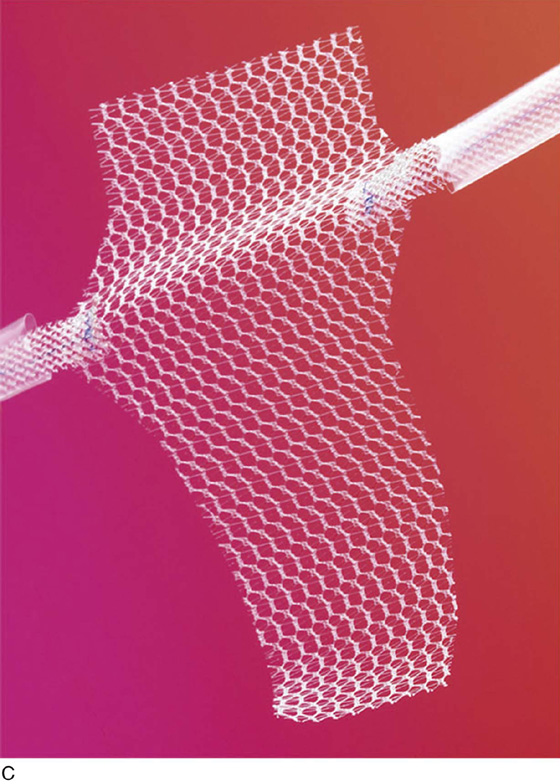
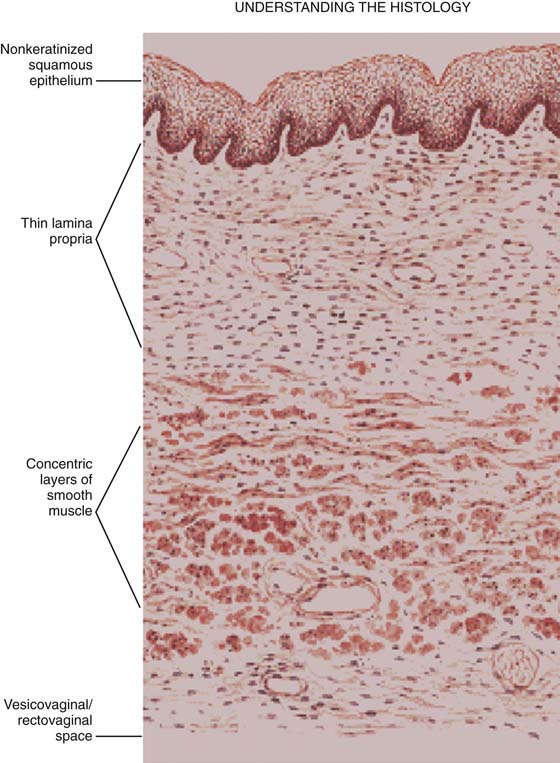
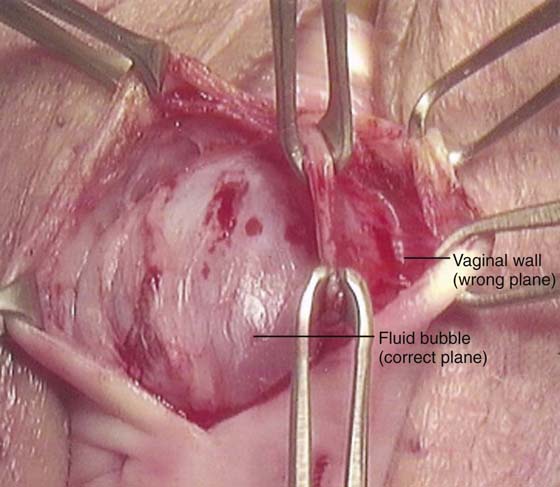
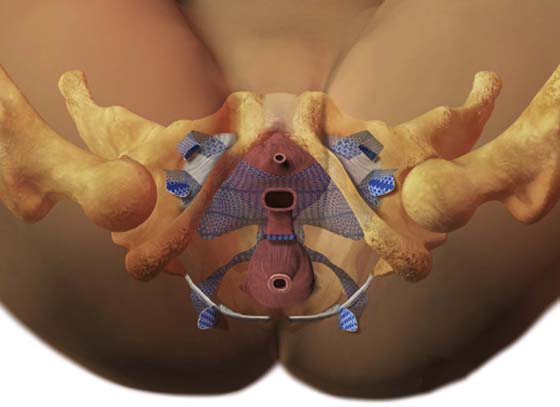
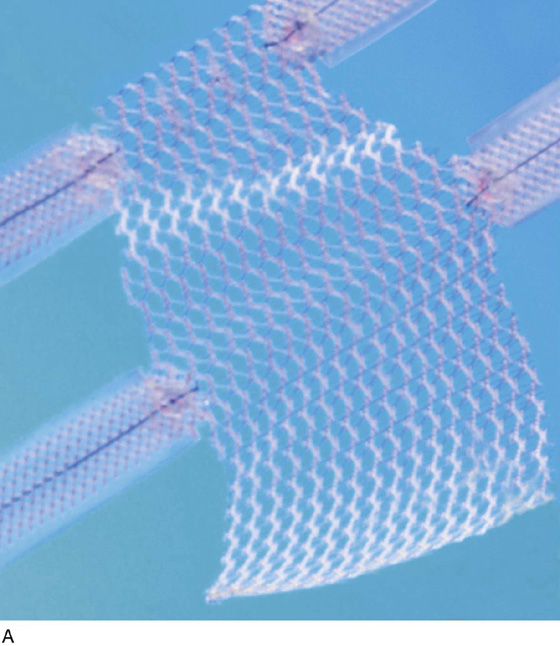
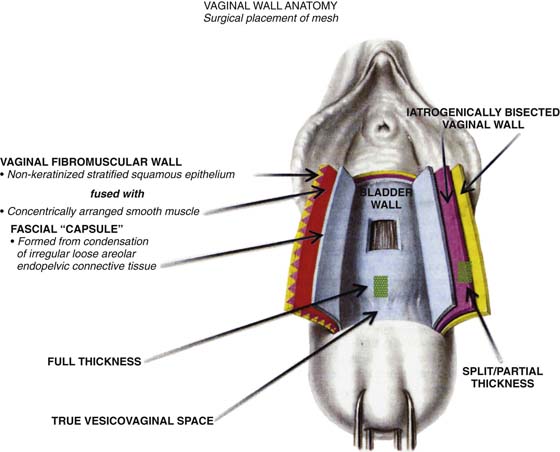
CHAPTER 57 Vincent Lucente Some surgeons believe that for many patients, native connective tissues are inadequate for successful long-term results in reconstructive pelvic surgery. Recently, meshes have been developed with the hope of meeting the unique requirements for use in the vagina. Innovative tension-free approaches to the placement of these meshes have been described in the hope of facilitating successful surgical outcomes while maintaining a minimally invasive surgical approach. The most commonly utilized mesh kits for prolapse are the Prolift system marketed by Ethicon Women’s Health and Urology (Fig. 57–1), the Apogee and Perigee Systems marketed by American Medical Systems (Fig. 57–2), and the Avaulta System marketed by Bard. These kits make use of an optimal mesh material (polypropylene) and an innovative trocar-based delivery system designed to facilitate tension-free placement. This chapter describes techniques used by the authors for placement of these systems. Patients undergoing pelvic reconstructive surgery via a transvaginal mesh system require appropriate and standard preoperative medical clearance, especially those patients at increased risk for operative adverse events, such as those resulting from fluid shifts, blood loss, susceptibility to infection, or impaired wound healing. Additional unique considerations must be carefully reviewed before a transvaginal mesh procedure is performed. Perhaps most important, as for many surgeries, is the provision of a very clear and understandable informed consent process. As with all evolving newer technologies and surgical procedures, one must have even a higher level of commitment to reviewing with the patient where in the development of evidence-based medicine (as well as your own surgical expertise) the surgical technology currently exists. At our centers, we have developed dedicated consent forms specifically designed to clearly communicate to patients the nuances of undergoing these relatively new approaches to pelvic reconstructive surgery. We go to great lengths to explain definitions of the term experimental versus standard of care. We discuss that the surgery has indeed gone through the review process of the FDA and has stood the test of earlier observational and comparative trials and has developed a growing body of literature supporting the benefits, as well as defining the associated risks. We candidly discuss our own success rates, as well as complication rates, especially those related to exposure or erosion and de novo dyspareunia. We also stress with our patients that we have found relative risks such as younger age, a history of undergoing a prior reconstructive procedure utilizing any permanent material or suture, and the presence of chronic pain disorder (especially pelvic pain) to be associated with the possibility of developing new-onset pelvic pain or, more specifically, dyspareunia. Last, each patient is given the option of a more traditional suture repair of endogenous tissue, as well as the alternative of an open or laparoscopic abdominal sacral colpopexy. All of our patients receive appropriate thromboembolic precautions, a rectal prep, including an enema the night before and the morning of surgery, preoperative antibiotic prophylaxis utilizing a second-generation cephalosporin, and careful operative prep of the vaginal canal and surgical site. We recommend that patients receive preoperative topical transvaginal estrogen and encourage patients to continue to use transvaginal topical estrogen for an extensive period of time postoperatively. It is important that patients realize that to optimize sexual function and comfort, the vaginal lining itself should be kept as healthy as possible with the support of topical estrogen. FIGURE 57–1 The Prolift system (Ethicon Women’s Health & Urology). FIGURE 57–2 The Apogee and Perigee Systems. (Courtesy American Medical System, Inc., Minnetonka, Minnesota. www.AmericanMedicalSystems.com.) We believe it is our responsibility to position the lower extremities carefully in adjustable Allen-type stirrups. From the lateral perspective, hip flexion should be no greater than 90°, and the leg should be abducted such that the knee is not in line with the foot and the contralateral shoulder (Fig. 57–3). Even with careful positioning, some patients will experience muscle strain and discomfort caused by hip flexion. Therefore, we often recommend that our patients perform specific stretching exercises for several weeks before undergoing surgery. Patients are instructed to perform these exercises while lying in bed in the morning or evening. Patients are instructed to grasp their knee or behind the knee, then while flexing toward their chest as much as they physically can, they can gently rotate the leg laterally and hold that position for a count of 10 seconds. Since embracing this exercise as part of our routine preoperative care, we have anecdotally seen a significant decrease in patient complaints of hip, back, and leg pain associated with the exaggerated dorsal lithotomy position required for transvaginal mesh surgery. In the authors’ opinion, the most technically challenging aspect of placement of any of the transvaginal trocar-based mesh kits is performing the proper dissection. Traditional dissection involved with suture plication of endogenous tissue of the anterior or posterior vaginal wall involves “splitting” of the vaginal epithelium from the underlying muscularis, followed by various forms of plication of the muscularis layer, trimming of the redundant epithelium, and closure. This splitting dissection, if utilized with transvaginal mesh placement, will inevitably result in a significantly high mesh exposure rate. To emulate and achieve the same low exposure rate experienced with transabdominal placement of the pelvic mesh, the transvaginal approach must enter the same pelvic spaces, placing the mesh deep to all of the histologic layers and compromising the vaginal wall. The surgeon must be skilled at entering the true vesicovaginal space anteriorly, as well as the rectovaginal space posteriorly, and placing the mesh into these spaces, as opposed to within the vaginal wall (Figs. 57–4 through 57–6). This specific full-thickness dissection is accomplished by utilizing first a very precise hydrodissection, then careful sharp dissection, and is finally completed with blunt dissection into the paravesical and pararectal spaces. Anteriorly, surgical entrance into the vesicovaginal space can be difficult because the lumen of the space is extremely small. Given the minimal amount of fat that exists in this potential space, it is best viewed as a balloon with little to no air within the lumen, which must be carefully entered. Recently, we adopted the use of an 18-gauge Tuohy needle, which provides increased tactile and visual feedback for precise bevel placement, allowing proper fluid dissection and distention of the vesicovaginal space (Fig. 57–7). Our approach to entering this space involves the placement of two Allis clamps on the anterior vaginal wall approximately 3 to 4 cm apart, in the area corresponding with the most pronounced portion of the anterior prolapse. Very commonly, the inferior margin of the bladder can be easily palpated through the vaginal wall. With a gentle pinch, the bladder can be pushed cephalad, potentiating the space between the bladder and the full-thickness vaginal wall. A Tuohy needle is then utilized to enter the vesicovaginal space, while a point closer to the inferior Allis clamp is chosen and the needle is held perpendicular to the plane of the vaginal wall edge. The needle offers 5-mm colored segments to provide the surgeon with a measured visual reference, which aids in accurate placement. The needle is carefully advanced through the full thickness of the vaginal wall, which most often is approximately 5 to 7 mm. Commonly, a popping sensation is distinctly palpable as the rounded tip of the needle enters the true vesicovaginal space. With the needle bevel-faced ventral in a 12-o’clock position, fluid can be infused easily into the space, creating hydrodissection. We prefer a dilute solution of 0.25% marcaine with epinephrine diluted 1 : 1 with injectable saline. A 20-mL aliquot of the fluid is placed along the midline. Next, a standard needle is used to reenter the 20-mL fluid pocket and then is directed off midline laterally, while the needle is kept parallel with the lateral aspects of the anterior vaginal wall. A vigorous push of the syringe will help force fluid laterally, physically separating the underlying detrusor muscle from the overlying full-thickness vaginal wall. Next, the anterior vaginal wall is incised with a scalpel or with the use of electrocautery to enhance hemostasis. Extreme care must be utilized to ensure that the surgeon has penetrated through all of the histologic layers of the vagina and has surgically entered the previously established fluid pocket. Often, this fluid pocket appears as a silver-gray jelly-like space that often contains yellow wisps of adipose tissue, which are easily visible without magnification. The incision is extended for a total length of approximately 4 cm (Fig. 57–8). FIGURE 57–3 Patient positioning on the operating room table with hip flexion not greater than 90°. FIGURE 57–4 Histologic layers making up the vaginal wall. FIGURE 57–5 Diagrammatic representation of different layers of the vaginal wall for optimal placement of mesh. FIGURE 57–6
Trocar-Based Synthetic Mesh Kits Used to Correct Pelvic Organ Prolapse
 Patrick Culligan
Patrick Culligan

![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


