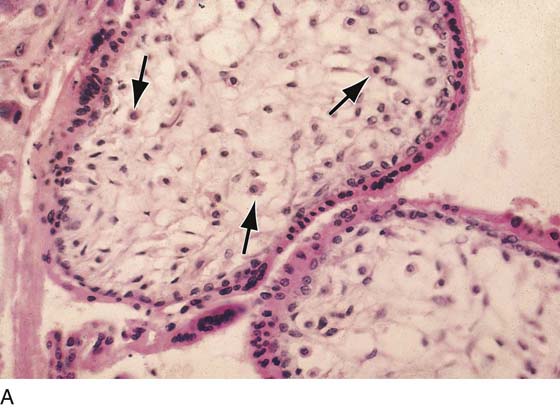
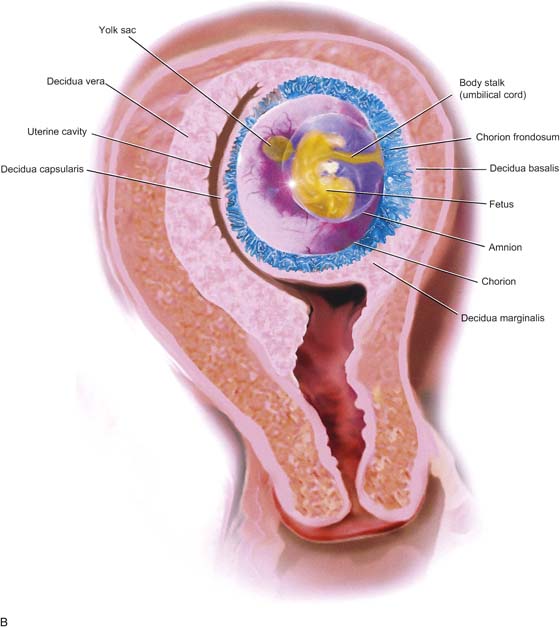
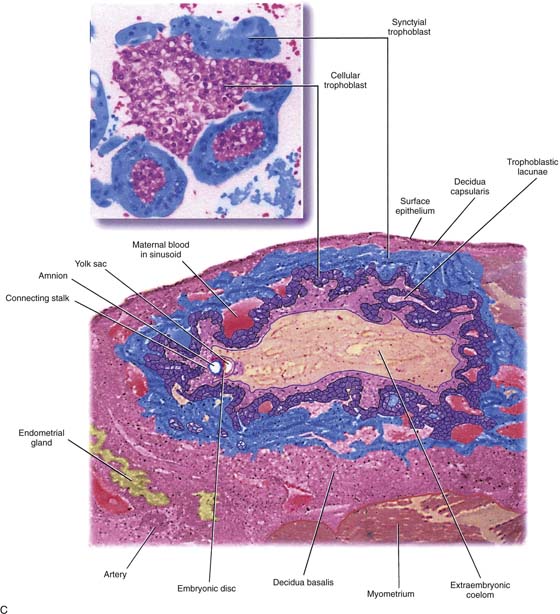
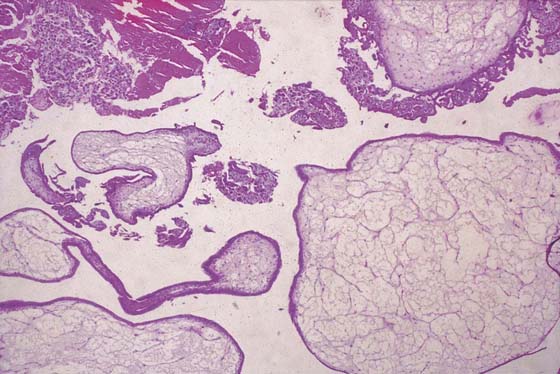
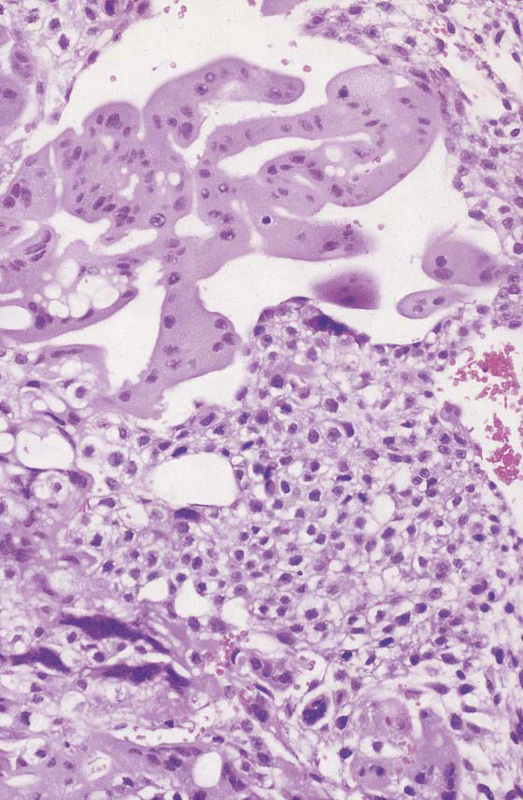
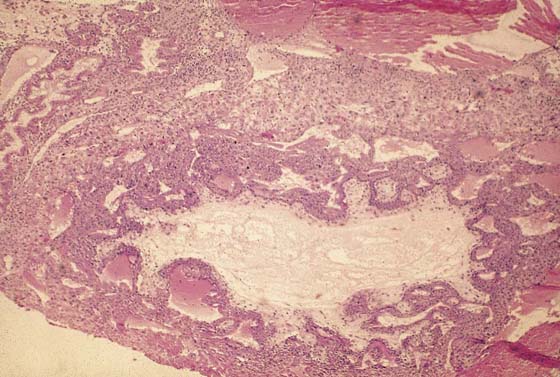
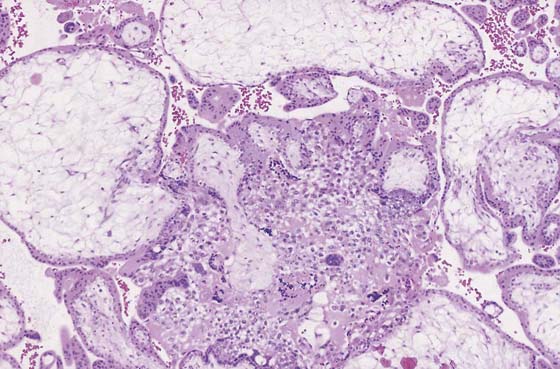
CHAPTER 21 Understanding the process of normal implantation and the development of villi together with the role played by the trophoblast is essential for similarly comprehending aberrations caused by abnormal trophoblastic generation (Figs. 21–1 through 21–3). Anatomic, microanatomic, and physiologic changes create a spectrum of disorders referred to as trophoblastic disease. Trophoblastic disorders may be divided into benign and malignant categories (Table 21–1). In developed countries (e.g., North America, United Kingdom, Western Europe), the incidence of hydatidiform mole is 1 : 1000 pregnancies, and choriocarcinoma is seen in 1 in 30,000 pregnancies. In the Far East, the number of molar pregnancies is 3 to 10 times greater, and the risk for choriocarcinoma is 10 to 60 times greater. Moles are subdivided into complete or partial. Complete moles are characterized by extreme villous swelling (hydropic change), trophoblastic hyperplasia, and paucity of fetal blood vascular channels (Figs. 21–3 through 21–6). Complete moles result from a single 23 X sperm fertilizing a defective ovum that contains no maternal genes. As a result of subsequent endoreduplication, the mole contains 46 XX chromosomes. In the case of partial mole, two sperms fertilize an egg with 23 X chromosomes, creating a triploid mole containing 69 XXX chromosomes (Fig. 21–7). Diagnosis is considered by a high index of suspicion based on clinical signs and symptoms of vaginal bleeding, hyperemesis, excess uterine size for gestational age, early-onset pre-eclampsia, hyperthyroidism, and intrauterine infection. The diagnosis is confirmed by viewing a passed molar vesicle, by pelvic ultrasound, by obtaining serial rising levels of serum and urine human chorionic gonadotropin (hCG), and by the presence of theca-lutein cysts (Fig. 21–8). FIGURE 21–1 Early implantation site. The deeper pink tissue is trophoblast, which is invading the decidua (light pink). Note the endometrial gland to the far left. FIGURE 21–2 A. Immature villi have two layers of trophoblast surrounding the villous connective tissue core. The outer, deep pink layer is syncytiotrophoblast, whereas the inner layer is cytotrophoblast. Note the open villous vascular channels and the Hofbauer cells (arrows). B. Trophoblastic cells make up the chorion and the villi, that is, the major part of the placenta. In this picture, the chorionic tissues are shown encapsulating the developing embryo and amnion. Major invasion and development of villi occur at the decidua basalis. The peripheral chorion frondosum will atrophy to form the bald chorion (chorion laeve). C. Physiologic trophoblast exhibits many of the characteristics of the premalignant and the malignant trophoblast. In this illustration, a trophoblast is shown to invade the maternal endometrium, open up maternal blood sinuses, create vacuoles, form blood lakes, and form primitive villi. The inset shows cores of cytotrophoblast being surrounded by syncytiotrophoblast. Strikingly normal trophoblast does not destroy the maternal tissues during the invasive process, whereas malignant trophoblast creates widespread necrosis. FIGURE 21–3 Well-developed, magnified view of a complete hydatidiform mole. The molar vesicles are fluid-filled distended villi. They can break off the main stem and be passed to the outside via the vagina, in which case the diagnosis of mole can be made with certainty. In the case of hydatidiform mole, no amnion is formed; therefore, direct entry and egress between the vagina and the uterine cavity exist. FIGURE 21–4 Low-power view of distended, hydropic villi clustered around masses of trophoblastic cells. FIGURE 21–5 Higher-power photomicrograph shows hydropic villi, absence of fetal vessels, and trophoblastic hyperplasia—three elements necessary to diagnose hydatidiform mole. FIGURE 21–6 High-powered view of trophoblast shown in Figure 21–4
Trophoblastic Disease
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


