FIGURE 13-1 Clinical photograph of radial longitudinal deficiency with a rudimentary pouce flottant.
Evaluation of the radial deficiency starts at the chest wall and shoulder. Entire upper limb involvement does occur with both obvious and subtle differences.
Phocomelia with preaxial deficiency is the most involved case. Elbow range of motion is critical to treatment decisions. In the presence of a stiff extended elbow, extreme wrist radial deviation functionally substitutes for elbow flexion. In the absence of at least 90 degrees of elbow flexion, definitive correction of the wrist deformity is contraindicated.
The obvious deficiencies are in the wrist and hand. This condition can have profound limitations of (1) forearm length, (2) wrist stability and motion, (3) thumb development and function, and (4) digital motion and strength. Anatomic variations abound, and the degree of soft tissue anatomic abnormalities tends to indentllel the degree of osseous deficiency. Muscle deficiencies throughout the entire upper limb, but in particular in the forearm, wrist, and hand, include partial or complete absence, hypoplasia, abnormal origins and/or insertions, and/or fusion to adjacent muscles and accessory muscles. Brachial plexus, radial, ulnar, and median nerve anomalies have been well described.4 The median nerve is usually present but with aberrant anatomic course through the forearm and wrist. Vascular anomalies also are frequently present, and, again, the more deficient the radius, the more likely an abnormal radial artery and palmar arch.5 The spectrum of thumb deficiency ranges from mild hypoplasia to complete absence (Blauth classification). Digital involvement spreads from the radial side to the middle of the hand depending on the degree of preaxial osseous and muscle deficiency. Digital lack of motion is common and greatly affects function. The ulnar digits tend to have more developed joints, as well as intrinsic and extrinsic muscles, than the middle or radial side of the hand. Ulnar prehension is common. Very few of the more involved children can perform power grip and normal pinch activities. Spherical grip is most often used for functional grasp. The hand tends to be assistive rather than independent. Since 50% to 60% have bilateral involvement, this can be debilitating.
Osseous classification is by the amount of preaxial deficiency. Bayne and Klug classified this by types I through IV, from a minor deficiency in length to complete absence (I = short distal radius, II = hypoplastic radius, III = partial absence radius, IV = complete absence radius). James et al. added type O for radial carpal and thumb deficiency with a normal radius. We use a type V for elbow involvement and phocomelia. Unfortunately, type IV is the most common type, meaning those with this deformity have a lot of involvement. The osseous classification can be misleading because it focuses only on the radius and precludes thinking of the ulna, muscle, and soft tissue involvement. In types III and IV, the ulna is always foreshortened (at best 60% of normal length) and frequently bowed. The osseous classification can lead us to think simplistically. “If I only straighten the forearm, wrist, and hand, all will be well,” forgetting the profound degree of muscle and soft tissue impairment.
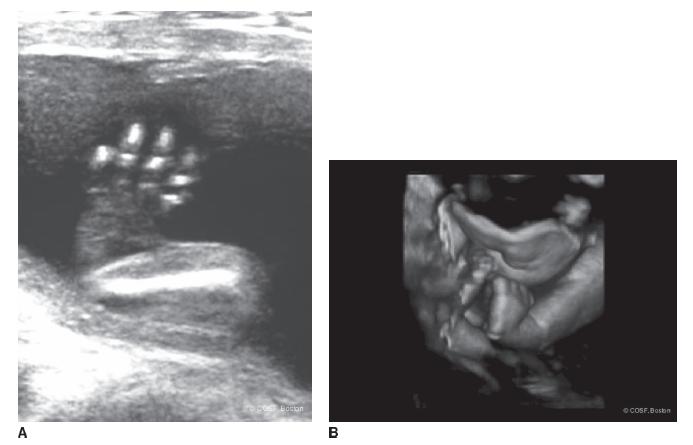
FIGURE 13-2 A: Prenatal ultrasound of severe radial longitudinal deficiency. B: A 3-D ultrasound of same patient. Clinical photograph of same patient shortly after birth is seen in Figure 13-1.
Treatment
Experience is that marvelous thing that enables you to recognize a mistake when you make it again.
—Franklin P. Jones
In all of congenital hand surgery care, at the present time there may be no greater variation and polarity of opinion than care of the severe radial club hand. A generation back, it appeared to be quite straightforward. Stretch the soft tissues with splints and/or casts early in infancy, surgically place the hand on the end of the ulna, and reconstruct the thumb. All in sequence during the first 1 to 2 years of life. Done deal. Unfortunately, as our partner Dr. John Emans says, “There is nothing that shakes your confidence as much as surgical follow-up.” Nowadays, there are the nihilists who almost believe in virtually no surgical intervention for type IV radial club hand and the optimists who believe that you use everything you have in your toolbox, including external fixation, lengthening, as well as microvascular bone and joint transfers. For the neophyte, even for the experienced surgeon, and especially for the parents, treatment selection can be confusing and daunting. The range of strong opinions makes for interesting debate but hard choices.
Nonsurgical
It is clear that the place to begin treatment is with stretching of the wrist from its malaligned position of radial deviation and flexion into extension and neutral to ulnar deviation. This can be by serial casting or by passive stretching many times a day and progressive forearm-based splinting of the wrist into a corrected position (Figure 13-3). With our skilled therapists, we tend to use progressive splinting and stretching followed by maintenance nighttime splinting in the first 6 to 12 months of life. For the mild type I or II radial deficiency, this is all the care that is needed for the wrist and forearm in infancy. They will correct and usually maintain their alignment throughout growth. If there is recurrent deformity, reinitiation of splinting and stretching is begun.
If the elbow is stiff in extension, a corrected wrist may impair hand-to-mouth, hand-to-head, and bimanual hand activities. Thus, most surgeons state that lack of elbow flexion is a contraindication to wrist surgery in radial longitudinal deficiency. We concur with that opinion.
Surgical Indications
Surgical intervention for radial club hand is for persistent wrist deformity that limits function. There is also the unspoken motivation to improve aesthetics. A well-designed and executed surgical plan will address the deficiencies in (1) wrist stability, (2) wrist alignment, and (3) forearm length. These often are not achievable in a single-stage procedure. Surgery does not come without a cost. For example, creating a straight, stable wrist may come at the cost of future growth of the ulna or wrist mobility and function. The more you strive to maintain or improve wrist motion, the more risk there is of recurrence. Ultimately, the functional outcome of any radial dysplasia patient, regardless of treatment, will be determined more by the quality of the fingers and thumb than the position and stability of the wrist.
Most of the time with more marked deformity, the stretching and splinting/casting precedes open or external fixation definitive surgical correction. The more difficult decision is what to do with a wrist, usually a Bayne type III or more commonly type IV deformity, that is uncorrectable by therapy, casting, and/or splinting. If it is extreme, most surgeons now progress to external fixation for soft tissue stretching and joint alignment.6–8 If the residual deformity is mild to moderate, many surgeons proceed to single-stage correction by open surgery. But there are some who do either a minimal soft tissue realignment with a bilobed flap9 or nothing, hence the controversy.

FIGURE 13-3 Static progressive splints, combined with therapist-assisted stretching, are used during the first 6 to 9 months of life to correct radial deviations of the wrist.
Well, boys, it’s a round ball and a round bat and you got to hit the ball square.
—Joe Schultz
 Centralization and Radialization
Centralization and Radialization
Classic treatment for longitudinal radial deficiency has been to centralize the hand over the distal ulna and stabilize the wrist in a single-stage procedure.10 A wealth of surgical experience for longitudinal radial deficiency came in the thalidomide crisis. All of the variations of procedures require extensive soft tissue rebalancing with releases, transfers, and capsular reefing. The amount of skeletal reconstruction differs. The extreme form of centralization (aligning the ulna and the third metacarpal) is the equivalent of a wrist arthrodesis by placing the distal ulna in a lunatecapitate carpal slot. This chondrodesis prioritizes wrist stability and alignment over motion and, ultimately, distal ulnar growth. A centralization procedure without a chondrodesis slot may involve a carpectomy or some distal ulna and carpal shaving to achieve alignment. This requires extensive soft releases and rebalancing to maintain correction. The goal of this modification is to maintain some wrist motion.11–13 The recurrence of radial deviation deformity, however, increases. A radialization (aligning the distal ulna with the second metacarpal) was advocated by Buck-Gramcko in order to maintain motion while lessening recurrence rate.14 This is done by increasing the ulnar deviation and extension static and dynamic forces.
There are also variations in skin incisions utilized. The most common are (1) radial Z-plasty and ulnar transverse ellipse,15 (2) dorsal wrist and forearm longitudinal S, and (3) bilobed flaps16 (Figure 13-4). We have used them all for different deformities and at various stages in our careers. Each allows for radial soft tissue release, rebalancing tendon transfers, and capsular reefing. The more severe the deformity, the bigger the incision we use to allow for the best repair with the least harm. Remember, the anatomy in these children is not normal and that in particular includes neurovascular structures. The more severe the radial dysplasia, the more likely the nerves and arteries will be anomalous or absent.
Case Scenario: Classic Centralization
The incision used in this particular case is a longitudinal dorsal S (Figure 13-5A). The skin and subcutaneous flaps are elevated extensively while preserving venous outflow. The extensor digiti quinti, extensor carpi ulnaris (ECU), and extensor digiti communis are isolated and protected (Figure 13-5B). These tendons can be very adherent to adjacent tissue and difficult to distinguish. The radial-sided anatomy is defined. The median nerve is usually displaced and taut. It needs to be protected. The radial artery may or may not be present. There may be an aberrant median artery. Release of fibrotic deforming forces is carefully performed. Tight musculotendinous units are released and tagged with sutures in case they can be transferred dorsoulnarly to improve dynamic stability. The volarradial wrist capsule usually needs to be opened and released for joint reduction and alignment. The dorsal ulnar capsule is opened in a transverse incision to visualize and stabilize joint reduction. The ECU is isolated. Care is taken to truly identify and enter the joint rather than plunge through the distal ulna or carpal cartilage. The articular surface and the distal physis are often oriented volar radially. The flaps are elevated while protecting the adjacent extensor tendons. Subsequent reefing of the capsule and ulnocarpal ligaments will help stabilize the ulnocarpal joint reduction. The ECU tendon is detached distally in preindenttion for advancement to improve dynamic joint stability (Figure 13-5C).
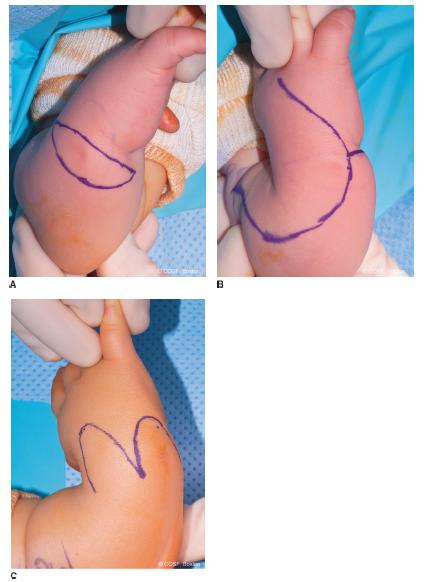
FIGURE 13-4 Clinical incisions used for centralization procedures. A: Ulnar ellipse to excise redundant ulnar soft tissues, used opposite Z-plasty incisions on the radial side of the wrist. B: Dorsal forearm and wrist “lazy S” incision with extension volarly and ulnarly. C: Dorsal bilobed flap incisions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


