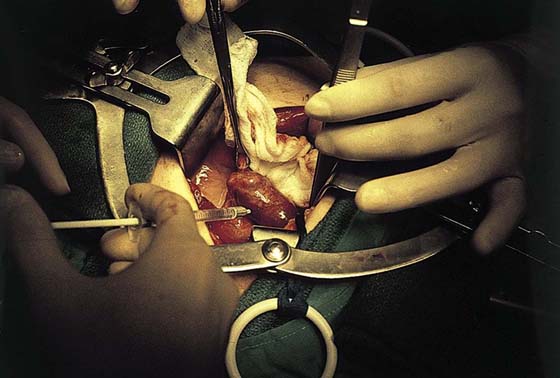
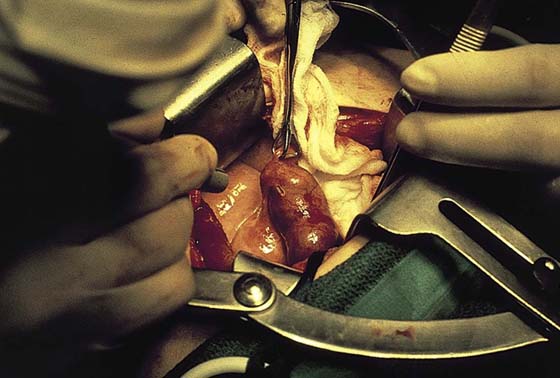
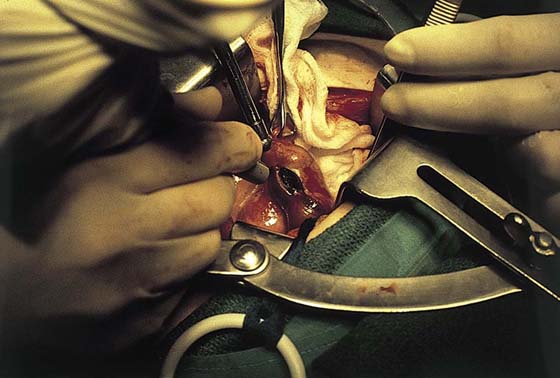
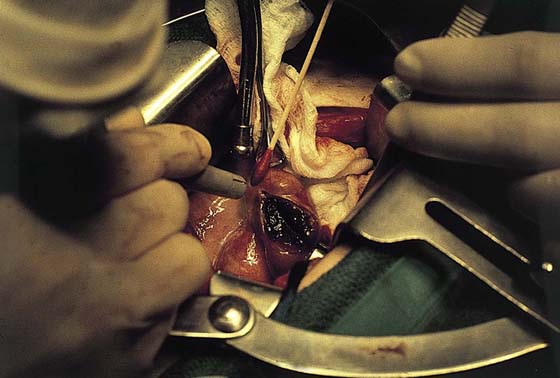
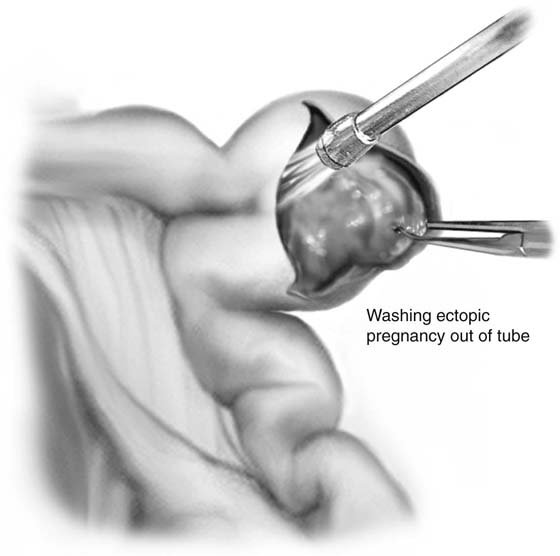
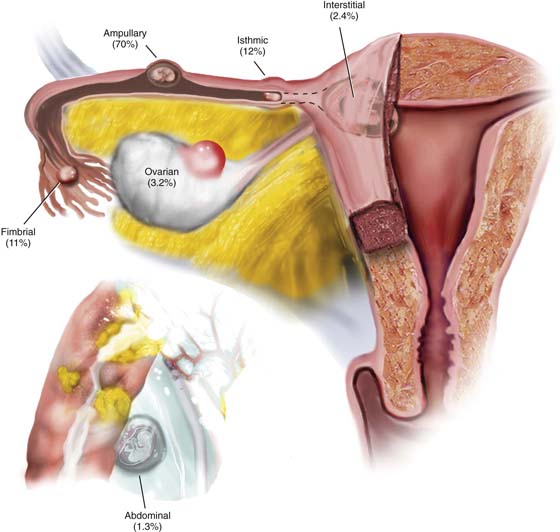
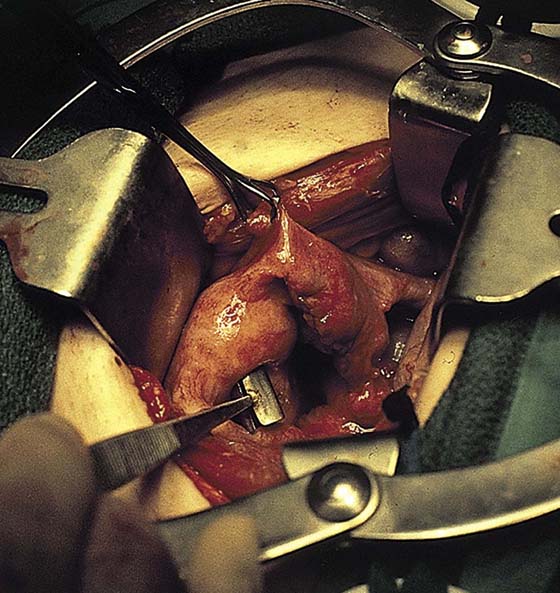
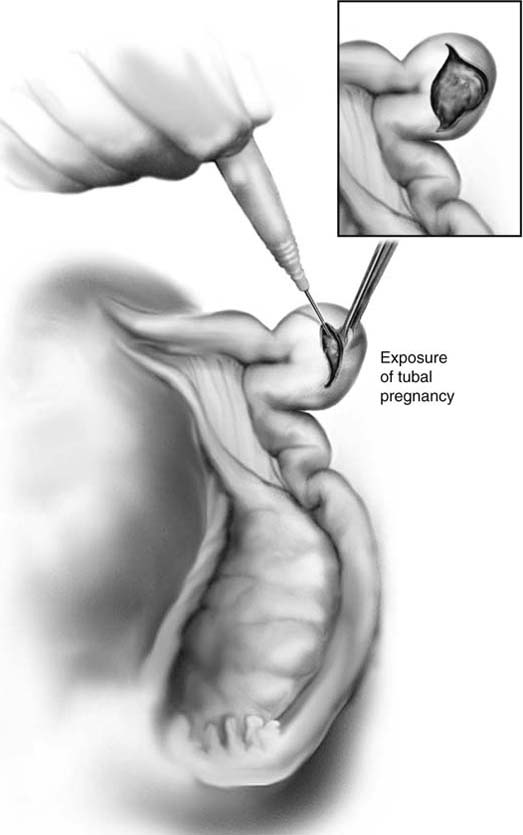
CHAPTER 26 Ectopic pregnancy may occur in a variety of locations. A vast majority of these occur within some part of the oviduct (Fig. 26–1). The goal of early diagnosis and prompt therapy is prevention of rupture and severe internal hemorrhage (Fig. 26–2). Although most tubal ectopic pregnancies are managed laparoscopically, certain circumstances may require laparotomy. These include large tubal pregnancies, rupture with substantial hemorrhage and hypovolemia, and cornual pregnancies. The open procedure for treating a leaking or unruptured tubal pregnancy is identical to the laparoscopic procedure. A linear salpingostomy is performed as the operation of first choice. If the tube has been severely damaged or if bleeding cannot be controlled, then a salpingectomy should be done. The affected tube is identified, as is the ipsilateral ovary (Fig. 26–3). Any blood in the abdominal cavity is evacuated. The contralateral tube and ovary are likewise examined for pathology. Next, the tube containing the tubal pregnancy is isolated via abdominal packs. A 1 : 100 vasopressin solution is injected (Fig. 26–4). It is wise to place traction (untied) stitches at either extreme of the bulging tube; alternatively, Babcock clamps may be applied. A trace incision is made on the antimesenteric edge of the tube with the use of an energy device (laser or electrosurgical) (Figs. 26–5 and 26–6). The incision is extended transmurally until the products of conception are contacted (Fig. 26–7). At this point, the pressure of the blood and clot expands the opening in the tube (Figs. 26–8 and 26–9). An irrigating probe is placed into the incision to facilitate separation of the products from the wall of the oviduct (Fig. 26–10). Traction is placed on the products, and the entire mass of blood, placenta, and embryo is removed (Fig. 26–11). The bed is irrigated (Fig. 26–12). The tube may be closed in one layer using 3-0 or 4-0 Vicryl, or the wound edges may be simply approximated and allowed to seal spontaneously (Figs. 26–13 through 26–17). FIGURE 26–1 This schematic drawing illustrates the various intra-abdominal sites and their relative frequencies for ectopic pregnancy. FIGURE 26–2 This ruptured ectopic pregnancy implanted on the mesentery of the ileum. When the abdominal pregnancy was diagnosed, the fetus had grown to 14 weeks’ gestational size. FIGURE 26–3 The right oviduct is grasped and elevated to reveal a swollen ampullary portion of the tube. FIGURE 26–4 The oviduct is injected with 1 : 100 vasopressin solution. The surgical site is injected to induce vasoconstriction. FIGURE 26–5 The antimesenteric surface is opened with an energy device (laser or electrosurgical) for purposes of hemostasis. In this case, a carbon dioxide (CO2) laser is used. FIGURE 26–6 The incision is linear and measures between 1 and 2 cm in length. FIGURE 26–7 As the tubal lumen is encountered, the pressure of the blood spreads the incision. FIGURE 26–8 Alternatively, an electrosurgical handpiece equipped with a needle electrode may be used to perform the salpingostomy. The net effect is similar to that produced by the carbon dioxide (CO2) laser. FIGURE 26–9 Typically, the tubal pregnancy presents as a large blood clot within the lumen. FIGURE 26–10 A small cannula is inserted into the incision, and the pressure of the irrigating solution dislodges the products of conception from the tube wall.
Surgical Management of Ectopic Pregnancy
Linear Salpingostomy for Tubal Ectopic Pregnancy


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


