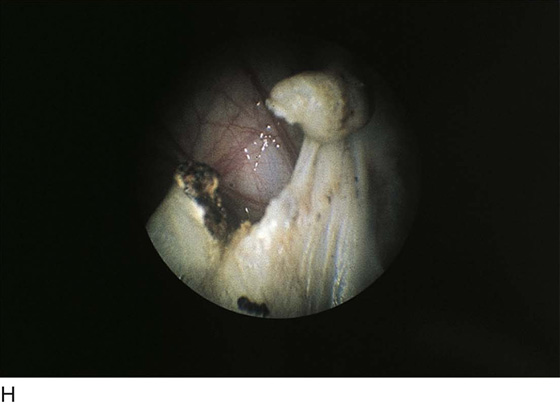
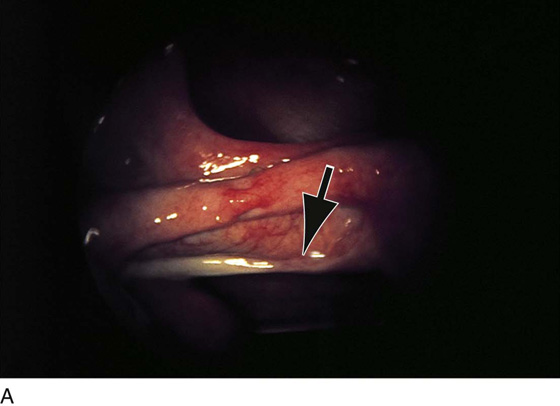
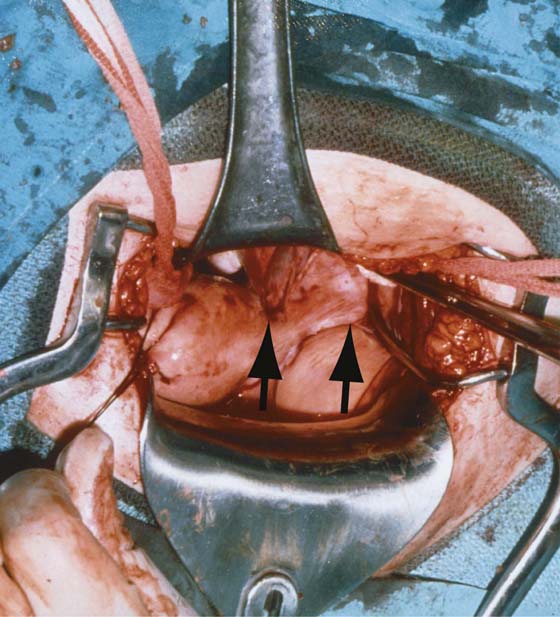
CHAPTER 30 Tubal interruption, or bilateral partial salpingectomy, is a relatively easy and direct method of accomplishing surgical sterilization. Typically, this operation is performed at the time of cesarean section, or immediately postpartum in the case of vaginal delivery. Two operations are especially well suited for these particular circumstances. Modified Irving and Pomeroy techniques are enhanced as further tubal separation may be anticipated as the result of rapid regression of the uterine mass to a nonpregnant size and shape. Most interval sterilizations are performed via laparoscopy (Fig. 30–1A–H). The Uchida operation can be performed as a postpartum or an interval operation. Simple fimbriectomy or ampullary-isthmus excision is well suited as an interim operation. Whatever method is selected for tubal sterilization, certain precepts must be followed. First, an executed sterilization permit must be obtained for each and every patient, and each patient must be informed that the operation is a permanent sterilization procedure, and that there is no possibility of pregnancy in the future. Paradoxically, patients also must be told that a failure rate is associated with each operation. Second, the tube must be carefully distinguished from the two other structures located at the top of the broad ligament: most anteriorly, the round ligament, and most posteriorly, the utero-ovarian ligament (Fig. 30–2). Next the tube should be traced from the uterus to the fimbriated end and then secured with a Babcock clamp or stay suture-ligature. Finally, the location of the ipsilateral ovary should be viewed relative to the tube. The proximal and distal ends of the tube are grasped with Babcock clamps, and the stretched tube is held straight and elevated upward so as to clearly expose the mesosalpinx. FIGURE 30–1 A. Endoscopic view of the oviduct. Note anteriorly the curving round ligament and below (arrow) the whitish utero-ovarian ligament. B. The close-up of the tube grasped by the forceps. C. Panoramic view from the front (anterior) detailing the three tubular structures emanating from the top of the uterus (dark line). Grasped within the forceps is the tube. Anteriorly is the round ligament and posteriorly the utero-ovarian ligament. D. Electric current is applied via the grasping forceps. White blanching (coagulation) occurs above and below the point where the tube is held by the forceps. E. Close-up view of the extensive coagulation. F. To achieve satisfactory hemostasis, coagulation continues until the mesosalpinx is coagulated. G. A coagulated segment of the oviduct is removed and sent to pathology. H. Completed laparoscopic bilateral partial salpingectomy performed by electrosurgical coagulation. FIGURE 30–2 Laparotomy performed on a woman who had a failed bilateral partial salpingectomy. The failure was caused by bilateral ligation of the round ligaments rather than ligation of the oviducts (arrows). A window is made under a 3-cm segment of tube with the use of fine, straight mosquito clamps, thus securing fat and vessels within the mesosalpinx (Fig. 30–3A). Next, Kelly clamps are applied to the uterine end and to the fimbriated end of the isolated tubal segment (Fig. 30–3B). The tube is ligated and then is suture-ligated on each end with 3-0 Vicryl or polydioxanone (PDS) double-armed sutures. The segment of tube is cut out and sent to pathology for diagnosis. The sutures are cut close to the knot on the distal (fimbriated) end. The two sutures are held with needles on the uterine end (Fig. 30–3C
Tubal Sterilization


Modified Irving Procedure
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


