The following technique has two variations: the first variation is best used in type III fractures using suture passed through tibial bone tunnels, and the second variation is best used in slightly comminuted type IV fractures using suture securely anchored to the anterior tibia. The initial screw fixation in both is the same.
Initial Fixation—Bioabsorbable Compression Screw
Initial fixation of the fracture fragment using a bioabsorbable screw is performed through a midpatellar portal to permit proper screw alignment and fixation.
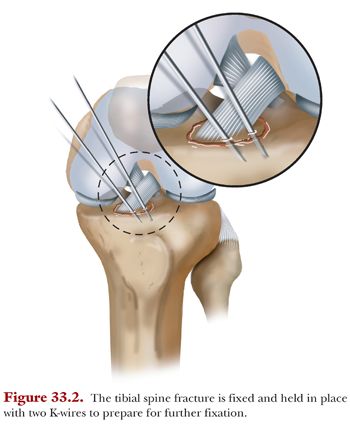
A 0.045-in K-wire is placed through the midpatellar portal in the desired location of the compression screw to stabilize the fracture fragment. A second K-wire is placed for additional fixation that will be maintained during screw placement (Fig. 33.2).
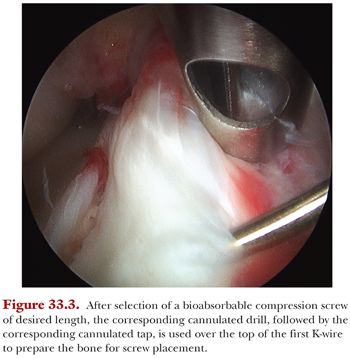
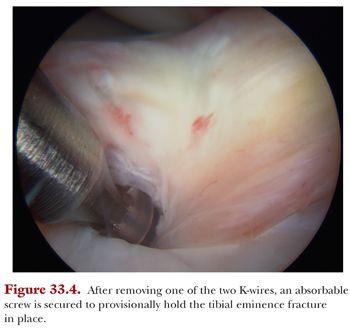
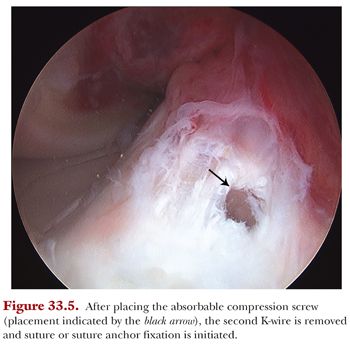
An incision for a portal is made around the first K-wire to accommodate a small arthroscopic cannula to prevent soft tissue obstruction. After selection of a bioabsorbable compression screw of desired length, the corresponding cannulated drill, followed by the corresponding cannulated tap, is used over the top of the first K-wire to prepare the bone for screw placement (Fig. 33.3). Because the drill and tap are cannulated while the bioabsorbable compression screw is not, to proceed, the K-wire used to drill and tap must be removed while maintaining fracture reduction. This is achieved by removing the first K-wire, with the second K-wire maintaining reduction, and replacing the removed K-wire with the selected screw (Fig. 33.4). Once the screw is implanted, the second K-wire is removed and the fracture is secure and stable (Fig. 33.5), allowing for easy reinforcement of the fixation with sutures.
Secondary Fixation—High-Strength Suture (Variation A for Type III Tibial Eminence Fractures)
With the fracture fragment secured in place by the bioabsorbable compression screw, secondary fixation is made more simple. Secondary fixation is completed using ultra high-strength suture, which is passed over the fragment, down two small bone tunnels, and tied over the front of the tibia.
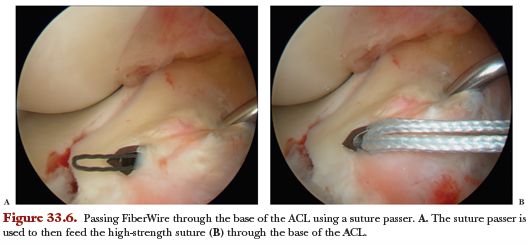
Two limbs of FiberWire (Arthrex, Naples, FL) are passed separately through the base of the ACL (running medial to lateral) using a suture passer (Fig. 33.6). Suture of different colors (FiberWire and TigerWire [Arthrex, Naples, FL]) can be used to help distinguish suture limbs.
An ACL tibial tunnel drill guide (Retrodrill Constant Guide [Arthrex, Naples, FL]) is then used to pass a 3-mm cannulated pin (Retrodrill Guide Pin, Cannulated [Arthrex, Naples, FL]) through the medial aspect of the fracture fragment at the base of the ACL insertion. FiberStick suture (Arthrex, Naples, FL) is passed up, through the cannula of the 3-mm pin, and retrieved through the medial portal using a grasper. The drill guide and cannulated pin allow for suture placement through the metaphyseal portion of the proximal tibia as well as the fracture fragment and the ACL. These steps are repeated to place a piece of high-strength suture, preferably of a different color than the first, through the fragment on the lateral side of the ACL. Then, both limbs of suture are pulled out through a single portal.
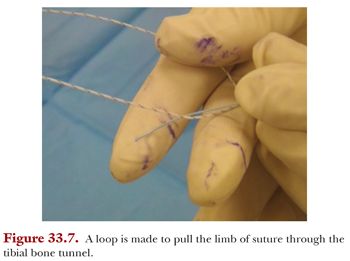
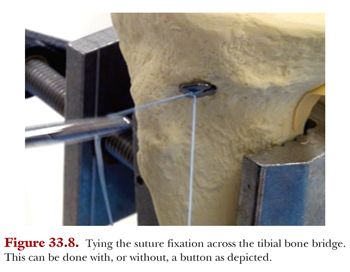
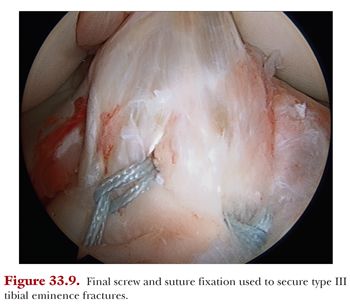
A loop is tied in one of the sutures (i.e., the solid suture) which is used to pull the other suture (i.e., the striped suture) down through the second bone tunnel (Fig. 33.7). The solid suture is then discarded and the striped suture is tied over the anterior bone bridge or a button (Fig. 33.8). Figure 9 is an image of the final fixation using this method with screw and suture fixation.
Secondary Fixation—High-Strength Suture (Variation B for Type IV Tibial Eminence Fractures)
In comminuted fractures of the tibial eminence, we have found that using a technique similar to basic shoulder labral repair, familiar to most arthroscopists and using the same equipment and fixation method, has been successful. After provisional fixation with a bioabsorbable compression screw, a high-strength suture fixation is achieved and secured with shoulder anchors.
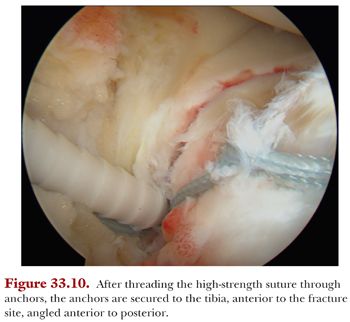
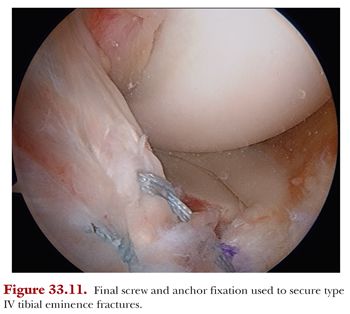
As described earlier (secondary fixation for type III tibial eminence fractures), use the midpatellar portals, using a suture passer to pass two limbs of high-strength suture through the base of the ACL (see Fig. 33.6), then through the anchors, and secure the anchor(s) anterior to the tibial eminence angled slightly anterior to posterior (Fig. 33.10). Figure 33.11 is an image of the final fixation using this method with screw and anchor fixation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


