Although early recommendations for treatment of symptomatic discoid meniscus consisted primarily of total or subtotal meniscectomy, our understanding of the role of the meniscus in load-sharing and stability of the knee has led to expanded indications for meniscal preservation and meniscocapsular repair. The lateral meniscus distributes up to 70% of the loads in the lateral compartment of the knee and plays a role in stabilizing the knee against rotational forces.1–3
Current strategies for the surgical treatment of symptomatic discoid menisci involve the creation of as normally shaped a meniscus as possible while stabilizing and preserving as much meniscus tissue as possible. A meniscus tear is addressed as indicated in the course of creating a more normally shaped meniscus. If the tear is in the midsubstance of a stable, completely discoid meniscus, simple saucerization is the treatment of choice. If the tear is at the periphery, repair should be undertaken. In the case of an unstable discoid meniscus that is not torn, saucerization is likely also required in order to provide adequate exposure for stabilization of the meniscus.
Saucerization involves removing the central tissue in a discoid meniscus. This is accomplished using arthroscopic biting and shaving instruments. The discoid tissue leaves less space than normal in the knee joint, causing difficulty with visualization and exposure. In addition, the patients are often young and may have very small knees compared to the average adult. In rare cases, the surgeon may even elect to use smaller arthroscopic instruments, such as the 2.7-mm arthroscope and the smaller arthroscopic biting equipment used in wrist, elbow, and ankle surgeries. However, discoid menisci consist of uniformly thick tissue rather than the central taper of a normally shaped meniscus. Although the discoid meniscus exhibits mucoid degeneration on histologic examination,4 it often maintains the thick, rubbery texture of an intricate collagen network. This abnormal collagen content can also be visualized on magnetic resonance imaging (MRI). Thus, smaller biting instruments may be inadequate to obtain control of the entire thickness. In order to be adequately prepared in a small patient, it is recommended to have both sizes of instruments and arthroscopes available. If a central horizontal cleavage tear is present, it can serve as an entry point for instruments to access the central portion of the meniscus and begin to taper it toward the periphery. A 70-degree arthroscope may prove helpful for visualization within the confined space.
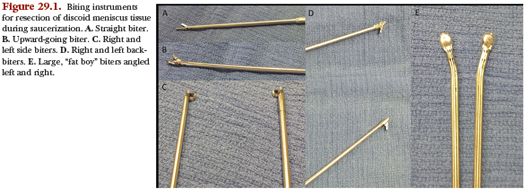
A typical set of arthroscopic biting instruments is shown in Figure 29.1. Straight and upward-going biters (Fig. 29.1A,B) are used through the ipsilateral portal to resect the posterior horn of the affected meniscus or through the contralateral portal to resect the body of the affected meniscus. The choice of straight or upward-going is dependent on anatomy and portal placement: A straight biter is ideal for the most central portion of the meniscal tissue, but any maneuvering around the femoral condyle might benefit from an upward-going biter. Right and left biters (Fig. 29.1C) are used through the ipsilateral portal to resect the body of the affected meniscus or through the contralateral portal to resect the anterior horn of the affected meniscus. For extensive resection of the anterior horn, a backbiter (Fig. 29.1D) should be available for use through the ipsilateral portal. The backbiter is not uniformly available in standard sets and must be requested specifically. Likewise, for very thick tissue, the large biter, or “fat boy” biter (Fig. 29.1E), should be requested in addition to standard instruments.
Portal placement must be carefully considered in order to reach the entirety of the discoid meniscus and achieve variable angles of approach. Initial viewing portal placement must be individualized to the patient’s size and relative location of the patella with respect to the tibiofemoral joint line. The anterolateral portal must not cause injury to the meniscus or the articular surfaces of the knee with instrument passage but must be sufficiently inferior as to allow access to the posterior aspect of the joint without injury to the femoral condyle. Once the arthroscope has been inserted into the joint, the anteromedial portal can be established under direct visualization, taking care to avoid injury to the anterior horn of the medial meniscus. An approach to the lateral meniscus from the medial side of the knee must allow clearance of the tibial spines, but it should not be so high as to preclude passage under the lateral femoral condyle. Localization with a small instrument such as a spinal needle prior to establishing the skin incision is recommended. Accessory portals, including the midpatellar portal and the posterolateral accessory portal, can also aid in visualization.
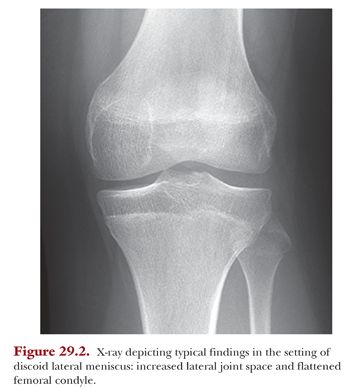
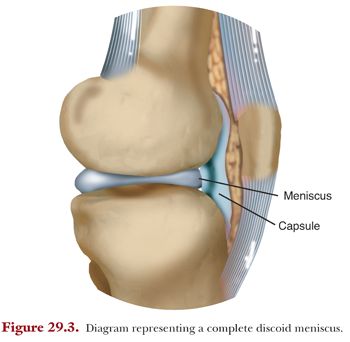
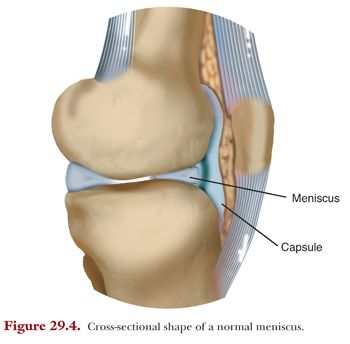
The amount of resection required to prevent continued impingement of the discoid tissue is a matter of some debate. Some surgeons recommend use of the curve of the lateral condyle as a guide, but the condyle adjacent to a discoid meniscus is known to have a larger average radius of curvature compared with a knee containing a normally shaped meniscus (Fig. 29.2—plain film of a knee with a discoid lateral meniscus). Others recommend leaving 6- to 8-mm rim of tissue in order to mimic a “normal” meniscus. In the case of a saucerized discoid meniscus (Fig. 29.3), however, this remaining rim is more of a trapezoid than the typical triangular tissue of a normal meniscus (Fig 29.4), and the implications of this increased remaining central thickness are unknown. At the minimum, the remaining meniscal tissue must have a stable rim, and dynamic assessment for impingement with range of motion can aid in intraoperative decision making.
Thermal ablation is a technique favored by some authors for contouring of meniscal tissue during adult meniscectomy. In pediatric patients, however, the proximity of the articular cartilage in the confined space of a compartment with a discoid meniscus makes the technique too high risk for tissue necrosis. If thermal instruments are used, we recommend using an outflow cannula in order to minimize the risk of elevated intra-articular temperatures.
In general, repair of a torn discoid meniscus and fixation of an unstable meniscocapsular junction should be suture-based. All-inside implants offer simplicity and speed compared to traditional inside-out or outside-in repair techniques, but they create larger defects in the meniscus with implant passage than do simple needles with suture. In pediatric patients in particular, small needles offer the advantage of multiple suture passes with minimal trauma, on both the femoral and tibial sides of the meniscus, in order to gain secure control of unstable and/or torn tissue.
Inside-out repair of the posterior horn and body of the meniscus and meniscocapsular junction requires an additional incision, generally on the posterolateral side of the knee. Vertical and horizontal mattress patterns may be used to obtain stable tissue fixation. The neurovascular structures are typically inferior to the trajectory of the needles on the lateral side of the knee, but care must be taken to avoid capture of the popliteus tendon as the sutures are passed. In the rarer circumstance of medial discoid meniscus, the saphenous nerve is at risk during inside-out repair of the posterior horn and body.
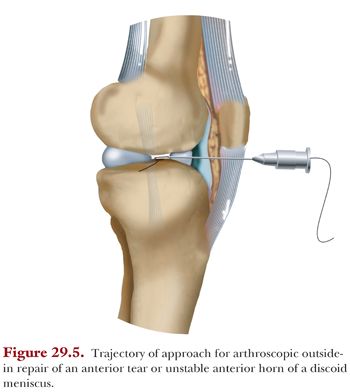
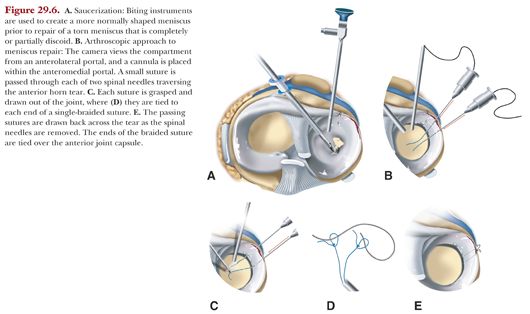
Because the interior of the knee is viewed from an anterior to posterior direction through the arthroscope, instability of the anterior horn of the discoid meniscus can be subtle and may be missed unless specifically investigated during the diagnostic portion of the procedure. Specific attention must be paid to this portion of a discoid meniscus, however, because the prevalence of instability has been reported to be as high as 53%.5 A probe or arthroscopic grasper can be used to exert pressure on the anterior horn, and instability is noted when the anterior horn of the meniscus displaces into the compartment. When the anterior horn of the meniscus is torn, or the anterior meniscocapsular junction is unstable, outside-in repair can be used arthroscopically. Figures 29.5 to 29.7 depict a technique for outside-in anterior horn repair: Two spinal needles are inserted through the meniscus from the anterior aspect of the knee at the level of the joint line. If the anterior horn is prone to flipping posteriorly during repair, traction sutures may be placed. When the anterior horn is successfully reduced, a shuttling suture is inserted through each spinal needle and drawn out through the arthroscopic portal using a grasper. A rigid monofilament suture of polydioxanone (PDS) or Prolene is easiest to push into the spinal needle. Care must be taken to ensure that no tissue bridge is interposed between the shuttling suture limbs—to avoid this, a cannula may be used or the shuttling sutures must be drawn out of the portal together. One limb of a braided doubled suture is then tied to each shuttling suture. The skin bridge between the spinal needles is incised, and the two suture ends are drawn across the anterior horn as the spinal needles are removed. The two suture ends are then tied over the anterior knee capsule, creating a mattress suture across the meniscus. If a vertical mattress suture can be managed within the available space, it provides a more even approximation of the meniscus to the capsule.

Discoid medial menisci have been reported sporadically in the literature, and their incidence is much lower than that of discoid lateral menisci. They should be treated according to the algorithm mentioned earlier, with an understanding that discoid medial menisci are more often stable than discoid lateral menisci, given their typically more robust capsular attachments. Like their lateral counterparts, torn discoid medial menisci often exhibit horizontal cleavage tears, along with anatomic changes within the medial compartment: widening of the joint space on x-ray, cupping of the medial tibial plateau, and even confluence of the medial meniscus with the anterior cruciate ligament (ACL) anteriorly.6–12
AUGMENTATION OF REPAIRED DISCOID MENISCUS
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


