FIGURE 42-1 A: Illustration of normal wrist anatomy with scaphoid (S), lunate (L), and triquetrum (T) noted. The TFCC and volar ulnocarpal ligaments are shown. B: Arthroscopic view of the normal TFCC in a right wrist viewed from 3-4 portal. C: Normal function of DRUJ ligaments in pronation, supination, and neutral positions of the forearm.
Pain is often diffuse (see Coach’s Corner). The opposite nonpainful wrist is used for comparison in all aspects of the physical exam. It is often best to start there, so the patient knows what you are going to do and establishes some trust. Specific locations (such as the ulnocarpal joint) can be diagnostic for anatomic injury (such as a TFCC tear). The presence of skin dystrophy and/or muscle atrophy is assessed before physical palpation or testing. Scaphoid, scapholunate, lunotriquetral, ulnocarpal, distal radioulnar, and volar radiocarpal joint areas are palpated in sequence. Palpation for ganglia in the usual locations (dorsal scapholunate, volar radiocarpal) is performed. Standard resistive strength (intrinsic and extrinsic), sensibility (light touch and two-point discrimination), and range-of-motion (passive and active) testing are performed on each patient to check for neuropathy, tenosynovitis,13 tendinopathy, and muscle injuries.14 Provocative testing for asymmetric ligamentous instability is necessary. Watson scapholunate shift, Lichtman midcarpal shift, lunotriquetral ballottement and shear, and ulnocarpal compression with forearm rotation are standard aspects of the exam. The presence of asymmetric clicking or clunking, particularly when it reproduces the patient’s pain, guides diagnosis. Injection of local anesthesia in the maximum pain area can be helpful, but many adolescents are resistant to needles. Ultrasound imaging of a mass can distinguish ganglia.

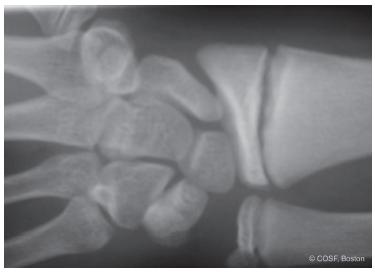
FIGURE 42-3 Radial stress injury in a gymnast.
Radiographs are obtained to assess for abnormalities such as physeal stress fractures (gymnast’s wrist),15 Kienbock’s avascular necrosis of lunate, unhealed fractures (scaphoid nonunion, hook of hamate nonunion,16 ulnar styloid nonunions and associated TFCC tears), carpal coalitions, and inflammatory arthritis, among others. Treatment is appropriately applied with each condition with a positive radiograph. With normal radiographs and a nonspecific exam, which is common, you are quickly at the crossroads of starting with the three R’s (reassurance, rest, and rehabilitation) or proceeding directly to an magnetic resonance imaging (MRI )scan or wrist arthroscopy. Unless the exam is specific for an anatomic injury, we always start with rehabilitation. Approximately 80% of our highly specialized referral practice fits that pattern and can still be successfully treated with resistive strengthening. It is rare we use casting for these patients but often use intermittent splinting programs. We use strengthening not only as treatment but also as a part of our evaluation. Grip-and-pinch strength on both sides is monitored by a therapist during intrinsic and extrinsic strengthening (elastic bands and therapeutic putty) with the wrist stabilized in neutral position. We stress the value of a home program that incorporates multiple sessions a day with weekly supervised care. We reassure them that there is a difference between “hurt” and “harm” and that we want them to work through the “hurting” pain without fear of causing permanent damage. If all goes well, by 6 weeks the patient will demonstrate marked reduction in pain and near-normal strength. By 12 weeks, the problem is often resolved.
If the problem persists, you then have to decide on more thorough musculoskeletal evaluation and treatment or referral to a pain specialist or nontraditional caregiver. The use of MRI scans can be diagnostic but also confusing depending on the threshold of signal abnormality the radiologist uses to make a reading.17–19 At our center, there are many more false negatives than false positives. The improving sequences narrow the gap of specificity and sensitivity but also make it imperative that we keep pace with the changing technology. The addition of arthrographic iodinated contrast material expands the diagnostic accuracy but, again, involves needles. In the remaining subset of patients with persistent problems, MRI scans often enable us, the patient, and the family to move definitively to surgery or away from orthopaedic interventions.
Surgical Indications
A limited number of adolescent patients presenting for evaluation of sports-related nonosseous wrist pain need surgery. As noted above, most can be treated with the three R’s: reassurance, rest, and rehabilitation. However, there are athletes with focal soft tissue and cartilaginous disorders that benefit from surgery. These include (1) scapholunate and lunotriquetral ligament tears;20 (2) chondral impaction injuries; (3) TFCC tears; (4) an unstable DRUJ; (5) arthroscopy for diagnostic dilemmas;21 and (6) rare, chronic tendinopathies. In addition, resection of the terminal branch of the posterior interosseous nerve at its insertion into the wrist can be a part of surgical management for chronic, recurrent conditions.
SURGICAL PROCEDURES
Do you know what my favorite part of the game is? The opportunity to play.
—Mike Singletary
 Ganglion Excision (Figure 42-4)
Ganglion Excision (Figure 42-4)
A dorsal ganglion, whether small or large, can cause symptoms with wrist arc of motion, especially dorsal impaction. However, not all ganglia are symptomatic. They can be associated with carpal instability, so excision alone may not resolve symptoms. They can be excised open or arthroscopically An open procedure is performed through a transverse incision over the dorsal ganglion. The origin of the ganglion is typically the scapholunate ligament. The dorsal veins and extensor tendons are protected with dissection. Circumferential dissection requires care not to rupture the ganglion before isolation of the stalk. Failure to remove the stalk is an invitation to recurrence. A square or circumferential dorsal capsulectomy is performed, incorporating the ganglion stalk. Some have advocated an inside-out removal of the stalk by opening the ganglion and following the stalk from the inside down to the origin. This is an open adaptation of the arthroscopic technique. After capsulectomy and stalk removal, the area of origin is debrided with a minirongeur and cauterized without impairing ligament integrity. The tourniquet is deflated to inspect for any bleeding. After local anesthesia injection and layered closure with absorbable suture, we usually immobilize in a bivalved cast or splint for 2 weeks followed by unrestricted activity. Stiffness and loss of strength are usually not a problem with these children. If they are ligamentously lax, we have them do a supervised strengthening program to eliminate that element of their pain as well.
Osterman and Raphael reported the arthroscopic removal of dorsal ganglia, and many now follow this technique.22 There may be cosmetic and rehabilitation benefits, especially in adults. Recurrence rates now appear to be similar, <5%.23 The scapholunate ligament, along with the rest of the joint, can be better assessed. The 3-4 portal cannot be used, as it is adjacent to or overlying the ganglion. The 4-5 portal is too close. Thus, visualization of the ganglia is with the arthroscope in the 6-R portal. A needle is placed from the dorsal skin through the ganglion into the radiocarpal joint. The needle enters the joint obliquely. An inside-out debridement is performed with the shaver in this modified 3-4 portal. The defect in the dorsal capsule and the ganglion stalk from the dorsal capsule to the scapholunate ligament is debrided. A complete capsulectomy is performed, and, afterward, the extensor carpi radialis brevis tendon should be visualized through the dorsal aspect of the capsule. Postoperative care is similar to open procedures but requires less time for wound protection and healing.
 Arthroscopic Debridement (See Sidebar) (Figures 42-5 and 42-6)
Arthroscopic Debridement (See Sidebar) (Figures 42-5 and 42-6)
Arthroscopy is the gold standard for diagnosis of intra-articular pathology. This is not to advocate for bypassing prudent physical exam, radiologic evaluations, and non-operative management of most children and adolescents with acute and chronic wrist pain. However, arthroscopy will provide definitive information on the interosseous ligaments, chondral articular surfaces, and TFCC and allow for surgical management of these specific problems not otherwise adequately treated.21,24
Adolescent athletes with ligamentous laxity can recurrently sublux their midcarpal and radiocarpal joints. This can occur in crew, tennis, and gymnastics, among others. Or, they can have a single subluxation episode with impaction from a fall, such as in soccer. In their mildest forms, these recurrent episodes produce mechanical symptoms and an inflammatory response. In the patient unresponsive to rest and therapy, arthroscopy often reveals synovitis, reciprocal impaction lesions of the volar lunate fossa and dorsal lunate with varying degrees of cartilage loss. There may be loose bodies. There can be a partial scapholunate tear and/or associated TFCC tear. Atraumatic debridement of loose bodies, synovitis, and loose cartilaginous flaps with mini-shavers is performed in standard fashion. If there is bare bone exposed, minimicrofracture is performed with thin angled bone picks. Immobilization in a short-arm cast for 2 to 4 weeks is followed by splinting and rehabilitation. We emphasize extrinsic strengthening to compensate for intrinsic ligamentous laxity. We do not perform dorsal capsulodesis procedures at initial arthroscopic debridement. Capsulodesis is reserved for recurrent injuries and static instability patterns.
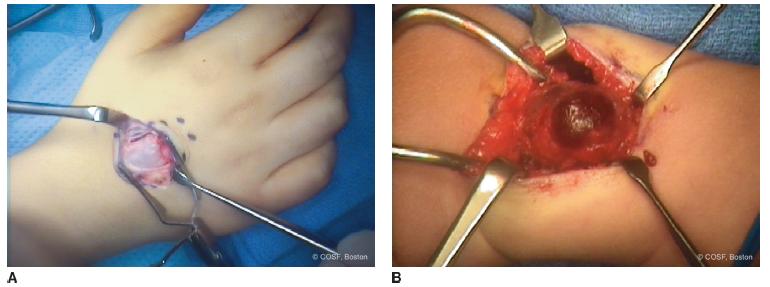
FIGURE 42-4 A: Dorsal ganglion excision. B: Hemorrhagic ganglion from repetitive trauma.
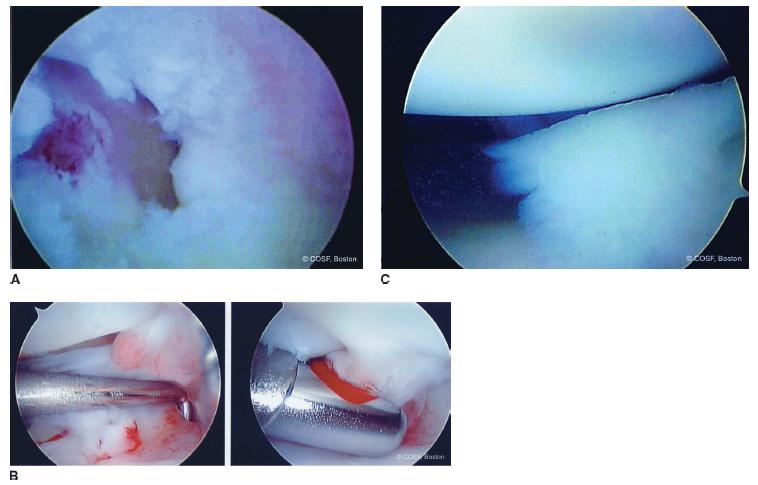
FIGURE 42-5 A: Chondromalacia of lunate and lunate fossa down to bare bone in an adolescent female crew athlete. Resection to stable edges and microfracture was performed. B: Reactive synovitis was debrided. C: Chondral loose body was removed.
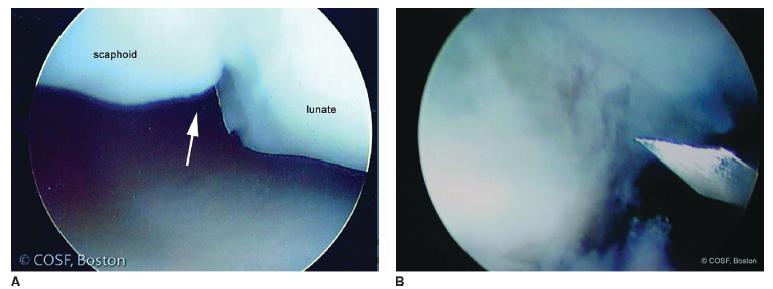
FIGURE 42-6 A: Partial scapholunate tear in athlete with chronic wrist pain. B: Drilling of osteochondral defect. There was associated chondromalacia and synovitis that was also debrided.
The stability of the scapholunate ligament is assessed from the 3-4 and midcarpal portals. The ligament is probed from the 4-5 portal with 3-4 visualization. From the midcarpal portal, the ligament should be tight without any step-off between the scaphoid and lunate. The lunotriquetral ligament is best seen from the 4-5 and midcarpal portals. It should be congruent from the 4-5 portal but can normally have a slight gap (1 mm or less) and incongruency from the midcarpal portal. Geissler developed an arthroscopic classification of interosseous ligamentous instability, graded I through I V. Type IV is a complete tear and requires ligamentous reconstruction. Types II and III have increasing dynamic instability and incongruency with a partial tear. Type IIs and the majority of type IIIs have been treated with successful arthroscopic debridement in adolescents25 and adults.26 The goal is debridement of the convex redundancy of the scapholunate and lunotriquetral ligament back to stable tissue without impairing the integrity of the ligament. With the scapholunate ligament, this can be performed with 3-4; 4-5; and midcarpal instrumentation and visualization. With lunotriquetral tears, this is performed with 3,4 (difficult visualization); 4-5; 6-R; and midcarpal surgery and visualization.27 Associated chondral lesions and synovitis are also debrided. We have not percutaneously pinned the carpal bones with carpal reduction as some have advocated. Immobilization is performed for 4 to 6 weeks followed by 6 weeks of rehabilitation.
 TFCC Repair
TFCC Repair
Athletes with chronic, ulnar-sided wrist pain, particularly with pronation and supination, should be evaluated for TFCC tears.28 In children and adolescents, most of these are associated with previous radius fractures, malunions, ulnar styloid nonunions, and/or positive ulnar variance.29 TFCC tears can also be seen in isolation. MRI can be diagnostic of the tear but not always; ulnar-sided TFCC injuries, in particular, may be difficult to characterize on MRI. Patients with unresolved pain and/or positive MRI scans should have arthroscopic exam and treatment. Any patient with an associated positive ulnar variance and ulnocarpal impingement should have a simultaneous ulnar shortening osteotomy. We do not advocate for wafer procedures in children and adolescents.
Palmer classified TFCC tears by mechanism30 (traumatic [I] and degenerative [II] and subtyped them by location—A = central [Figure 42-7]; B = peripheral; C = volar; D = radial). Most adolescent athletes have type IB peripheral tears followed less commonly by ID radial tears.31 Isolated tears are treated arthroscopically Tears associated with bone and joint deformity can be treated either open or arthroscopically depending on the situation and in conjunction with osseous reconstruction. Ulnar shortening osteotomy should be performed whenever there is a TFCC tear with positive ulnar variance.32 Arthroscopy can be easier and atraumatic after rigid internal fixation of an ulnar shortening osteotomy for marked positive variance.
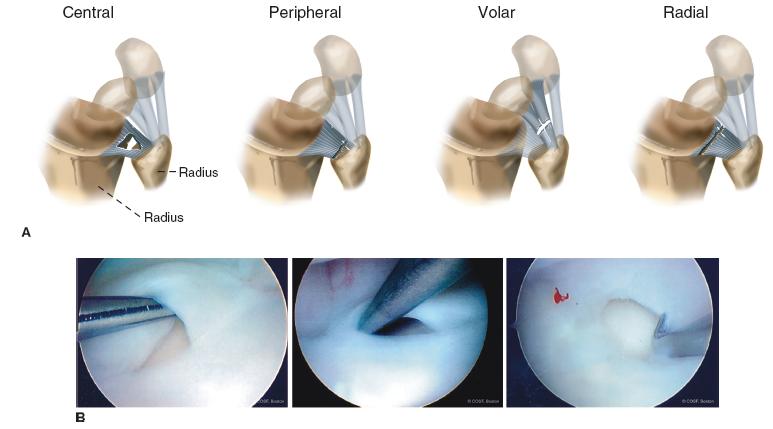
FIGURE 42-7 A: Traumatic tears are classified as IA = central (rare in children); IB = peripheral (most common type); IC = volar; and ID = radial (second most common in adolescents). B: Arthroscopic views of Central TFCC tears.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


